 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Imtiaz Ali1* , Javeria Anees1, Faiza Hassan1, Rabiya Siraj1, Muhammad Ayub Mansoor1, Aiza Sohail Khan2
, Javeria Anees1, Faiza Hassan1, Rabiya Siraj1, Muhammad Ayub Mansoor1, Aiza Sohail Khan2
1Department of Radiology, Liaquat National Hospital and Medical College, Karachi, Pakistan
2Department of Dental and Maxillofacial Surgery, Liaquat National Hospital and Medical College, Karachi, Pakistan
Correspondence to: Imtiaz Ali, Department of Radiology, Liaquat National Hospital and Medical College, Karachi, Pakistan.
Received date: April 25, 2022; Accepted date: May 03, 2022; Published date: May 10, 2022
Citation: Ali I, Anees J, Hassan F, et al. (2022) Unusual Giant Calculus of Left Submandibular Duct. J Med Res Surg 3(2): pp. 41-43. doi: 10.52916/jmrs224075
Copyright: ©2022 Ali I, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted
use, distribution and reproduction in any medium, provided the original author and source are credited.
Sialolithiasis account for the most common disease of salivary glands. The majority of salivary gland calculi involve the submandibular duct and rarely in its parenchyma. This is common benign disease may cause the acute or chronic sialadenitis. Sialolith can be single, multiple, unilateral or bilateral. Patient can presents with history of swelling and pain. Giant sialolithiasis is not a common condition mainly occur in submandibular duct. Here we discuss the unusual giant submandibular duct calculus in adult male patient, its Computed Tomography (CT) scan appearance and post-surgical findings.
Salivary gland, Sialolithiasis, Submandibular duct sialolithiasis, Giant calculus
Sialolithiasis, it is common benign condition of the salivary gland [1]. Most of the salivary gland calculi occur in Wharton’s duct and submandibular gland parenchyma accounting for 80% of all salivary gland calculi. These are commonly involve the submandibular duct rather than gland parenchyma [1-3]. The salivary duct calculi are commonly less than 1.0 cm in size, only few of calculi reach the size greater than 1.5 cm and classified as giant Sialolithiasis [1]. Large calculi have been reported in literature and rarely seen [4]. Giant calculi are very rare and 95% reported in submandibular glands, almost all of them occurring in male patients [3]. There are causative factors for stone formation is salivary retention and depends on composition of saliva, the calcium concentration is higher in patients with Sialolithiasis then healthy individuals. Other risk factors includes higher viscosity of saliva may be due to chronic dehydration or secretory inactivity in some conditions, however the actual etiology is not known [3,5]. Radiological investigations used to diagnose the salivary gland calculi includes, Plain radiography, sialography, ultrasound, and CT scan, sialendoscopy [4,5]. There are many approaches to treat the Sialolithiasis, these includes extra corporeal short wave lithotripsy, sialo-endoscopy for smaller calculi and trans-oral sialo-lithotomy with sialodochoplasty or sialadenectomy is treatment of choice for giant calculi [5].
A 43 years adult businessman by occupation presented in outpatient department of dental and maxillofacial surgery with history of hard slow growing swelling in left submandibular region with occasional dull pain marked during oral intake of meal for last 6 to 7 years. On asking further history he had no known co-morbid and underlying chronic disease and he also denied the history of smoking, betel nuts, tobacco and alcohol consumption. On local examination, there was hard mass in left submandibular region, beneath the tongue on left side and non-mobile adherent to the surrounding structure. The intraoral mucosa was normal with no evidence of inflammation, induration, sinus or any patch. There was also no evidence cervical lymphadenopathy on either side of neck. During milking maneuver there was no evidence of salivation on left side at the site of opening of submandibular duct.
His radiographic examination was already done from outside our hospital revealed large radio-opaque mass along the inner aspect of left hemi-mandible (not shown here). We recommended the CT scan with contrast to rule the underlying neoplasm and acute or chronic infection. CT scan shows a large calculus in left submandibular duct within the floor of mouth along the left hemi-mandible. This is causing obstruction resulting in dilation of proximal submandibular duct and its intra-glandular branches. Left submandibular gland is mildly enlarged (Figure 1 and 2).
 Figure 2: (A) CT scan axial section with contrast shows dilated proximal
Wharton duct (white arrow) and calculus in left submandibular duct (black
arrow); (B) CT scan axial section with contrast shows dilated intra-glandular
ducts (white arrows)
Figure 2: (A) CT scan axial section with contrast shows dilated proximal
Wharton duct (white arrow) and calculus in left submandibular duct (black
arrow); (B) CT scan axial section with contrast shows dilated intra-glandular
ducts (white arrows)Patient was counseled, prepared and scheduled for elective surgery. After baseline investigations and general anesthesia fitness, patient underwent the trans-oral sialo-lithotomy with sialodochoplasty (Figure 3 and 4). The patient went through the smooth recovery with no drastic or minor complications on antibiotic and symptomatic treatment in hospital post-operative course and on follow up visit remained asymptomatic.
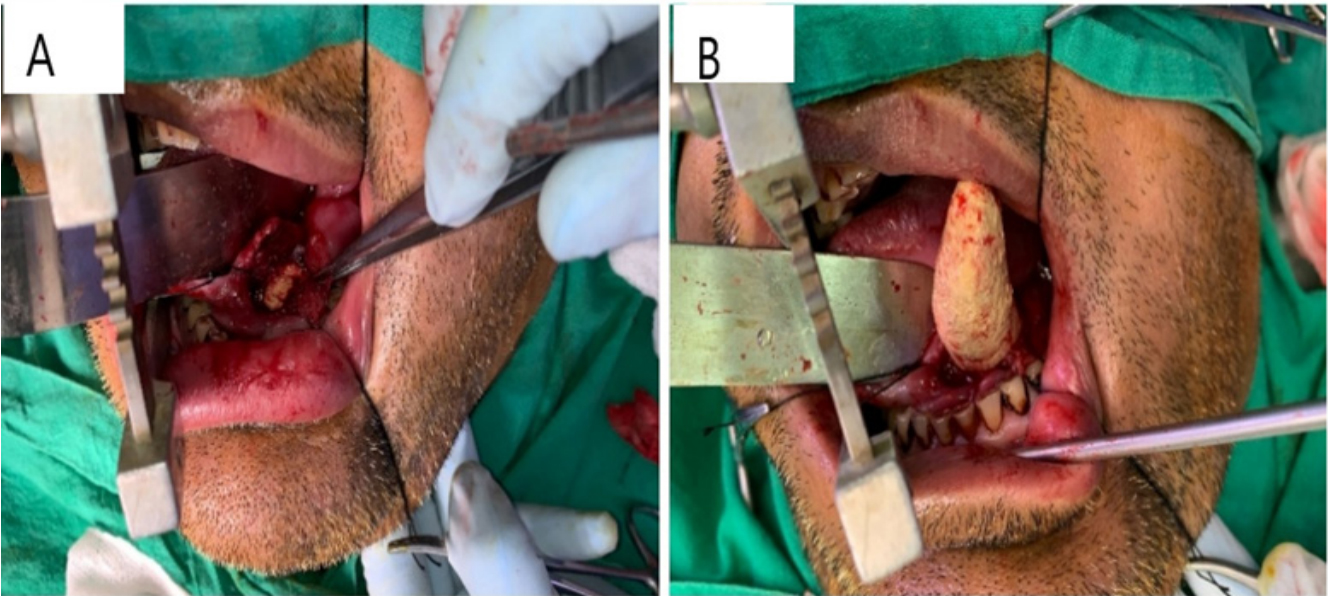 Figure 3: (A) CT scan bone window axial section; (B) CT scan with contrast axial section show large calculus in left submandibular duct (white arrow)
Figure 3: (A) CT scan bone window axial section; (B) CT scan with contrast axial section show large calculus in left submandibular duct (white arrow) Figure 4: A and B show removed calculus.
Figure 4: A and B show removed calculus.Submandibular gland are two in number present in submandibular triangle of floor of mouth which is formed by digastric muscles anteriorly and posteriorly and mandible inferiorly. They drain the saliva via the Wharton’s duct into the oral cavity. The gland is consist of large superficial and small deep lobe [4,5]. Sialolithiasis is common benign disease of salivary glands [1,3,6]. This condition can occur in any age group with more common in male adult. These calculi can occur in any salivary gland duct and their parenchyma but more common in Wharton duct. Giant sialoliths are rare with size varying from 1.5 cm or more [3]. Sialoliths are usually unilateral, oblong and round in shape, with irregular or smooth margins, vary in size and yellow in color [4]. Clinical presentation of salivary gland calculi is mild pain and swelling at the site of gland involved, however pain is usually increased with eating [4]. Giant submandibular calculi are very rarely present in routine clinical practice. The calculus with dimension more than 3 cm are extremely rare. Only few cases are reported in literatures [2]. In our case, we also reported on CT scan a very large unusual calculus measuring more than 4.5 cm in submandibular duct.
Etiology and pathogenesis of submandibular sialolithiasis includes several factors; these are flow of salivary gland secretions against gravity, the secretions are more alkaline in nature, submandibular saliva appears more mucinous, and has higher concentration of calcium and phosphate, Wharton’s duct is wider and longer with a kink over the posterior border of mylohyoid muscle. These all factors explain the preferential calculi formation in submandibular duct and its parenchyma [2-4]. Furthermore mineral salts, several local, mechanical and chemical factors are also involved in pathogenesis of salivary gland calculi [2]. One of literature postulated that, the cause of sialolithiasis is unclear, but there are two assumptions. First stated that inflammatory process in local area, this leads to mucus plugging with calcification, second stated that mineral salt deposition around the nidus of bacteria, mucus or desquamated cells [7]. Radiological investigations used to diagnose the sialolithiasis includes, conventional radiography, CT scan, ultrasound, sialography, and sialo-endoscopy [5,7]. The best view in conventional radiography is standard mandibular occlusal X-ray [3]. Sialography can be performed in patients in which conventional radiography not able to detect the calculi with less calcification. It is the technique in which low osmolar contrast is injected into the gland duct and visualized the entire ductal system. This is contra-indicated in acute infection and patient with contrast allergy. Non contrast high resolution CT scan is noninvasive and modality of choice for sialolithiasis [5,7]. A new method that has been overcome the conventional radiography is sialo-endoscopy, in which sialolith is directly visualized and can be removed. This is used for distal salivary gland ducts calculi [5]. Nowadays cone beam CT scan has been increasingly used in maxillofacial disease [7].
There are many methods for treatment of sialolithiasis, the minimally invasive techniques includes basket retrieval, lithotripsy, sialendoscopy, these techniques have good efficacy but with some limitation on infected or giant calculus for which sialo-lithotomy is preferred. if calculus is palpable on examination, regardless of its size, location, it is most crucial factor for successful removal [4]. In our case calculus was palpable, we have removed it successfully.
Sialolithiasis is common benign entity of submandibular gland. CT scan is modality of choice to diagnose the sialolithiasis, its extension, pre-operative assessment of stone its precise location, relationship with adjacent structures and associated complications. It is mandatory to diagnose and treat the patient early by surgical approach in case of unusual giant calculus to prevent the complications.
This case report was written and images of patient’s surgical and CT scan were added after taking consent from patient and patient’s identity is not shown here and will be kept confidential.
The authors declare no conflict of interest.
No funding or grant support.

