 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Faruk Hernández Sampayo1*, Gabriela Carvajales Lozano2 , María Yuliana Amell Wilches3
1 General Surgeon, Universidad Metropolitana de Barranquilla, Colombia
2 General Physician, Universidad del Norte de Barranquilla, Colombia
3 General Physician, Universidad de Sucre, Colombia
Correspondence to: Faruk Hernández Sampayo, General Surgeon, Universidad Metropolitana de Barranquilla, Colombia.
Received date: November 05; 2021; Accepted date: November 19; 2021; Published date: November 26; 2021
Citation: Sampayo FH, Lozano GC, Wilches MYA (2021) Tubo-Ovarian Inguinal Hernia with Ruptured Bleeding Follicle: A Case Report. J Med Res Surg 2(5): pp. 1-2. doi: 10.52916/jmrs214060
Copyright: ©2021 Sampayo FH, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License; which permits unrestricted use; distribution and reproduction in any medium; provided the original author and source are credited.
Introduction: Hernias are abnormal protrusions of any abdominal-pelvic or fat organ, which are produced by a defect in the abdominal wall, the most frequent are inguinal hernias and their content is generally of the omentum or intestinal loops, the presence of pelvic organs is very infrequent and the majority of cases described are in children under five years of age.
Objective: To analyze the entity in connection with a case of a patient with a tubo-ovarian inguinal hernia.
Clinical case: The case of a 34-year-old female patient is presented, who was under follow-up by the gynecology service due to the presence of a left ovarian cyst, with symptoms of pain in the left iliac fossa for more than 6 months of evolution. which is performed an ultrasound, which reports left inguinal hernia for what is electively scheduled by the general surgery service, when performing the herniorrhaphy incarcerated hernia with left ovary with bleeding follicle and fallopian tube is evidenced.
Conclusions: These types of findings are infrequent, documented in the literature with a global incidence of Tubo-ovarian inguinal hernias ranging from 0-8-4.4%, however it is worth clarifying that these studies are in infant patients, so its presentation in adults associated with a hemorrhagic follicle is anecdotal as in this case.
Keywords: Inguinal Hernia, Tubo-Ovarian Hernia, Bleeding Follicle
An inguinal hernia is defined as an abnormal protrusion of the viscera, omentum or fat that occurs through the inguinal canal, due to a defect in the abdominal wall, its etiology is multifactorial, it can occur due to chronic increase in intra-abdominal pressure, heredity, smoking, muscle weakness among other factors [1].
Currently, inguinal hernia is one of the main reasons for consultation in general surgery, corresponding to 70-75% of all hernia surgeries and represents approximately 2.000.000 surgeries per year [2]. Being a more frequent pathology in men than in women. Generally, the content of the hernial sac is omentum or intestine segments, but unusual content such as the urinary bladder, Fallopian tubes, ovaries, cecal appendix, among others, may also be present. In this article we will present a case of a patient of childbearing age, with a tube-ovarian inguinal hernia, confirmed by histopathological examination, a rare entity with a global incidence between 0.8-4.4%, however it is worth clarifying that these studies are in infant patients, so its presentation in adults associated with a hemorrhagic follicle is anecdotal, as in this case [3].
A 34-year-old female patient with a history of dyslipidemia, who consulted the gynecology service due to pain in the hypogastrium and left iliac fossa, with ultrasound that reported the presence of a simple cyst of the left ovary; received conservative management with ultrasound follow-up for 6 months, in his last ultrasound they reported that it was not possible to show the left ovary due to abundant meteorism, however, given the persistence of symptoms and the appearance of a small protrusion at the left inguinal level 4 months later, they requested ultrasound with emphasis on inguinal region which reports a defect at the level of the abdominal wall at the level of the left inguinal region of approximately 9 mm, mobile, through which hypoechoic material protrudes that appears to correspond to fat, findings compatible with left inguinal hernia, therefore The patient is referred to the general surgery service where they decide to program for a left inguinal herniorrhaphy due to clinical and imaging findings.When performing the surgical procedure, the patient is found to be incarcerated left inguinal hernia, her sac contained an ovary and a left tube, and a ruptured follicle is evident in the ovary. bleeding, which deforms itself (Figure 1) for which it was decided to perform unilateral salpingo-oophorectomy by laparotomy, a sample was sent for histopathological study; the patient is hospitalized for post-surgical surveillance, which progresses favorably, so she is discharged two days after surgery, the patient returns to the consultation with a result of pathology that concludes with a left ovary with a hemorrhagic cystic corpus luteum+fallopian tube with a simple cyst+hernial sac.
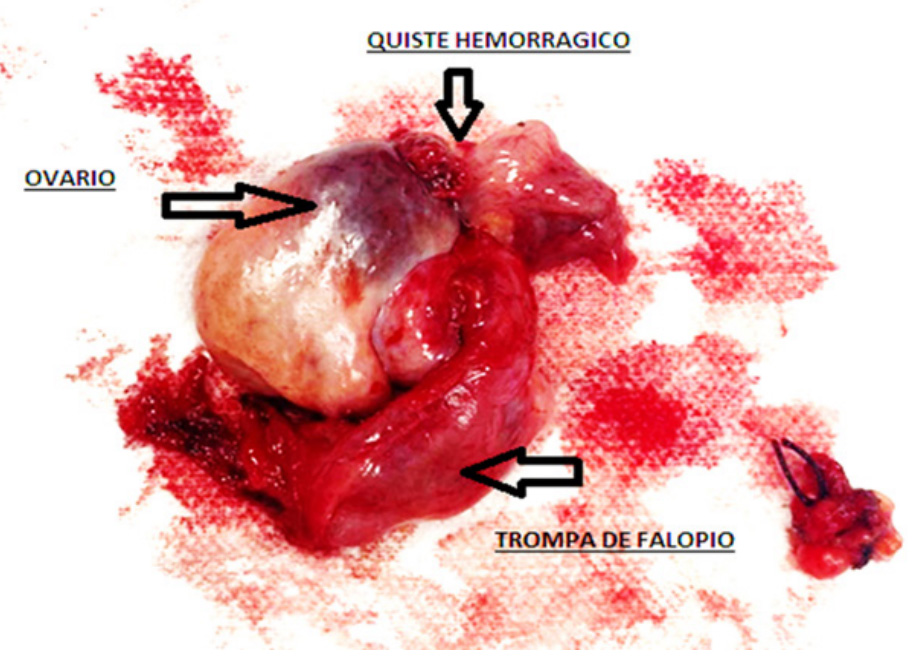 Figure 1: : Hernial sac content: left ovary with hemorrhagic cystic corpus luteum+fallopian tube with simple cyst.
Figure 1: : Hernial sac content: left ovary with hemorrhagic cystic corpus luteum+fallopian tube with simple cyst.Hernias of the abdominal wall are composed of a peritoneal sac that protrudes through a defect in the muscular layers, they are produced by a congenital or acquired defect, they occur in 40 to 51% in the most productive ages of the individual, being more frequent in men than in women, in a 3:1 ratio, by location inguinal hernias represent the majority of cases in 75% [4].
Inguinal hernias that contain attachments are very rare, in the literature there are no clear data on their epidemiology, a literature review was carried out until 2018 of the literature where the described cases of inguinal hernia that contained ovaries were searched and only found in 17 case reports, a prospective study was also conducted where unusual hernia contents were documented, including 1,950 inguinal hernias, with a reported incidence of 2.9% of patients with sacs that included fallopian tubes and ovaries. 9 Most of the Tubo-ovarian hernias have been reported mainly in childhood in 71% in girls under 5 years of age, associated with embryological disorders and anomalies of the genital tract.
The etiological mechanisms by which inguinal hernias are formed are very diverse, we find anatomical factors such as the persistence of the nuck duct in women or the vaginal peritoneal duct in men, absence of aponeurotic fibers in the transverse muscle of the abdomen, poor occlusion of the internal inguinal orifice by the muscular layers that lead to an enlargement of the dimensions of the inguinal floor, which added to the increase in intra-abdominal pressure is one of the main causes in the genesis of the inguinal hernia [5]. There are also biological factors such as structural collagen alterations, which are generally hereditary, and acquired factors such as senility, obesity, malnutrition, diseases that cause a lot of coughing and lifestyle [4]. The hypotheses suggested for the presence of tuboovarian hernias mention the weakness of the broad ligaments or the suspensory ligaments of the ovary [6].
Our patient is a 34-year-old female, G2P2, with a history of dyslipidemia, managed by the gynecology service due to the presence of a left adnexal cyst, under ultrasound follow-up, who six months later presented herniation of said ovary through the inguinal canal. Fortunately, it was approached early for the general surgery service, where they decide to schedule the surgery, finding as an incidental finding the presence of an ovary with a bleeding follicle and a left tube with a simple cyst. When these types of hernias that contain ovaries occur, the treatment must be given early the risk of torsion is increased and more if there is incarceration that can happen in up to 33-43% [7]. The surgical procedure seeks to preserve the organs and restore blood flow, a delicate release of these since they can have firm adhesions, however in cases where there is incarceration, it is recommended to resect the organs compromised, as in the case presented, where the resection was motivated by the finding of an incarcerated hernia and the hemorrhagic content that was found within the sac as a result of the rupture of the follicle, subsequently documented by histopathological study.
The presence of an inguinal hernia with a sac that contains ovaries and fallopian tubes is very rare, however it should be noted that since hernioraphy is one of the surgical procedures performed in the daily practice of surgeons, it is likely that more than once may face these findings in their professional career and this may pose a difficulty in the approach and decisionmaking, so it is important to know the inguinal canal in detail, especially in women where the inguinal canal is less delimited than in men. The preservation of the organs should always be tried, however, in the face of chronic incarceration and severe affection of the tube and ovary, its resection is better to avoid future complications such as abscess or residual bleeding.
The author declares there is no conflicts of interest.
No funding.
1. Pablo BM, Luis GO, Patricio PS (2005) Fisiopatología de la hernia inguinal primaria, algo más que un fenómeno mecánico. Revista Chilena de Cirugía [en linea] 57(5): pp. 432-435.
2. Hermida PAC, Zamarra DRB, Nope CG, et al. (2017) Incidencia y factores asociados al dolor crónico postoperatorio en pacientes llevados a herniorrafia inguinal. Revista Colombiana de Anestesiología 45(4): pp. 291-299.
3. Thomas AK, Teague CT,Jancelewicz T (2018) Canal of Nuck hernia containing pelvic structures presenting as a labial mass. Radiol Case Reports 13(3): pp. 534-536.
4. https://www.amhernia.org/wp-content/themes/amhernia2/files/guias2015.pdf.
5. Malik KA, Al Shehhi RM, Al Qadhi H, et al. (2012) Ovarian Hernia: A rarity. Sultan Qaboos Univ Med J 12(2): pp. 225-227.
6. van Heesewijk HP, Smith FW, Heitbrink MA, et al. (2019) Herniation of an Ovarian Cyst Through the Inguinal Canal: Diagnosis with CT. Am J Roentgenol 154(1): pp. 202-203.
7. Takezoe T, Sato K, Watanabe T, et al. (2018) A female infant with an inguinal hernia containing the uterus and bilateral ovaries. J Ped Surg Case Reports 3: pp. 46-47.
PDF Google Scholar 10.52916/jmrs214060
