 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
UT Zierau*, L Martell, W Lahl
Saphenion® Vein Care Center Berlin/Rostock, Germany
Correspondence to: Zierau UT, Saphenion® Vein Care Center Berlin/Rostock, Germany
Received date: January 28, 2021; Accepted date: February 11, 2021; Published date: Febraury 18, 2021
Citation: Zierau UT, Martell L, Lahl W (2021) Vein Glue VenaSeal® for the Therapy in Case of Varicose Vein Thrombosis: A Case Report. J Med Res Surg 2(1): pp. 1-4. doi: 10.52916/jmrs214037
Copyright:©2021 Zierau UT, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
The thrombosis in areas of the superficial truncal varicose veins and cutaneous veins is not a rare complication; it requires drug or surgical therapy if the thrombosis grows in the direction of deep veins. This situation is particularly striking in the case of thromboses of the great saphenous vein GSV and small saphenous vein SSV as well as other saphenous veins and leads to deep vein thrombosis in around 20% of cases. We will report about a case of SSV thrombosis and the catheter-based therapy of thrombosis following the therapy of truncal varicose vein SSV with VenaSeal® in one session.
Varicose, VenaSeal®, Thrombosis
The thrombosis in the area of the superficial truncal veins and cutaneous veins (superficial venous thrombosis-OVT; thrombophlebitis) is not a rare complication; it requires drug or surgical therapy if the thrombosis grows in the direction of deep veins. This situation is particularly striking in the case of thromboses of the great saphenous vein GSV and small saphenous vein SSV as well as other saphenous veins and leads to deep vein thrombosis in around 20% of cases [1-5].
This deep vein thrombosis - in the case of the great saphenous vein it is the thigh/pelvic vein, and in the case of the small saphenous vein it is the knee vein, has a pulmonary embolism risk of up to 60% unless effective medical and/or surgical therapy is carried out immediately. Right now we have to note a highthrombosis rate as a result of the current Covid-19 pandemic, as viruses (e.g. Covid-19, HIV, influenza) also prefer to implant in the vein walls of the leg veins and there provoke inflammatory, thrombosis-inducing changes in the vein wall [6-8].In a current case, we saw a fresh thrombosis (approx. 7 days old) of the small saphenous vein in the course of a planned and carried out VenaSeal® varicose vein sealing on 3 saphenous veins on the operating table. The patient had no major complaints and was only able to describe a slight feeling of pressure when asked. The clinical findings were also completely normal. We decided to use a catheter to remove the fresh blood clots from the SSV and then to glue the veins as part of the planned varicose vein therapy. Of course, this therapy was accompanied by a drug-based thrombosis therapy, which is possible without any problems with the VenaSeal® procedure [9-14].
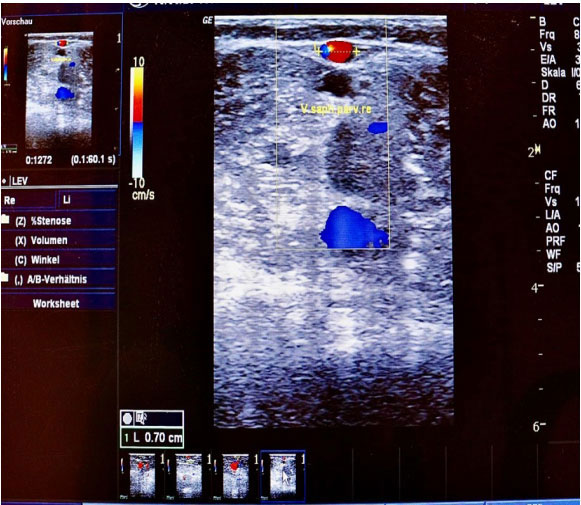 Figure 1: Preoperative sonography 6 months before therapy SSV varicose
vein without any phlebitis.
Figure 1: Preoperative sonography 6 months before therapy SSV varicose
vein without any phlebitis.The 54-year-old patient presented to us for the first time in June 2020. The anamnesis, clinical and ultrasound diagnosis revealed multiple varicose veins. Both the great saphenous veins and the right small saphenous vein were affected. We recommend the combination therapy using VenaSeal® on all 3 truncal veins simultaneously and then microfoam therapy of the lateral branches of varicose veins on both legs. The patient received an estimate for his insurance .
On 11th January 2021, minimally invasive therapy using VenaSeal® catheters took place. Simultaneous therapy was planned for all three affected truncal varicose veins. First, we ablated the two great saphenous veins in the normal supine position, then the patient turned around on his own. During the duplex sonographic examination of the SSV, we immediately noticed the previously described thrombosis of the truncal vein. The questioning of the patient, he was awake and had renounced sedation, revealed a slight feeling of pressure in the right lower leg for 3 days [15-18].
We decided, after clarification of the specific nature of the disease and the patient’s consent, to aspirate the fresh thrombus in the vein using the VenaSeal® sheath. The vein was probed with a guidewire and sheath up to its confluence with the deep knee vein. We sucked most of the blood clot out of the truncal varicose vein, after cleaning the sheath we then inserted the VenaSeal® Teflon catheter into the vein using the known technique and glued the varicose vein with the known technique. There were no problems with that. At the same time, the patient was given the adjuvant therapeutic dose of a heparin preparation over 7 days (Arixtra® 7.5 mg 1 × daily).
 Figure 2: Fresh thrombophlebitis in SSV in intraoperative sonography
Figure 2: Fresh thrombophlebitis in SSV in intraoperative sonography Figure 3: VenaSeal® introducer sheath and rest of thrombus material.
Figure 3: VenaSeal® introducer sheath and rest of thrombus material.The clinical and duplex sonographic follow-up examinations on the 1st and 7th the post-therapeutic day each produced inconspicuous subjective clinical and duplex sonographic findings. All veins were effectively closed, the patient is very satisfied and has no complaints. He started his professional activity on the first day after the intervention [19-22]. A further 7 days later, in accordance with our planned therapeutic procedure, we began with the microfoam therapy(sealing foam) of the lateral side branch varicose veins on both legs. As a rule, as in this special case, we start with the microfoam therapy of side branches and connecting veins about 14 days after the VenaSeal® therapy of the three truncal varicose veins.
 Figure 4: postoperative clinical picture, marker shows the catheter incision
point.
Figure 4: postoperative clinical picture, marker shows the catheter incision
point.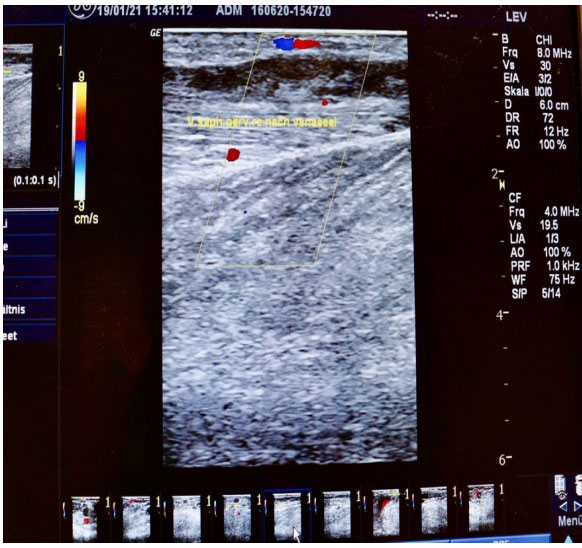 Figure 5: SSV sonography after sealing the vein
Figure 5: SSV sonography after sealing the veinIn the treatment of truncal varicose veins, catheter-supported procedures (laser, radio wave, VenaSeal®) have largely become established over the past 21 years and radical surgery has taken a back seat. This applies worldwide, but it must be said that in Germany these procedures are still not regularly reimbursed by statutory health insurances (except for special contracts with individual insurances). The VenaSeal® procedure is currently still the latest, although it was approved in Europe in 2011 and the USA in 2015 [23-25].
There are very few publications on the use of catheter procedures for thrombosed varicose veins. We had to go back to 2012 in our literature research. At that time, the Swiss colleague Prof. Markus Enzler published his experiences with the use of the laser catheter for varicose vein thrombosis. Our experience report on the use of the VenaSeal® system in the cases described is the first report on the problem, so our colleagues and the German Network VenaSeal® reported.
It can be said that the therapy of thrombosed varicose veins is primarily the healing and recanalization of the thrombosed areas by means of medicament therapy. Additional active intervention is only recommended if the appropriate technology and experience with the catheter systems are available. This procedure aims to shorten and alleviate the thrombotic changes in the varicose vein as well as absolute protection against deep vein thrombosis with possible pulmonary embolism [26-27].
The VenaSeal® system is initially not approved for the treatment of thrombosed varicose veins. Nonetheless, with the existing catheters and locks, it is quite possible and useful to first suction off the soft thrombi in the case of fresh thromboses in the truncal varicose vein with the lock system to avoid complications. The defective “varicose vein” can then be effectively closed immediately. The long-term closure rate of the VenaSeal® system is >96% over an observation period of more than 8 years.
So far, we have not seen any side effects or complications in our treated patient. The convalescence was adequate to the process, and the follow-up treatment can also be carried out following our normal Saphenion® standards. It should be noted, however, that the Venaseal® catheter was not primarily designed for therapy of varicose vein thrombosis and therefore each of these interventions is initially reserved for individual cases.
There are no conflicts of interest

