 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Trine Maria Mejnert Joergensen1,2*, Holger Wemmelund3,4, Anders Green5,6, Jes S. Lindholt6, Kim Houlind1,2
1Deptartment of Vascular Surgery, Kolding Hospital, Sygehusvej 24. 6000 Kolding, Denmark
2University of Southern Denmark, Institute of Regional Health Research, Winsløwparken 19, 3, 5000 Odense C, Denmark
3Department of Anaesthesiology, Herning Regional Hospital, Gl. Landevej 61, 7400 Herning, Denmark
4OPEN, Odense Patient data Exploratory Network, Odense University Hospital/Department of Clinical Research, University of Southern Denmark, J.B. Winsløws Vej 9 A, 3, 5000 Odense C, Denmark
5University of Southern Denmark, Institute of Clinical Research, Winsløwparken 19, 3, 5000 Odense C, Denmark
6Elitary Research Centre of Individualized Medicine in Arterial Disease (CIMA), Department of Cardiothoracic and Vascular Surgery, Sdr. Boulevard
29, 5000 Odense C, Denmark
Correspondence to: Trine Maria Mejnert Jorgensen, Department of Vascular Surgery, Kolding Hospital, Sygehusvej 24. DK-6000 Kolding, Denmark.
Received date: November 23, 2020; Accepted date: December 06, 2020; Published date: December 13, 2020
Citation: Mejnert Joergensen TM, Wemmelund H, Green A, et al. (2020) Develop More Aggressively Among Patients With a Positive Family History of the Disease. J Med Res Surg 1(6): pp. 1-7. doi: 10.52916/jmrs204035
Copyright: ©2020 Mejnert Jorgensen TM, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Introduction: It is well known that a family history of Abdominal Aortic Aneurysm (AAA) strongly increases the risk of developing AAA, but it is still unknown whether familial AAAs develop differently than non-familial AAAs.
Objectives: To investigate whether familial AAAs develop more aggressively than non-familial AAAs by looking at the growth rate, risk of surgery and rupture, as well as the size of the aneurysm at the time of diagnosis and the patient’s age at the time of operation, rupture and diagnosis.
Design: Observational retrospective longitudinal study.
Materials and Methods: 318 patients with AAA diagnosed between 1996-2008 in Jutland, Denmark with information on family history of AAA, the diameter of AAA throughout follow-up, surgery, ruptures, comorbidity, smoking, and use of medication. Patients with and without a family history of AAA were compared regarding mean age at diagnosis and surgery, the diameter of AAA at diagnosis, risk of surgery and rupture as well as comorbidity and use of medication. Mean growth rates were compared between the two groups and a mixed-effects model was fitted to control for confounders.
Results: We included 93 patients with and 225 without a family history of AAA. Patients with a family history of AAA ere significantly younger than patients with no family history of the disease (69.8 vs. 72.4 years, p=0.032), but we found no significant differences in age at operation (72.2 vs. 70.6, p=0.204), the proportion of patients experiencing rupture (16.0 vs. 10.6%, p=0.226) or undergoing surgery (78.2% vs. 81.7%, p=0.484). We found no significant difference in growth rates between the two groups; 5.25 mm/year for patients with positive family history and 6.19 mm/year for patients with no family history of AAA (p=0.490).
Conclusions: We found no evidence to suggest that AAA develops more aggressively in patients with a positive family history of the disease.
Abdominal aortic aneurysm, Family history, Vascular surgery, AAA, Aortic diseases
AAA: Abdominal Aortic Aneurysm; COPD: Chronic Obstructive Pulmonary Disease; MRI: Magnetic Resonance Imaging; US: Ultrasound; AIC: Akaike Information Criterion.
AAA: Abdominal Aortic Aneurysm; COPD: Chronic Obstructive Pulmonary Disease; MRI: Magnetic Resonance Imaging; US: Ultrasound; AIC: Akaike Information Criterion. Abdominal Aortic Aneurysm (AAA) is a potentially lifethreatening, progressive disease, which is related to arteriosclerosis, hypertension, and smoking, but also to familial predisposition, which strongly increases the risk of developing AAA. This was first reported by Clifton in 1977 [1] and later confirmed in other studies [2-4]. It has recently been shown [5] that a very high percentage of the liability of the development of AAA is caused by genetic effects and the higher prevalence of AAA among first-degree relatives with the disease is probably due to the familial accumulation of genes responsible for the development of the disease. It is, however, not knowing whatthis means for the individual patient in terms of managing the disease. Unanswered questions include whether the familial cases are more likely to rupture, whether they grow faster and whether the patients are younger when they get the disease.
There have been very few reports of increased or decreased growth rates of familial AAA compared to growth rates of AAA in patients without a family history of the disease. In a recent small study from Japan [6], Akai et al showed that a family history of AAA was an independent risk factor for increased growth rate. However, the study only included nine patients with a family history of AAA and only included small aneurysms. Whether familial AAA develops earlier than non-familial AAA is also uncertain; Baird [7] and Adamson [8] found that patients with familial AAA had a lower age at the time of surgery and although one study found a higher rupture rate and the lower average age at rupture among familial cases [9], studies regarding familial AAA are generally few and often of older date. Further investigation seems needed to determine whether familial aortic aneurysms develop more aggressively among patients with a positive family history of the disease.
This study aimed to investigate whether familial abdominal aneurysms develop more aggressively than non-familial AAAs by looking at the growth rate, risk of surgery and rupture, as well as the size of the aneurysm at the time of diagnosis and age at the time of surgery, rupture and diagnosis.
For this study, we created an AAA growth database including all cases of AAA in Jutland, Denmark from 1996-2008. The peninsula of Jutland has approximately 2.5 million inhabitants. Using the Central Person Registration System [10,11] (which provides all Danish residents with a unique identification (CPR) number) the growth database was cross-linked with the Danish National Patient Registry, the Danish National Prescription Registry and the Integrated Database for Labor Market Research to retrieve information regarding comorbidity, use of medication and level of education.
The National Patient Registry [12] contains information on all somatic hospital contacts, including date of hospitalization, department, main and secondary diagnoses, operations and procedures, place of residence and CPR number. Diagnoses are classified according to the International Classification of Diseases (ICD). ICD-8 was used until 1993, ICD-10 hereafter. Operations and procedures are classified according to the NOMESCO Classification of Surgical Procedures (NCSP). AAA was coded as 441.20 or 441.29 in ICD-8 with procedure codes 86550-86555 and I714 in ICD-10 with procedure codes KPDG10, KPDG20, KPDG21, KPDG23, KPDG24, KPDQ, and KPDQ10. Ruptured AAA was coded as 441.21 in ICD-8 and I713 in ICD-10. The National Patient Registry was also used to retrieve information on the level of overall comorbidity including acute myocardial infarction, congestive heart failure, Chronic Obstructive Pulmonary Disease (COPD), hypertension and cerebrovascular disease using ICD-codes as well as using the Charlson Comorbidity Index (CCI) score [13] for assessing the overall level of comorbidity.
The Danish National Prescription Registry [14] contains information on all dispensed prescriptions in Denmark, including, type and amount of medication and the date of dispensation. Information regarding the use of medication included the use of Acetylsalicylic Acid (ASA) or other NonSteroidal Anti-inflammatory Drugs (NSAID), AngiotensinConverting-enzyme inhibitors (ACE-inhibitors), statins and betaadrenoceptor blocking agents (beta-blockers). Information on the level of education was retrieved from the Danish Integrated Database for Labor Market Research (IDA) [15].
In the growth database, we included retrospective data from medical records including baseline information (up to one year before the first contact with a vascular surgical department) on smoking status, alcohol consumption, claudication and ankle-brachial index. In cases where surgery for AAA was performed, it was registered whether any iliac aneurysms were present. If no surgery was performed it was registered if the patient was considered unfit for surgery. Furthermore, the database includes up to ten recorded diameters of the AAA for each patient with information on the size in mm, date, imaging modality (Computed Tomography (CT), Magnetic Resonance Imaging (MRI) or Ultrasound (US) and direction of measurement (anteroposterior or maximum). AAA was defined as a maximum abdominal aortic diameter ≥ 30 mm. All scans performed within the study period were included even if some measurements were < 30 mm. Information on family history of AAA was also included and patients were defined as having a positive family history if they had stated at least one first degree relative with the disease. Family history could be registered as “yes”, “no” or “unknown”. Patients with unknown status or where the status had not been recorded were excluded (see Appendix 1 for patient characteristics regarding included and excluded patients). Only preoperative data were included and follow-up was defined as the time between the first and the last scan performed.
Both medically treated and diet regulated diabetes were included. Peripheral artery disease (PAD) was defined as either the ankle-brachial index < 0.9 and/or a history of intermittent claudication.
In the analysis of growth rates, we included patients with at least two measurements at least 3 months apart. MRI scans were excluded from the analysis of growth rates as they were not commonly used for follow-up, but mostly for initial analysis when patients were examined for other reasons
All analyses were performed according to a predefined analysis plan. In the univariate analyses, the Pearson Chi-square test was performed to test categorical variables for variables with frequencies >5 in each cell and Fischer’s exact test for variables with cells with frequencies < 5. Univariate analyses on continuous data were performed using a paired t-test. Any p-value < 0.05 was considered statistically significant.
Growth rates were calculated as changes in diameter over time with each measurement as a time point. A mean growth rate for each patient was then calculated and overall means between patients with and without a family history of AAA werecompared. To test for confounders a mixed-effects model with a random slope (allowing each patient to have a unique growth rate) and random intercept (allowing each patient to have a unique overall level) was fitted. Mixed-effects models are commonly used for growth data and include both fixed variables (that do not differ over time e.g. sex or other baseline information such as comorbidity) and variables with random effects (effects that vary between each observation e.g. direction of measurement of aortic diameter) [16].
Random effects models allow for clusters in data as well as for the non-independence of repeated measurements and can be fitted to take differences between modalities into account. A logarithmic transformation of the outcome variable (the measurement of AAA-diameter) was necessary to account for the observed exponential growth of aneurysms. Initial analysis was done including known confounders (smoking and diabetes) as well as variables that differed between the two groups in the univariate analyses (hypertension and age at initial scan). Furthermore, we included size of the aneurysm at first measurement as an explanatory variable, as it is expected that larger aneurysms grow faster than smaller ones. We assumed random effects of time, imaging modality and direction of measurement. Model assumptions were tested using residualplots and the Akaike Information Criterion (AIC) was used to identify the best fitting model (the model with the lowest AIC value was preferred).
We included a total of 318 patients with information on family history. Ninety-three had a positive family history and 225 had no known family history of AAA (see flow diagram, Figure 1).Patient characteristics and surgery details can be seen in Table 1. Patients with a positive family history of the disease were more than two years younger at diagnosis (69.8 vs. 72.4 years, p=0.032) with a non-significant tendency towards the familial aneurysms having a smaller maximum diameter at diagnosis (54.5 vs. 57.8 mm, p=0.098). Patients with a positive family history had more follow-up scans performed (mean number of scans 3.0 vs. 2.4, p=0.024), but there was no significant difference in the mean duration of follow-up (16.7 vs. 13.7 months, p=0.317). We found no significant difference between the two groups (+/- family history of AAA) regarding sex, age at surgery or rupture, frequency of surgery or rupture, the proportion of patients with iliac aneurysms or the proportion of patients being considered unfit for surgery and we found no differences between the educational level and history of smoking between the two groups.
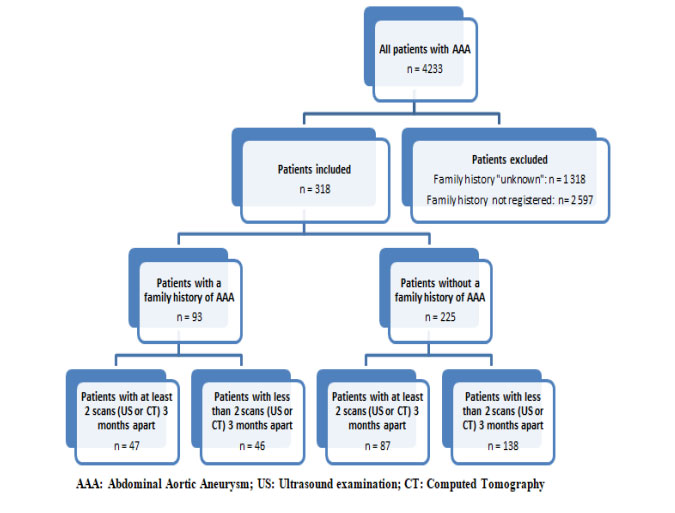 Figure 1: : Flow diagram of included and excluded patients.
Figure 1: : Flow diagram of included and excluded patients.| Without familiar disposition n=225 | With familiar disposition n=9 | p-value | |
|---|---|---|---|
Male sex, n (%)
Yes |
(N=225)
196 (87.1) |
(N=93)
77
(82.8) |
0.315 |
Surgery, n (%)
Yes (open surgery or EVAR) |
(N=225)
176 (78.2) |
(N=93
76 (81.7 |
0.484 |
Unfit for surgery, n (%)
Yes |
(N=192)
16 (8.3) |
(N=84)
5 (6.0) |
0.828 |
Age at first scan (years), mean
(range) |
(N=132) 72.4
(52.7-88.2) |
(N=49)
69.8 (51.0-84.7) |
0.032* |
Modality initial scan, n (%)
Ultrasound
CT
MR |
(N=215)
144 (67.0)
66 (30.7)
5 (2.3) |
(N=89)
50 (56.2)
36 (40.4)
3 (3.4) |
0.200 |
Follow-up
Number of scans, mean (range)
Months of follow-up, mean (range) |
(N=225)
2.4 (0-10)
13.7 (0-176) |
(N=93)
3.0 (0-9)
16.7 (0-81) |
0.024* 0.317 |
| Age at surgery (years), mean (range) | (N=110)
72.2 (52.7-86.4) |
(N=47)
70.6 (52.6-87.6) |
0.204 |
| Age at RAAA (years), mean (range) | (N=36)
71.7 (52.7-85.5) |
(N=10)
71.3 (52.6-87.6) > |
0.897 |
RAAA, n (%)
Yes |
(N=225)
36 (16.0) |
(N=93)
10 (10.6) |
0.226 |
Level of education, n (%)
Primary
Secondar
Higher education |
(N=118)
62 (52.5)
39 (33.1)
17 (14.4) |
(N=47)
23 (48.9)
20 (42.6)
4 (8.5) |
0.424 |
Initial scan,
mm (range)
Max. diameter
Max. AP-diameter |
(N=215)
57.8 (25-120)
58.2 (30-104) |
(N=89)
54.5 (32-105)
54.3 (35-83) |
0.098 0.116 |
Iliac aneurysm, n (%)
Yes |
(N=173)
66 (38.2) |
(N=75)
30 (40.0) |
0.784 |
Smoking, n (%)
Current
Former
Never |
(N=210)
107 (51.0)
79 (37.6)
24 (11.4) |
(N=86) 44 (51.2)
32 (37.2)
10 (11.6) |
0.997 |
Alcohol abuse
Yes |
(N=100)
12 (12.0) |
(N=42)p> 3 (7.1) |
0.390 |
| RAAA=Ruptured Abdominal Aortic Aneurysm, EVAR=Endovascular Aneurysm Repair; Alcohol abuse=More than 2 standard drinks per week for women/3 standard drinks per week for men. N: number of patients with information regard | |||
Regarding comorbidity and use of medication, we only found one significant difference between the groups: there was a larger proportion of patients diagnosed with hypertension in the group with a family history of AAA compared to the group with no known family history of AAA (29.6 vs. 15.6%, p=0.023).
We found no significant differences regarding CCI score, PAD, cardiac disease, COPD or use of medication (statins, ASA or other NSAID, ACE-inhibitors or beta-blockers). See Table 2 for details regarding comorbidities and use of medication.
Table 2:Patient comorbidity and use of medication| Without familiar disposition n=225 | With familiar disposition n=93 | p-value | |
|---|---|---|---|
CCI score, n (%)
0 |
(N=138)
58 (42.0) |
(N=54) 28 (51.8) | 0.315 |
1
2 |
36 (26.1)
44 (31.9) |
9 (16.7)
17 (31.5) |
0.315 |
Hypertension, n (%)
Yes |
(N=138)
21 (15.2) |
(N=54)
16 (29.6) |
0.023* |
Diabetes, n (%)
Yes |
(N=49)
7 (14.3) |
(N=16)
2 (12.5) |
0.857 |
PAD, n (%)
Claudication
ABI<0.9 |
(N=129)
39 (30,2)
(N=225)
34 (15.1) |
(N=57)
19 (33.3)
(N=93)
19 (20.4) |
0.674
0.246 |
Cardiac disease, n (%)
Myocardial
infarction
Congestive heart failure |
(N=138)
24 (17.4)
13 (9.4) |
(N=54)
13 (24.1)
7 (13.0) |
0.291
0.470 |
COPD, n (%)
Yes |
(N=138)
15 (10.9) |
(N=54)
11 (20.4) |
0.084 |
Cerebrovascular disease,
n (%) Yes |
(N=138)
19 (13.8) |
(N=54)
11 (20.4) |
0.257 |
Statins, n (%)
Current users |
(N=138)
29 (21.0) |
(N=54)
16 (29.6) |
0.204 |
ASA, n (%)
Current users |
(N=138)
46 (33.3) |
(N=54)
19 (35.2) |
0.810 |
Other NSAID, n (%)
Current users |
(N=220)
12 (5.4) |
(N=80)
4 (5.0) |
0.881 |
ACE-inhibitors,
n (%) Current users |
(N=138)
23 (16.7) |
(N=54)
13 (24.1) |
0.238 |
Use of beta-blockers,
n (%) Current users |
(N=138)
38 (27.5) |
(N=54)
10 (18.5) |
0.194 |
| CCI=Charlson Comorbidity Index; Hypertension=Subjects with diagnosed hypertension; PAD=Peripheral Arterial Disease; COPD: Chronic Obstructive Lung Disease; NSAID=Non-Steroid Anti-Inflammatory Drugs; ASA=acetylsalicylic acid; ACE = Angiotensin Converting Enzyme N denotes the number of patients with information regarding the specific variable | |||
In the analysis of growth rates, we included a total of 134 patients (47 with and 87 without a family history of AAA), who had at least two measurements of AAA-diameter at least 3 months apart. The crude means growth rate was 5.25 mm/ year (95%CI: 3.73; 6.78) for patients with positive family history and 6.19 mm/year (95%CI: 4.40;7.97) for patients with no family history of AAA (p=0.490). Also, we found no significant difference between growth rates in the two groups when fitting data to the mixed-effects model. However, large initial diameter, as well as modality (CT scans versus US scans), were independently associated with increased growth rates. See Table 3 for results from the best fitted reduced mixed-effects model.
Table 3:Results from a mixed-effects model| Outcome variable: logus (log(AAA diameter, mm)) | Regression coefficient | Standard Erro | p-value |
|---|---|---|---|
Sex
Male |
0.0226 | 0.0227 | 0.32 |
Familial disposition Yes |
0.0300 | 0.0180 | 0.10 |
| Time, years | 0.0742 | 0.0051 | < 0.001* |
Initial diameter, mm
30-39
40-49
50-55
>55 |
Reference
0.2113
0.3657
0.5828 |
Reference
0.0234
.0287
0.0289 |
Reference
<0.001*
<0.001*
<0.001* |
Modality
UL
CT |
Reference
0.0524 |
Reference
0.0107 |
Reference
< 0.001* |
| Outcome variable: log-transformed measurement of maximal aortic diameter in mm AAA: Abdominal Aortic Aneurysm *: p-value significant at 95% confidence level | |||
In this study, we found that a family history of AAA was not an independent risk factor for increased growth rate. Familial cases tended to have a lower growth rate than non-familial cases; however, this finding was not significant. We did find a difference in age at first diagnosis as familial cases were generally about two years younger than non-familiar cases and we also found a non-significant trend towards smaller diameter of the AAA at the first scan. We did not find that familial cases had a higher risk of surgery or rupture and even though there was a tendency towards familial cases having surgery at a younger age, this was not a significant finding. We found no difference in mean age at rupture between the two groups. All these findings combined point towards familial cases being diagnosed earlier, probably because of increased attention towards screening of first-degree relatives of AAA-patients. There is, however, nothing in our data that suggests that familial cases of AAA behave more aggressively than non-familial cases.
The tendency towards a lower growth rate among familial cases is contrary to findings of a recent study by Akai et al. [6], which demonstrated a family history of AAA to be associated with more rapid growth. This study, however, included only very few patients (9 with a family history of AAA) with small aneurysms (≤ 5 cm) and in the analysis, they assumed linear growth of aneurysms. Also, differences in the pathophysiology of AAA may exist between Asian and Caucasian populations. Furthermore, it was not possible to identify the reason for the very small number of patients with a family history of AAA as information on the initial study base was not included. It is therefore difficult directly to compare the results [17].
In this study, we included both US and CT scans and we found that CT scans were associated with faster growth than ultrasound. There are some possible explanations for this. First, CT scans are known to overestimate the diameter compared to US [18,19] and our findings are in line with this. Second, in Denmark CT scans are often used in the planning of operative treatment (open surgery or EVAR) when the diameter of the AAA reaches a size that requires surgery, whereas the US is often used in the surveillance of smaller aneurysms. Third, CT scans are often used in the diagnosis of ruptures, which is more likely to occur in larger AAAs or in AAAs with more rapid growth. To account for this possible bias, we included modality both as a fixed variable as well as a random variable in the mixed-effects model.
We found no significant difference between the initial maximum mean diameter in the two groups. It is however worth noting that the mean diameter in both groups was very close to or even above the threshold for surgical intervention. This, combined with the large proportion of ruptures in both groups (14.5 % in the two groups combined) as well as in the group of patients not included in the analysis (30.3%) emphasizes the need for a national population screening program in Denmark.
Since this study is based on clinical data, the scans (whether it be the initial scan or the scans performed during follow-up) were not performed according to a standardized method. We aimed to take this into account when fitting the mixed-effects model as this model allows for different effects of both modality and direction of measurement. To limit the errors of measurement, we excluded MRI scans from the growth data, as these are often performed for other reasons than the follow-up of AAA.
A major limitation of this study is the large proportion of patients with missing data on family history of AAA. This group included a large proportion of ruptures and, naturally, there were missing data on this group of patients, where the main focus often is immediate surgery. We included information regarding the excluded patients in appendix 1 and 2 and overall the included and excluded patients were very similar.
In this retrospective study of differences in AAA among patients with and without a family history of the disease, we did not find any evidence to suggest that familial cases of AAA develop more aggressively than non-familial cases. We found that patients with a positive family history were younger at diagnosis, but we did not find any statistically significant differences regarding growth rate, age at operation, or rupture and we did not demonstrate any differences between the frequencies of operations performed or ruptures in the two groups. Generally, there were very few differences between the two groups regarding comorbidity and use of medication.
This study has been approved by the Danish Data Protection Agency and the Danish Health and Medicines Authority
The University of Southern Denmark; The Region of Southern Denmark; Viborg Regional Hospital, Viborg, Denmark; Rosa and Asta Jensens Foundation, Viborg, Denmark; The Health Research Foundation of the Central Denmark Region.
The funding sources have not been involved in designing the study, collecting, analyzing or interpreting data, writing the manuscript or deciding regarding submission of the article for publication

