 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN TH AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN TH AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN TH AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN TH AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
David John Mackay Smith*
Department of Medicine, University of Queensland, Australia
Correspondence to: David John Mackay Smith, Department of Medicine, University of Queensland, Australia.
Received date: October 6; 2021; Accepted date: October 14; 2021; Published date: October 21, 2021
Citation: Smith DJM (2021) The Influence of Non-UV Wavelengths of Light on Skin: What Constitutes a Healthy Level of Exposure Particularly in Relation to
Melanoma?. J Med Res Surg 2(S1): pp. 1-5. doi: 10.52916/jmrs21S104
Copyright: ©2021 Smith DJM. This is an open-access article distributed under the terms of the Creative Commons Attribution License; which permits unrestricted
use; distribution and reproduction in any medium; provided the original author and source are credited.
We live with solar radiation from birth to death and have since the emergence of life on earth. Why then does skin cancer diagnosis remain so disturbingly high in Australia? Part of the problem is the majority of the population are of Northern European ancestry. Moving closer to the equator on mass we have carried with us a polymorphic melanocortin receptor gene on our melanocytes responsible for an incomplete tanning response. We attempt to protect ourselves with clothing and creams or remain indoors but this does not seem to be stemming the tide.
Occupation, recreation or both drive us outside and into the sun. We need to be more successful at negotiating the potentially harmful effects by relooking at solar radiation and instead of focusing on the most harmful wavelengths look at the overall effect of the whole spectrum. We also need to re-examine our behaviour and exposure patterns.
Prolonged periods indoors under artificial light punctuated with short bursts of intense irradiation is maladaptive. Creams aim to block the ultraviolet component, ignoring 90% of solar photons, the protective effect is incomplete, yet their use encourages more prolonged exposure. Protective behaviours are necessary for the most sensitive skin types but they are still at risk. For the rest of the population evolutionarily developed natural protective mechanisms can be employed. Regular moderate sun exposure, below the burn threshold, ideally aimed at early morning or late afternoon. Augmented with clothing, hats and creams with an appreciation of the incomplete protective effect of these measures.
Electromagnetic radiation, Skin, Melanoma, Ultraviolet, Visible Light, Infrared.
Electromagnetic radiation emitted by the sun covers a wide spectrum of wavelengths but only a fraction reaches the earth’s surface. Ultraviolet radiation (UVR; 280-400 nm), visible light (VL; 400-700 nm) and infrared (IR; 700 nm-1 mm). The shortest wavelength of UVR, UVC (100-280 nm) is absorbed by the ozone layer. The contribution of the UV component of solar radiation to skin damage, with exposure, has been established. Activity levels of UVR can break covalent bonds resulting in direct DNA damage but it has been found that there is also an indirective effect of oxidative damage on DNA through the production of Reactive Oxygen Species (ROS).
The early fixation on reaction to the specific UVB (280-320 nm) wavelengths, led to an overestimation of its biological importance. This has been followed by a change in focus to include longer UV wavelengths with an appreciation of the underestimation of UVA (320-400 nm) damage. All the attention has been on UV effects, consequentially, the additive, synergistic or antagonistic interactions between different wavelengths have been largely overlooked.
Mahmoud demonstrated that visible light has an effect on erythema, pigmentation, thermal damage and free radical production in human skin [1,2] and Liebel et al found that irradiation of human skin equivalents with visible light induced production of ROS, pro-inflammatory cytokines and Matrix Metalloproteinase (MMP-1), with deeper penetration at a dermal level, suggesting that visible light contributes to skin photoaging [3].
How significant is the contribution of these non-UV wavelengths of solar radiation to skin damage through exposure? Should sunscreens provide an even broader wavelength protective effect, and is it appropriate to single out UV, being the most biologically active wavelengths, rather than consideration of the total effect of the whole solar spectrum? UVA can augment UVB-induced immunosuppressive effects but, alternatively, at an appropriate dose and wavelength, it can provide immuneprotection through modulation of cytokines and enzymes such as heme oxygenase (OH-1) with anti-inflammatory and antiapoptotic properties [4]. Exposure to non-UV wavelengths contributes to photoaging, at least, but this is also dose related, low doses having beneficial effects on wound healing and photo-adaption [5,6]. There now needs to be an appreciation of the human response to the complete solar spectrum. Is the common factor the oxidative effect of excess free radical production? This free radical production is the start of a cascade of biological effects with both either beneficial or damaging outcomes. Considering that UV comprises < 10% of solar radiation and sunscreens are ineffective at protection from other wavelengths, the potential harmful, and beneficial, effects of the Visible Light (VL) and Infrared (IR) components need to also be considered.
With few exceptions, life on our planet depends ultimately on sunlight as an energy source. The fact that sunlight can be both beneficial and harmful has been a key factor in the evolution of life. Perhaps, the most remarkable aspect of this fact is that even after approximately 3 billion years of natural selection, under the stress of solar radiation, it is still a serious environmental hazard for humans. Only if they move out of their long-term geographical niche either by immigration (Australia, USA) or by culture (summer holidays in Spain). Allowing for present trends in ozone depletion and possessing a variety of avoidance and repair processes, humans, are still at risk under solar exposure. Overall, the fitness of individuals relies on exposure levels, age, physiological state and innate ability to correct solar irradiationinduced DNA damage.
Solar radiation is essential to our well-being. Our design has evolved to deal with outdoor exposure, and most Australians aspire to an outdoor life-style, however, excessive exposure to solar radiation has immediate and long-term negative consequences. Sunburn, immunosuppression, premature skin aging and cancer. The modern life-style follows a pattern far removed from our primitive ancestors. We now spend prolonged periods indoors under artificial light, with short irregular periods exposed to solar radiation. Recreational activities and holidays in more sun-drenched locations to catch up on exposure. We cover ourselves with protective creams and clothing but there remains a disturbingly high rate of melanoma diagnosis in Australia. This trend persists partly in relation to preceding comments but also, I would suggest, to present maladaptive exposure patterns to solar radiation.
On a photon entering the skin there is scattering and this is directly dependent on the wavelength of the photon, affecting the depth of penetration. Longer wavelengths, although less biologically active, penetrate deeper. There is also a process of absorption. This, initiates chemical changes in the cell with transfer of the photon’s energy to a chromophore. Depth of penetration is not only affected by wavelength but also the position and absorption spectrum of the chromophore. Absorption spectrum is the probability of absorption against the wavelength. A number of chromophores only absorb in the UV and others absorb throughout the UV and visible wavebands, β-carotene has absorption maxima at 465 and 490nm in the visible spectrum but also absorbs in the UV range. Other endogenous chromophores which absorb in VL include melanin, water, riboflavin, haemoglobin and bilirubin. Exceptionally, melanin absorbs throughout the UV and visible wavebands (Figure 1).
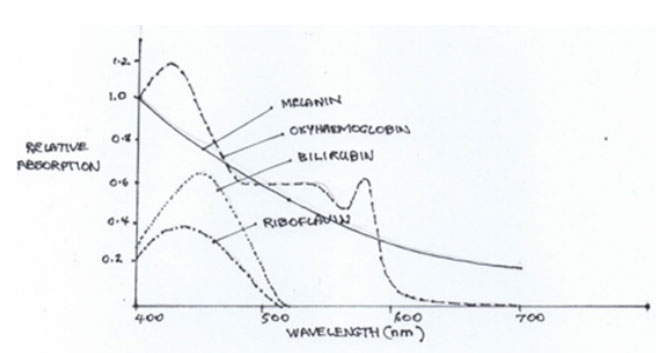 Figure 1: Skin chromophore absorption spectra (Adapted from Mahmoud et
al, 2008).
Figure 1: Skin chromophore absorption spectra (Adapted from Mahmoud et
al, 2008).
The photoprotective effect of the skin resides in the epidermis where the keratinocyte and melanocyte cooperate with melanin being made available to the keratinocytes through either oxidation or neo-synthesis of melanin by the melanocyte and thickening of the stratum corneum by the keratinocytes. Melanin is a neutral density filter, capable of absorbing across the broad spectrum of UVR and VL, as well as scavenging ROS and acting as an antioxidant. Melanin is packaged as melanosomes, darker skin types having larger, more dispersed melanosomes, which provide better protection and these skin types also show enhanced DNA repair
Melanin is a biopolymer, represented in a wide range of living organisms. In specialised organelles of melanocytes L-tyrosine is oxidised by tyrosinase. The oxidation products interact amongst themselves favouring self-polymerisation and eventually producing two types of melanin, eumelanin and pheomelanin. Both are rich in conjugated C-C double bonds, giving them the ability to absorb free electrons, promoting their role as endogenous sunscreens. This oxidation process can have both positive and negative effects.
Photoexcitation of melanin in human skin by sunlight results in the formation of excited states such as reactive oxygen or nitrogen species that if produced in excessive quantities can transfer energy/electrons to surrounding molecules. VL on melanin inducing significant oxidative damage in nucleic acids, lipids, proteins. There is also the accumulation of premutagenic lesions in sensitive sites in nuclear DNA. Skin cells respond by release of pro-inflammatory cytokines and MMP-1, propagating further cell death and skin aging.
Melanin absorbs both UVR and VL. Traditionally UVR has been considered to be the cause of skin photodamage because of its higher level of activity. This is problematic because UVR makes up < 10% of irradiance with a much larger contribution being shared between VL and IR. There is considerable scientific evidence that VL produces a similar effect to UVA. VL inducing melanoma in cells and animal models [7].
Early on, Moan et al found epidemiological support for a hypothesis that melanoma induction indicated a role for UVA radiation [8]. Using data from Norway and Australia, they found that the latitude gradients for BCC/SCC were significantly larger than for melanoma and this closely followed the latitude gradient for UVB, whereas the gradient for melanoma more closely followed that for UVA. They suggested that melanin in the upper layers of the skin is protective, while melanin in melanocytes is subjected to melanogenic change by the longer wavelengths that are penetrating deeper [9].
Current photoprotection policies are heavily focused on avoiding UVR effects of sunlight exposure. This is reflected in sunscreens that only provide protection in the UV range, the potential adverse effects of other wavelengths being ignored. The frequency of skin cancer continues to increase in Caucasian populations worldwide. This begs the question as to whether what is considered proper application of sunscreen is encouraging excessive sun exposure with skin damage still occurring through the effects of the ignored wavelengths of solar radiation and unrealistic expectations of the protective effect of sunscreens.Acute effects of UVR include, erythema, pigment darkening and delayed tanning, epidermal hyperplasia and Vitamin D synthesis. Erythema is a cutaneous inflammatory reaction, peaking at 6-24 hours. Pigment darkening is biphasic. Immediate Pigment Darkening (IPD), induced by UVA, occurs within minutes, lasting up to 2 hours. At higher doses of irradiation, it is followed by Persistent Pigment Darkening (PPD), lasting up to 24 hours. Delayed tanning occurs after 3-5 days induced by UVB and may persists for days, weeks or months, influenced by genetic factors. Chronic effects are photoaging, immunosuppression and photo-carcinogenesis, melanoma and non-melanoma skin cancer. These are the commonest cancers in some Caucasian populations, such as Australia and United States.
VL is the portion of the electromagnetic spectrum visible to the human eye, which responds to 400-760 nm, with maximum sensitivity at 555 nm, the green region of the optic spectrum. Accumulation of melanin can be considered to be a photoprotective response by melanocytes to reduce DNA damage induced by UVR. It is known that excess UVA radiation induces modification and degeneration in both eumelanin and pheomelanin. Despite the fact that visible light (VL) makes up nearly half of the solar spectrum there has been very little study on VL’s potential involvement in this sort of effect.
Ito et al investigated the role of VL, alone or in combination with UVA, in the photodegradation of both types of melanin in human epidermal melanocytes. Ito has a long history in the examination of the structure and chemistry of melanin. Using physiological doses of VL and UVA, they found that VL accelerated the UVAinduced structural changes in both types of melanin, although acting alone there were only minor changes [10].
In 2012 Liebel et al examined the physiological responses of skin equivalents to visible light (400-700nm) irradiation. They found production of ROS, pro-inflammatory cytokines, and Matrix Metalloproteinase (MMP-1) suggesting that other portions of the solar spectrum contributed to skin damage and that sunscreens, aimed purely at UV wavelengths, may be providing an incomplete protective effect [3].
Erythema and sunburn are mainly caused by UVB. UVA and VL can cause erythema but require a much higher dose. A 1960 study found UV (250 and 297 nm) erythema was caused by capillary dilatation, these wavelengths only penetrating superficially into the upper dermis. Longer wavelengths penetrate deeper into the dermis resulting in dilatation of vessels of the subpapillary plexus [11].
VL induces pigmentation especially in darker skin types playing a part in the pathophysiology of photo-induced pigmentary disorders, such as melasma and post inflammatory hyperpigmentation, through interaction with potential photoallergens. Sunscreens are ineffective at reducing this effect [2] .
IR consists of wavelengths 700 nm-1 mm, and accounts for about 40% of solar radiation reaching the earth’s surface. It is divided into IRA (near IR); 700-1400 nm, IRB; 1400-3000nm and IRC; 3000 nm-1 mm. IRA and B penetrate to the subcutis while IRC is almost completely absorbed in the epidermis, due to the presence of water, its chromophore.
Piazena et al suggested that a single exposure was capable of inducing erythema, thermal pain and tissue damage, chronic exposure causing erythema ab igne and squamous cell carcinoma [12]. With the focus of attention on UV, the biological effects of IR have been neglected due to the idea that these effects are almost always mediated by heat enhancement, with the induction of heat shock proteins (Hsp). However, Menezes et al pre-irradiated E. coli with IR, under temperature control, and found that they became more resistant to UVC challenge. They then when on to find that, in a similar way, human fibroblasts were protected from cytological effects of UVA/B by a non-lethal, preconditioning dose of IR radiation. Maximal protection ~700-1000 nm. This was independent of proliferative effects or Hsp on the cells. On a daily basis, in the natural environment, cells are first irradiated by IR due to solar zenith angle and absorbance properties of atmospheric components. This IR irradiation prepares cells to deal with the following UV radiation. They proposed that this acts as a natural protective mechanism, acquired and preserved through evolutionary selection. Concluding that “Although sunlight is polychromatic, its final effect on human skin is the result of not only the action of each wavelength individually but also the interactions between wavelengths” [13].
In follow-up studies by Frank et al it was proposed that the protective mechanism involved mitochondrial apoptotic pathways modulating Bcl2/Bax balance, p53 signaling playing a role [14,15]. Applegate et al also suggested a repair mechanism involving Ferritin induced by IR.
So, morning IR, not only pre-conditions skin for later UV irradiation effects but afternoon IR possibly aids in repair [16]. There is evidence from in vitro studies of ROS production and effect on the mitochondrial respiratory chain through both thermal and photochemical mechanisms with IR exposure. Deep penetration affects many cell types- keratinocytes, melanocytes, fibroblasts, Langerhans and vascular endothelial cells, as well as corneal and retinal tissue in the eye [17]. The effects are partially similar and partially different to the influence of UV, making the net effect difficult to predict. There have been few in vivo or epidemiological studies to date. Effects maybe adverse or beneficial depending on total dose administered: fluence (J/cm2 ) and irradiance (mW/cm2 ).
Photobiostimuation occurs at < 10 J/cm2 and adverse effects >120 J/cm [2,18]. There is less experimental evidence between these 2 figures with overlapping effects depending target tissue and irradiance. The contribution of irradiance is not clear, although very low irradiance at high dose should not be harmful. High irradiance (>100 mW/cm2 ) may heat tissues and are likely to be hazardous over even low does. Daily exposure to out-door workers could span a few tens to several hundred J/ cm2 depending on a large range of variables. Tanning maybe a marker of damage or indicate an adaptive response. Immunosuppressive effects may be beneficial or deleterious dependent on level of exposure, health status or coexposure to physical, chemical or biologically active agents with immunomodulatory activity.
Modest ROS production and activation of the NF-kB pathway with changes of gene expression ultimately leads to cellular proliferation and extracellular matrix synthesis and remodelling. This can modulate of some of the UV damaging effects and can be used therapeutically. The photobiostimulatory role has been exploited for years to treat a range of skin conditions, aiding wound healing, reducing inflammation and stimulating metabolism [5,6].
Higher levels of heat or ROS production can lead to heat shock protein (Hsp) synthesis and activation of Activator protein 1 (AP-1) pathway, triggering apoptosis and synthesis of Matrix Metalloprotienase-1 (MMP-1). These changes resulting in acute or chronic skin damage with acceleration of skin aging and possible facilitation of carcinogenesis [18].
This biphasic response to IR, beneficial effects at low dose and damaging at high can result in an adaptive reaction, increasing resilience of tissues to environmental stresses.
Humans have been exposed to solar UVR since our appearance on earth and evolution has enabled individuals, with the capacity, to adapt to exposure, photoadaptation, leading to a decreased response after acclimatisation.
Highly energetic, short UVB wavelengths are absorbed by epidermal chromophores while longer wavelength UVA reaches the basal layer and dermis, effects on the basal layer are enhanced by back scatter from the dermis. Both are genotoxic, either through direct DNA damage by photoproducts or the oxidative effects of ROS formation on cellular DNA, lipids and proteins. ROS can also act as a secondary messenger activating protein kinase proliferative pathways. There is also an immunosuppressive effect, with depletion of Langerhans cells locally and a systemic effect on cytokines, such as IL-10 and TNFα. Visible response is erythema or sunburn, an inflammatory reaction dependent on skin type and expressed as a Minimal Erythema Dose (MED).
There are a number of natural protective responses. Pigmentation, thickening of the epidermis/stratum corneum, DNA repair, mobilisation of antioxidant systems and Vitamin D production. Pigmentation occurs through oxidation of preexisting melanin, enhanced melanin synthesis and increased transfer of melanosomes to keratinocytes. This effect is mediated by paracrine and autocrine stimulation of the Melanocortin 1 Receptor (MC1R) on the melanocyte and polymorphism in MC1R alleles results in a highly variable level of receptor dysfunction in Caucasian populations. Epidermal thickening occurs through proliferation and differentiation of keratinocytes. DNA repair consists of Nucleotide excision repair (NER) and base excision repair (BER) mechanisms. P53 plays a role, transactivating genes involved in G1/2 arrest and global genomic repair genes (a slower part of NER response). This not only removes damage but also increases the resilience of keratinocytes against a second UVB dose, leading to increased survival of cells that retain their capacity to repair. This is achieved only if the interval between insults allows time for the p53 program to be induced [19].
As a skin cancer clinician, I have a special interest in melanoma pathogenesis but there are major inconsistencies and contradictions in exposure patterns that are difficult to reconcile.
It is accepted that sun exposure is the major environmental factor in melanoma incidence, however sun exposure is critical for Vitamin D synthesis. Sub-optimal levels are associated with reduced bone health and increasing literature linking increased risk of other diseases, so that a balance between exposure and protection is needed. Overall, genetic-epidemiological data suggests intermittent exposure and sun-burn have been responsible for the drastic increase in melanoma in Caucasian populations this century. Excluding the high-risk phenotypes, the epidemiological data is complex but suggests that exposure can be protective in some circumstances, possibly through photoadaptation or higher Vitamin D levels [21].
Vitamin D is anti-proliferative in vitro for some melanoma cell lines [22]. At melanoma diagnosis, lower Vitamin D levels are associated with thicker tumours and poorer prognosis [23,24]. Sun-sensitive people have lower Vitamin D levels [25] and patients with a previous diagnosis of melanoma are likely to practice sun-avoidance behaviours. Should we be measuring levels and suggesting supplementation for our melanoma patients?
There is good evidence that moderate, regular sun exposure below the burn threshold is beneficial as far as general health and particularly melanoma risk is concerned. It remains unclear, however, if this relates to photoadaptation or Vitamin D levels. Obviously, this excludes high risk melanoma individuals- personal or strong family history, densely freckled or type I skin type and high naevi counts. There is better prognosis for melanoma in Australia than the UK, comparing populations with a similar ethic background, but with the suggestion that promotion of public education and closer surveillance in Australia providing earlier detection rather than a sunnier climate inducing higher Vit D levels, although vitamin D levels throughout the UK tend to be suboptimal. Vitamin D provides some level of photoprotection with higher Vitamin D levels at diagnosis associated with thinner tumours and better survival independent of Breslow and protecting against recurrence. It is no coincidence that the absorbance spectra for vitamin D synthesis matches the UVB wavelength exactly.
How can an outdoor lifestyle choice be enjoyed while minimising melanoma risk? A point of balance can be found, but it will require a rethink on behaviour and recreational exposure patterns. It may be more helpful to rely on natural protective mechanisms provided through eons of evolution matched to circadian rhythms being employed. Augmentation by artificial measures, certainly, but with an appreciation of their only limited protective ability.

