 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Julio Palacios-Juárez1*, Valdez-Díaz Brenda1, Sergio G. Moreno-Hernández3, Araujo-López Adan2 , Hurtado-Díaz Luisa Fernanda4, Paulina Cardona-Ochoa5
, Hurtado-Díaz Luisa Fernanda4, Paulina Cardona-Ochoa5
1Plastic Surgeon, Department of Plastic, Angeles Hospital, London Clinic, Mexico City, Mexico.
2Plastic Surgeon Resident, Department of Plastic, Angeles Hospital, London Clinic, Mexico City, Mexico.
3Department of General Medicine, Angeles Hospital, London Clinic, Mexico City, Mexico.
4Plastic Surgeon, London Clinic Hospital, Private Practice Mexico City, Mexico.
5Plastic Surgeon, Private Practice Mexico City, Mexico.
Correspondence to: Julio Palacios-Juárez, Plastic Surgeon, Department of Plastic, Angeles Hospital, London Clinic, Mexico City, Mexico.
Received date: January 23, 2024; Accepted date: March 5, 2024; Published date: March 12, 2024
Citation: Palacios-Juárez J, Valdez-Martínez B, Moreno-Hernández SG, et al. Easiest and Secure Surgical Treatment for Sialocele Post Bichatectomy: An Innovation Surgical Technique J Med Res Surg. 2024;5(2):25-28. doi: 10.52916/jmrs244132
Copyright: ©2024 Palacios-Juárez J, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted
use, distribution and reproduction in any medium, provided the original author and source are credited.
Introduction: Bichatectomy is one of the most common surgeries of the face, but in any of all the hands, it could be a complication, and the most difficult to treat is the Sialocele, so we made an easy way to treat it, and solve it.
Surgical Approach: We present a case of a young female, after the bichatectomy in the 5th day the middle face a Tumor, so we decided to create a new stenon duct, with a drainaige in anatomical position, getting a good result at the moment.
Discussion: The bichectomy has an important historical antecedent since in the beginning it was a surgery even without importance in the medical field. The removal of Bichat fat currently has more aesthetic than reconstructive purposes, so the increase of the Sialocele is more tan 3% independent the hands of the surgeon.
Conclusion: During the complications of bichatectomy, we decide to create an alternative for the surgeons that are in training, and an easy way to solve it.
Sialocele, Fistula, Bichaectomy, Surgical treatment, Tumor.
The Buccal Fat Pad (BFP) was described by the German anatomist Lorenz Heister in 1727 in his “Compendium Anatomicum” calling it “Glandular Moralis” (molar gland) for the first time [1]. He believed that it had no specific function, so from then on time more anatomists have been given the task of studying its function, embryology, and its relationship with the masticatory space [1].
Later in 1801, Marie-François Xavier Bichat French physician, surgeon and anatomist who described the BFP where he showed that it was composed solely of adipose tissue and located between the buccinator and masseter muscles and the skin [1,3]. He also mentioned that it is an independent structure of the adjacent.
In 1977, Peter Egyedi used for the first time the BFP as a pedicle flap with a skin graft for closure of oroantral and oronasal fistulas. Tiedeman in 1986 showed that a BFP flap epithelialized 3 weeks after placement [1-3].
Since then, BFP has not only been withdrawn to improve facial esthetics, but has also been used to reconstruct intraoral defects, but now is the a good options for aesthetic indication and have very good results, even the surgical approach, vestibular versus buccal, it is a good option to analyze, and we decide to made an study to analyze surgical approaches and compare, in our hospital, removing the buccal fat pad [3,4].
Anatomically the BFP is a tubular-shaped collection of adipose tissue that occupies a prominent position in the midface [2]. It has an average weight of 9.3 grams and an average volume of 9.6 cc [3]. Other authors divide the body of the BFP into three lobes: The anterior, posterior, and intermediate lobe. These three lobes are each encapsulated by an independent membrane, fixed by other ligaments and they vascularization by different arteries [2-5].
The vascularization of the BFP is derived from 3 branches of the maxillary artery: the deep temporal, buccal, and superior posterior alveolar arteries, also from branches of the facial artery. The venous drainage is provided by the facial vein [1,4 5].
The innervation of the BFP is provided by the facial nerve, in its buccal and zygomatic branches [5].
We present the case of a female of 23 years old, during the direct interrogatory she want a slim middle third of the face, no comorbidities, so we offer a bichatectomy.
The indications for these procedure would be patients with round face, middle third of the face with round mark of the buccal fat pad, and the contraindications for these surgery are patients with lot of comorbidities, with more of the fat under the cervical angle, than in the middle third, that patients need more than a bichactectomy.
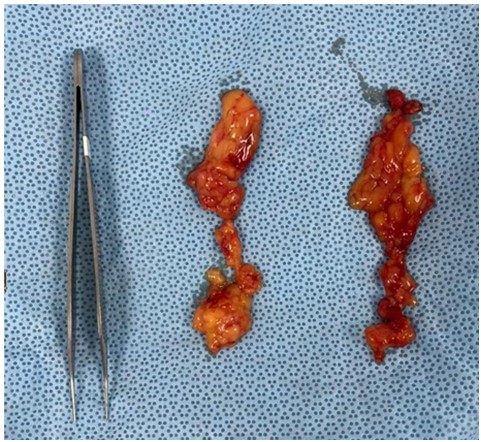 Figure 1: Fat Pad 3 cc from each side, without much blood.
Figure 1: Fat Pad 3 cc from each side, without much blood.We program the patient to the operation room, and did it with local anesthesia, the approach was by buccal incision, during the surgery was 20 mins long with 3 cc of the buccal fat pad (Figure 1), after the surgery everything was perfect, just pain in the scale of Analogic Pain in 7, so we discharge of the hospital.
During the 5 day of post-op (Figure 2), the patient went to the office with sweeling of the left check, with a minimum pain. We check over the internal vestibular check and we saw a tumor over the approach (totally closed) and with non-drainage over the Stenon terminal duct.
 Figure 2: Left side with the swelling at the 5-day post-op, increasing by days.
Figure 2: Left side with the swelling at the 5-day post-op, increasing by days. Figure 3: The material, the drainage that we use to the neoduct.
Figure 3: The material, the drainage that we use to the neoduct. 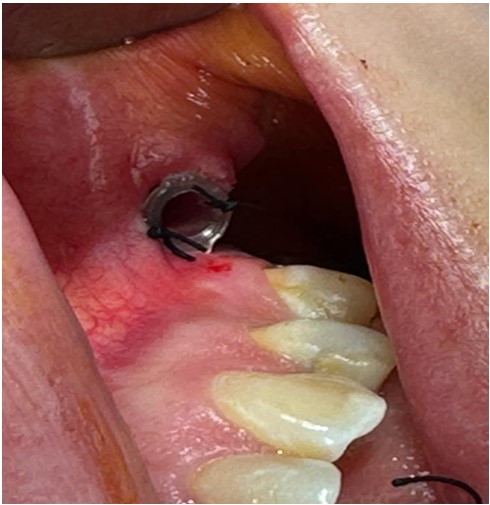 Figure 4: The neoduct with silf fixation.
Figure 4: The neoduct with silf fixation. The Surgical Treatment of this Sialocele diagnosticated, we give antibiotics, and prepare to the operating room, and with local and general sedation we reoperated surgically, previously with local anestesia where we think it is the stenon duck, clean with antiseptic lotion, we located just in the top of the tumor, with a Scalpel No. 11, we decided to explore it, and we did not saw the stenon duct, even the exploration was so deep with a mosquito forceps, by the previous approach, and then we decided to collocated a direct catheter (a syringe cap of 21 gauch blue color) to the top of the tumor, and instantaneously the gland begin to drainage saliva – creating a neostenon duct (Figure 3,4), and then tie with silk 4-0, by 4 stiches at each side, after the fixation where totally drained and the tumor decreases, we finish the procedure we use a gauze to clean, and finish the procedure. The patient went home with a liquid diet only for 72 hours, and review at the office, the tumor and the sialocele were drainage, and decided to leave the catheter for 10 days, after that the neostenon duct were fistulized, and the tumor was totally drained, and the sweeling of the patient was 90% cured (Figure 5,6).
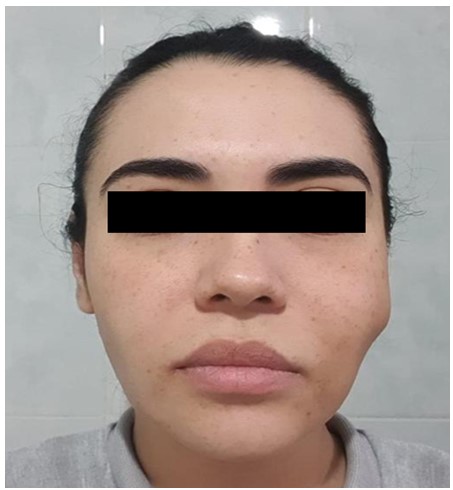 Figure 5: 1 day post-op of the follow up of the surgical drainage with our technique.
Figure 5: 1 day post-op of the follow up of the surgical drainage with our technique. Figure 6: Left Side View at 1 day post-op of the follow up of the surgical drainage, the asimetry.
Figure 6: Left Side View at 1 day post-op of the follow up of the surgical drainage, the asimetry. The follow up of the patient at the 15 days of the second surgery, was totally cured and with a good aesthetic result and the total recovery at the 3 months, the patients did not need any other instructions for the follow up of the drainage (Figure 7).
 Figure 7: The Initial and the follow up of the patient at 3 months after the bichatectomy and the sialocele surgical treatment.
Figure 7: The Initial and the follow up of the patient at 3 months after the bichatectomy and the sialocele surgical treatment.The Buccal Fat Pad has historically been removed to improve facial aesthetics, it has also been performed to reconstruct intraoral anatomical defects, and currently it is an excellent option for aesthetic improvement and with very favorable results, in addition, thanks to the studies that have been carried out, They have different surgical approaches as a resource for adequate removal of the buccal fat pad [1].
The BFP has different functions, in the infant, it prevents retraction of the cheeks during sucking and improves intermuscular movement. The shape and function of the buccal fat pad change considerably with age, its suctorial function and its volume in relation to the surrounding structures decrease over time, it can be concluded that different functions are attributed to it, including suction, it contributes to mastication, protection and cushioning of the neurovascular bundles, separation of the muscles of mastication from each other and aesthetics [1,2].
Anatomically, the BFP is fatty tissue wrapped by a thin layer of connective tissue, with a pyramidal shape, it is found in the genian, temporal and infratemporal regions, reaching deep to the pterygopalatine region, it is distributed in the masticatory space, separating the chewing muscles [3].
The BFP is fatty tissue found in the deep facial spaces. It is located behind the zygomatic arch. There are four processes, the pterygoid process, the superficial process, the buccal process, and the deep temporal process that extend from the body to the surrounding tissue spaces such as the infratemporal space and the pterygomandibular space [3]. The BFP is divided into three lobes, posterior, intermediate and anterior, according to the structure of the lobar covers, the ligaments and the vessels that supply it. The buccal, pterygoid, pterygopalatine, and temporal extensions are derived from the posterior lobe. The BFP is fixed by six ligaments and supplied by various vessels. The buccal BFP's function is to fill deep tissue spaces and function as a sliding pad, as a cushion in muscle contraction and to drive external force. Relaxation, poor development of the ligaments or rupture of the capsules could cause prolapse or fall of the oral extension [4].
Stuzin, et al. made findings based on 12 fresh cadaver dissections (6 samples). All the bodies were over 60 years old at the time of the autopsy. In all their dissections, the anatomical relationship of the BFP within the masticatory space and with the facial structures was constant. The weight of each fat pad averaged 9.3 g and the volume, as measured by water displacement, averaged 9.6 c). There is a small variation between the right and left sides and the total weights were on average 1.5 g in all samples. No considerable relationship was found between the size of buccal fat and the general adiposity of the corpse. Their findings demonstrated that cachectic specimens with little subcutaneous fat had buccal fat pads of normal volume and weight [4,5].
In recent years, the number of procedures for removing BFP for aesthetic purposes has increased, which can be performed by both the dentist and the plastic surgeon. Patients who are candidates for this surgical procedure usually have excessive facial circumference, and in some cases, tearing of the buccal mucosa tissue secondary to constant bites in the same site [5].
Bichectomy is a surgical procedure performed with the aim of improving the contour of the cheeks, highlighting the malar eminences by reducing their prominence. It is a very useful tool performed in facial aesthetic surgery, which can generate important complications, including: immediate post-operative hematoma, facial paresis or paralysis, abscess, stenosis of the Stenon duct, facial asymmetry and sialocele, so it is of vital importance that it is carried out by a professional with skills and expertise [6].
Complications such as excessive scarring and contracture, persistent trismus, change in cheek contour, or flap failure have been associated with excessively large BFP harvest and larger defects [6].
Buccal depth obliteration is usually a temporary phenomenon, commonly when the BFP is directed through an oral subperiosteal tunnel with the aim of closing an oral antral fistula in the first molar area. As the fat is reduced and gradually replaced by other tissues, the vestibule tends to return to a more normal contour. Research has shown that harvesting the BFP flap does not negatively affect facial contour or vestibular depth, and facial aesthetics and function are maintained in a large percentage of patients [6,7].
Sialocele is an accumulation of saliva in the tissues surrounding the gland duct or in the parenchyma without drainage [7,8]. There are different etiologies: neoplastic, infectious, traumatic, ductal stenosis, the most common etiology is saliva extravasation, secondary to a disruption of the parotid duct or parenchyma due to sharp trauma [9].
Salivary fistula or sialocele is a wound complication that occurs in 5% to 39% of parotidectomies [8]. A salivary fistula occurs when the fluid is no longer contained and drains towards an epithelial surface, while a sialocele is an accumulation of saliva within the surgical site. It is thought that sialoceles are formed as a consequence of the alteration of the salivary parenchyma and the subsequent spillage of saliva into adjacent tissues. Research has suggested that sialoceles formation is associated with foreign bodies within the wound bed or the degree of parotid removal [10].
Bichat surgery has a scientific foundation in various issues, both aesthetic and functional [1] described that the approach maters more by vestibular as easiest. But complications after this common surgery are less than 10% in surgical hands. Nowadays non plastic surgeons, try to do this common surgery, but not with a good results, and the rate of complications like Sialocele increase, but that is not the problem, is that many of this are not well treat.
In this article, we try to teach to the plastic surgeon community a new, secure, and easy matter to treat this complications and the most important thing is that the aesthetic result does not change, one of the most feared of the patient and the surgeon.

