 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Satori Iwamoto* , Mason Johnstone, Michelle Chiu, Hillary Chu
, Mason Johnstone, Michelle Chiu, Hillary Chu
California Northstate University, College of Medicine, United States
Correspondence to: Satori Iwamoto, California Northstate University College of Medicine, United States.
Received date: March 27, 2022; Accepted date: April 06, 2022; Published date: April 13, 2022
Citation: Iwamoto S, Johnstone M, Chiu M, et al. (2022) Acute Ischemic Stroke in a Young Woman with an Otherwise Asymptomatic SARS-CoV-2 Infection. J Med
Res Surg 3(2): pp. 38-40. doi: 10.52916/jmrs224074
Copyright: ©2022 Iwamoto S, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits
unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
It was well-observed that SARS-CoV-2 may cause a hypercoagulable state in hospitalized patients. Often these hospitalized patients exhibit severe upper respiratory symptoms with hypoxia, requiring high amounts of oxygen support. In this study, we report a young healthy 30-year-old woman with no medical problems, who experienced an embolic stroke due to an otherwise asymptomatic SARS-CoV-2 infection in July 2020.
The patient presented to the emergency department after experiencing sudden slurred speech, dizziness, and acute left leg weakness during a social gathering on a river boat the day prior to admission. She also vomited once, non-bilious. The patient had no upper respiratory symptoms and had not been practicing social distancing nor wearing a mask. She did not have any sick contacts or significant travel history. Patient used oral contraceptives but never smoked.
The workup included a Computed Tomography (CT) angiogram, an Magnetic Resonance Imaging (MRI) and an Magnetic Resonance Angiography (MRA) of the brain. It was significant for acute stroke with acute intraluminal thrombus causing partial occlusion of the distal basilar artery with left pontine stroke. Given that the onset of symptoms was greater than 4 hours, she was outside of the tissue Plasminogen Activator (tPA) administration window. Patient was also not a candidate for embolectomy as National Institute of Health Stroke Scale (NIHSS) was 3 and the occlusion was partial. SARS-CoV-2 PCR test was positive. D-Dimer level was elevated but CRP was normal. Echocardiogram was unremarkable. The patient had no history of autoimmune disorder. Patient was initially treated with antiplatelet medications aspirin and clopidogrel (Plavix). Her condition improved and she could ambulate with a front wheel walker and stand by to assist. She was discharged four days later with anticoagulation medication rivaroxaban (Xarelto) for 3 months.
This case illustrates that patients with an otherwise asymptomatic SARS-CoV-2 infection may still suffer from complications of SARS-CoV-2. Do women on oral contraceptives have higher risk of arterial embolism when infected with SARS-CoV-2? More study is needed.
COVID-19, Ischemic stroke, Hypercoagulable state, Case report, SARs-CoV-2, Oral contraceptive
Ischemic stroke is a frequent cause of disability and mortality. It can be a life-changing event for both the patient and family. Many hospitals in the US have dedicated stroke centers to treat patients with stroke. However, it is uncommon for young healthy adults to suffer from an ischemic stroke.
Epidemiologically, the majority of strokes (75%) happen at age 65 years or above [1]. For young adults, the risk factors for acute ischemic stroke tend to relate to congenital, metabolic and drug ingestions [2]. In the elderly, typical risk factors of hypertension, smoking, diabetes, and hyperlipidemia are the causes of ischemic stroke [3]. In the past 2 years, we have seen acute ischemic stroke as a complication of patients with severe SARS-CoV-2 infection [4]. However, it is uncommon to see stroke as the only presenting symptom for a young adult with an otherwise asymptomatic SARs-CoV-2 infection. According to the Helsinki study, viral infection is not a common cause of ischemic stroke in this age group of 15 to 49 years old [5].
Etiology of brain ischemia is mostly characterized by four categories: thrombosis, embolism, systemic hypoperfusion, and hypercoagulability [6]. First, thrombosis describes local obstruction of the artery. Examples are atherosclerosis, arterial dissection, and fibromuscular dysplasia. Superimposed thrombin may or may not be involved. Second, embolism describes an arterial blockage arising from elsewhere (aortic valve, or thrombus broken away from elsewhere). Third, systemic hypoperfusion refers to issues involved with the general circulatory system. Examples are hypovolemic shock, cardiogenic shock, and septic shock. Lastly, hypercoagulability occurs when a thrombus is more likely to form due to intrinsic pathology of blood, causing embolic stroke. In acute leukemic patients with hyperleukocytosis with White Blood Cell (WBC) approaching 100,000 per microliter of blood, there is an increased risk of ischemic stroke [7].
Hospitalized patients with severe SARS-CoV-2 infections are almost always immobilized. They are bed-bound, tethered to an oxygen delivering system (high flow, bi-level positive airway pressure, ventilation system, etc.) in order to stay oxygenated. It has been suggested that the spike protein of SARS-CoV-2 may activate the alternative complement pathway, and injure the endothelial cells in hospitalized SARS-CoV-2 patients [8]. Cytokine storms and Systemic Inflammatory Response Syndrome (SIRS) observed in hospitalized SARS-CoV-2 patients can definitely contribute to the hypercoagulable state. It is uncommon, however, for non-hypoxic ambulatory asymptomatic SARSCoV-2 patients to show signs of thrombosis.
In addition, use of combined estrogen-progestin oral contraceptives with concurrent smoking has been reported to increase the risk of arterial and venous thromboembolism [9]. On the other hand, the use of modern low hormone dose contractives alone do not seem to increase risk of stroke [10].
The patient is a young healthy 30-year-old woman with no significant past medical history who presented to the emergency department for sudden onset of left leg weakness, dizziness and slurred speech that began around 11:15 PM on July, 2020. She was with her friends for a social gathering on a river boat that night and was taking a group photo when they noticed her symptoms. She also vomited once, non-bilious. She was brought to the emergency department the following morning around 5:00 AM. She denied any head or neck trauma, and had not been practicing social distancing nor wearing a mask. She had no upper respiratory symptoms, did not have any sick contacts nor significant travel history. She has a history of using birth control pills but does not smoke. Initial physical examination showed mild dysarthria, no facial asymmetry, no obvious motor deficit, mild ataxia on right finger to nose test, mild altered sensation on the right, gait ataxia requiring assistance, and she scored 3 points on the National Institute of Health Stroke Scale (NIHSS).
The workup included a Computer Tomography (CT) angiogram, an Magnetic Resonance Imaging (MRI) and an Magnetic Resonance Angiography (MRA) of the brain, suggesting an acute intraluminal thrombus causing partial occlusion of distal basilar artery with left pontine stroke. MRI of the brain showed a focus of reduced diffusion involving the upper left aspect of the pons and the posterior medial pons about the periaqueductal/inferior colliculus region. There was no hemorrhage, mass effect nor herniation (Figure 1 and Figure 2). MRA of the brain reported filling defect within the distal basilar artery and proximal left posterior cerebral artery (Figure 3 and Figure 4). Neurology was consulted. She was outside of the tissue Plasminogen Activator (tPA) administration window because the onset of symptoms was greater than 4 hours and was also not a candidate for embolectomy as NIHSS was only 3 and the occlusion was partial. She also tested positive for SARS-CoV-2 on PCR test. D-Dimer level was elevated but C-Reactive Protein (CRP) was normal. Echocardiogram was unremarkable. The patient had no history of autoimmune disorder. Patient was initially treated with antiplatelet medications aspirin and clopidogrel (Plavix). Her condition improved and she could ambulate with a front wheel walker and with a stand-by assist. She was discharged four days later with anticoagulation medication rivaroxaban (Xarelto) for 3 months.
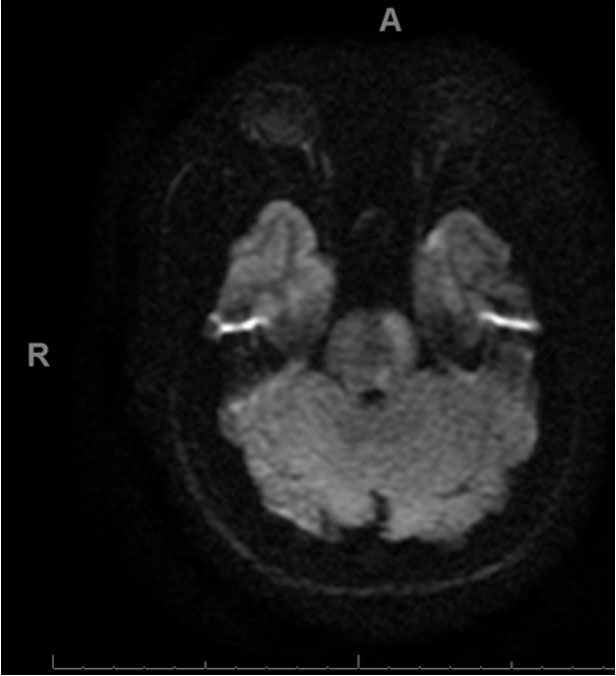 Figure 1: Magnetic Resonance Imaging (MRI), diffusion-weighted, axial section of the brain showing reduced diffusion on the upper left aspect of pons.
Figure 1: Magnetic Resonance Imaging (MRI), diffusion-weighted, axial section of the brain showing reduced diffusion on the upper left aspect of pons.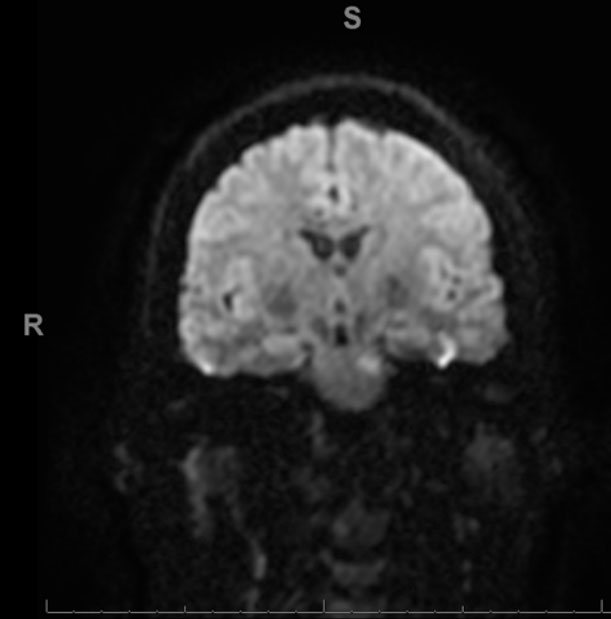 Figure 2: MRI sagittal section of brain shows lesions at the left pon
Figure 2: MRI sagittal section of brain shows lesions at the left pon Figure 3: : MRA sagittal section of the head showing filling defect within the distal left basilar artery.
Figure 3: : MRA sagittal section of the head showing filling defect within the distal left basilar artery. Figure 4: : MRA sagittal section of the head showing filling defect within the distal left basilar artery.
Figure 4: : MRA sagittal section of the head showing filling defect within the distal left basilar artery.The significance of this case is how the young and healthy population can still be negatively affected by SARS-CoV-2 even though they have no respiratory symptoms whatsoever. While the incidence of ischemic stroke in “asymptomatic” SARS-CoV-2 patients is probably very low, the overall high prevalence of SARS-CoV-2 infections during pandemic may result in more patients affected by ischemic stroke. While this patient used oral contraceptives, she did not smoke. Perhaps SARS-CoV-2 infection increases the risk of arterial embolism in patients on contraceptives? Should we offer low dose anticoagulation to folks with “asymptomatic” SARS-CoV-2 infection? Will aspirin be enough? Or will low molecular weight heparin be needed? Do women infected with SARS-CoV-2 while on oral contractives need prophylactic anticoagulation? What about post-menopausal women on hormone therapy? Would they also need to be anticoagulated prophylactically if infected with SARS-CoV-2? Further studies are needed to answer these questions.
The authors declare no competing financial interest.
None.

