 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Yulia Bogdanova Peeva*
Associate Professor at the Department of Social Medicine and Public Health, Faculty of Public Health, Medical University, Plovdiv, Bulgaria.
Correspondence to: Yulia Bogdanova Peeva, Associate Professor at the Department of Social Medicine and Public Health, Faculty of Public Health, Medical University, Plovdiv, Bulgaria.
Received date: February 14, 2023; Accepted date: February 25, 2023; Published date: March 04, 2023
Citation: Peeva YB. Treatment Plan and Discussions of Class I with Smilestream: A Case Report. J Med Res Surg. 2023;4(1):12-16. doi: 10.52916/jmrs234099
Copyright: ©2023 Peeva YB. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted
use, distribution and reproduction in any medium, provided the original author and source are credited.
The aim of the study was to present a Class I case and the treatment plan related to orthodontic diagnosis. The chief complaint of a patient and his parents are crowded teeth upper and lower and anterior crossbite. “@I’m looking like a crocodile” were the first words of the boy sitting on the dental chair. The main task was functional but also esthetics because it was from the first important to him. The treated malocclusion is characterized with a narrow maxillary width and prominence of the mandible. The maxilla was deficient in anteroposterior and transverse dimensions, causing a slightly concave and unpleasant profile, a crossbite relationship of lateral incisors and upper and lower anterior crowding. The use of mechanics was preferred and accepted as a better solution for the patient according to the idea to generate well directed growth. The patient was 12 year-old boy with Class I malocclusion and anterior crossbite. A molar and canine class 1 and correction of the malocclusion were obtained. The improvement of facial aesthetics and smile enlarging were also ensured.
Orthodontic, Crossbite, Retroclination, Aesthetic improvement
Patient and his parents are living in 100 km distance from the dental practice. For the Bulgarian scale map, it’s not a small distance, so the patient takes my respect for his motivation. Unfortunately, his motivation is external, which means, it comes generally from his mother.
Something the doctor is obliged to know is the profession and social status of the parents because it may affect in addition the treatment process. The family is actively sportsmen who are much disciplined in personal plan; so, probably they’ll follow advices and requirements of the doctor. Before the patient's subjective feeling of a disease or not, of a condition or not, there is awareness. Orthodontic treatment is a complex impact on the part of the orthodontist (sometimes combined with surgery) on the dental structures, the underlying soft tissues and the shaping of the maxillofacial bones [1-3]. Its success also depends on other factors:
According to them, the following basic principles are laid down in health education:
It is a significant process in the patient-physician relationship. It’s important for the awareness of the patient from one side, but it also protects the doctor during the treatment. Informed consent is written document which is necessary to be read, understand and signed by the parents. The patient was informed about the potential risk for the dental structures during the orthodontic treatment: • Tooth decalcification: the lack of appropriate oral hygiene during the treatment. The most common damage to the tooth surface • Root resorption: additional X-ray can be requested to check periodically the condition of the tooth roots • Bone or tooth lose: gingivitis or periodontitis with a loss of supporting structures • Gingival recession: lack of good dental care can lead to gingival recession • TMJ symptoms • Surgery • Fees
Fixed appliance treatment can lead to the improvement of functional and esthetical problems of the patient. Nowadays, patients more than ever demand orthodontic treatment to get it because of improvement of their smile and facial profile. Evaluating the problem list, extra-oral examination and treatment objectives the doctor can differ a lot of problems related to the skeletal and dental issues. The patient, from the other side is not able to recognizeall of this, so the orthodontist is obliged to ask for the main compliant in order to check and to solve this problem (Figure 1). It can lead to higher satisfaction from the treatment because this is the reason he is coming to the dental practice. So, patient and family concern are: • Crowded teeth • Anterior crossbite • TMJ problems • Esthetics • (During the treatment always ask about the hygiene. It’s well visible from the photos that he has a problem with soft tissue)
Once a patient’s orthodontic problems have been identified, four issues must be faced in determining optimal treatment plan: • The timing of the treatment • The complexity of the treatment that would be required • The predictability of success with a given treatment approach • The patient’s (the parents) goals and desires [7]
G. M. has a dolicofacial facial pattern with a straight profile and average width of nose and mouth. The upper midline is centered relative to the facial midline but the lower deviated to the left with 1.5 mm. The lips are average, the sublabial fold average and the nasio-labial angle is greater than 110°. The patient had no relevant prenatal, natal, postnatal history, history of habits, medical or a family history and allergies.
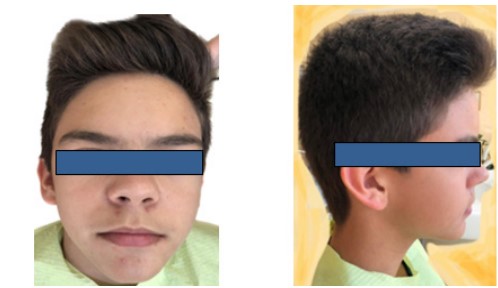 Figure 1: Pretreatment records of a 12-year boy with anterior crowding exhibiting dental Class I.
Figure 1: Pretreatment records of a 12-year boy with anterior crowding exhibiting dental Class I.The lip competency was adequate, without efforts, with lip tonicity being normal. A slight shift of the lower lip to the left is observed, which can be interpreted as asymmetry. Breathing was observed to be normal.
On the left side early clicking was noted. The patient and his parents do not report any TMJ problems.
Initial records and intraoral examination on frontal view showed presence of crowding in the maxillary and mandibular anterior region. The mandible is shifted to the patient’s left with 2 mm. The frontal view shows also crossbite of maxillary right lateral incisor. On lateral right patient showed presence of Class I incisor, canine and molar relationship and canine Class II relationship in left and Class I in molars. It can be seen also an average overjet and overbite; proclined and forwardly placed upper and lower anterior teeth. The occlusal view showed presence of maxillary and mandibular lower anterior crowding with multiple rotated teeth seen in lower and upper arch. Both arch presence “U”-shaped form. Dental crowding was estimated in 6 mm in the upper arch and 7 mm for the lower. The vertical dimension is dental average. The supporting structures show obvious problem with the lack of hygiene.Midline discrepancies are among the most complex and commonly seen problems in clinical orthodontics (Figure 1-4) [8].
 Figure 2: Pre-treatment intra-oral photographs.
Figure 2: Pre-treatment intra-oral photographs. Figure 3: Straight view and upper and lower study models.
Figure 3: Straight view and upper and lower study models. Figure 4: (a): Right side molar 1 mm class I, canine class I; (b): left side: molar class I, canine 2 mm class II.
Figure 4: (a): Right side molar 1 mm class I, canine class I; (b): left side: molar class I, canine 2 mm class II. Figure 5: No missing teeth. All of the permanent teeth present except 8 s. Fan-shaped lower incisors. Insufficient place for the eruption of 13. Possible relapse with the crowding of lower incisors after the eruption of lower 8 s.
Figure 5: No missing teeth. All of the permanent teeth present except 8 s. Fan-shaped lower incisors. Insufficient place for the eruption of 13. Possible relapse with the crowding of lower incisors after the eruption of lower 8 s.A second consultation was held, at which time several treatments were considered possible, including non-extraction. The estimated time of treatment was 18-24 months, with an estimated fee of €XXXX for the braces, monthly payment of €XX and €XXX for both retainers. The findings at the clinical examination were consistent with the patients’ chief complaint of crowding. When asked about the perception of protrusion, the patient’s opinion was: acceptable now, can move the teeth forward (Figure 5).
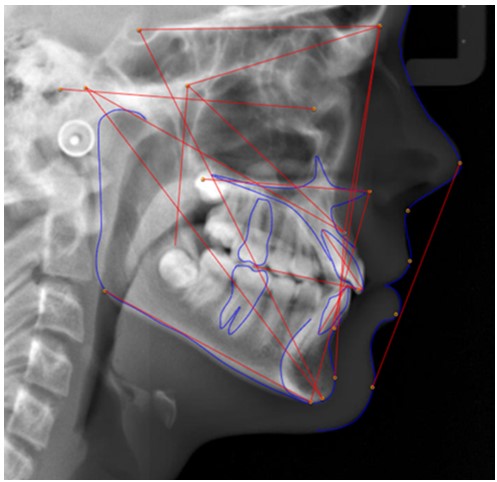 Figure 5: Start lateral ceph.
Figure 5: Start lateral ceph.|
|
Pre-treatment |
Post-treatment |
|
SNA |
79.5 °(deficient); |
81° |
|
SNB |
80.7 °(average) |
80° |
|
ANB |
-1.2 ° (indicates that the upper jaw is retruded because of the lack of space and infra position of 13) |
1° |
|
Wits |
-4.1 (Class III, more skeletal resistance can be expected); |
-1° |
|
FMA |
24 ° (average) |
25° |
|
Upper 1 to SN |
122.9° (proclination, the normal value is 103°+/- 6°) [9] |
114° |
|
Interincisal Angle |
115.6 ° (135°+/- 5.8 is normal, proclined incisors; Best Finish 125 to 130) |
116° |
|
Lower 1 to MP |
92.3° (lower I inclination, average, protruded) |
92° |
|
Upper 1APo |
8.3 mm (2.7+/- 1.8 is normal) |
4.2 mm |
|
Naso-Labial Angle |
123.87 |
115 |
The Skeletal vertical dimension is average with a dental average bite. At the time of initial evaluation, growth was expected for this patient. The maxilla is positioned in retruded position, and the mandible is average. The relationship of the upper and lower jaws is Class III based on evaluation of the ANB and Wits measurements. The lower incisors are average with the antero-posterior position being average. The upper incisors are proclined with the antero-posterior position being average. Based on the cephalometric evaluation, the initial clinical impressions, and the patients’ feelings about the position of his teeth, a treatment objective has been decided to leave the incisors near the starting position.
The lower archform was selected to maintain the ovoid medium dental archform. The upper archform was selected to expand the dental archwire.
A flat splint was prepared that removed the bad occlusion with the crossbite on 12,22 and helped the lower fit the upper. He has complaints for 1 week and there was NO MORE PAIN –splint was discontinued after 6-7 weeks (Figure 6 and Figure 7).
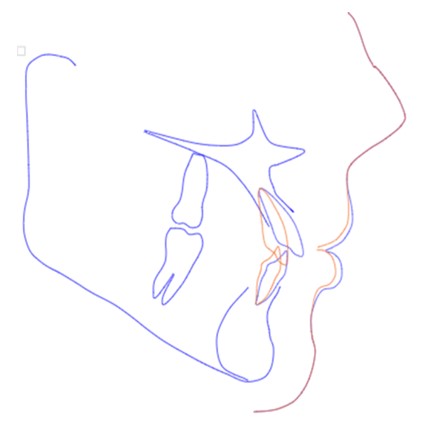 Figure 7: Non-extraction VTO with alignment. The proclination of the upper and lower incisors was solved with dental VTO.
Figure 7: Non-extraction VTO with alignment. The proclination of the upper and lower incisors was solved with dental VTO.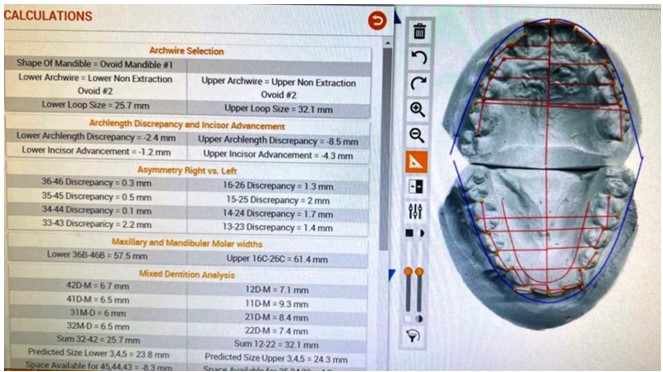 Figure 8: Calculations and treatment decision options.
Figure 8: Calculations and treatment decision options.The final decision is that Class I Non-extraction. 002 Limit lower incisor advancement, standard wire progression (Figure 8).
 Figure 9: Final facial picture sent by mummy. Happy patient, happy all.
Figure 9: Final facial picture sent by mummy. Happy patient, happy all.Smile is more important today than ever because it can prove not only the function and esthetics but the quality of life in general. And these positive outcomes are visible only for one reason. Because of smiling, the scientific results show that better carrier, perfect partner or things which can happens easier or even though the healthy years Expectancy indicator depends from how much per day the individual smile or laugh.
We have no known conflict of interest to disclose.
The consent was taken from the patient.
No.

