 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Barry TI1, Diakité SY2*, Sow Z1, Diallo AA1, Koundouno AM3, Bah IK4, Touré A5, Diallo AT5, Diallo B1
1Department of Visceral Surgery, Donka National Hospital, Guinea.
2Department of Visceral Surgery, Conakry Enta Nord Regional Hospital, Guinea.
3Department of Surgery, Kankan Regional Hospital, Guinea.
4Department of Gynecology-Obstetrics, National Hospital Ignace Deen, Guinea.
5Department of General Surgery, National Hospital Ignace Deen, Guinea.
Correspondence to: Diakité SY, Department of Visceral Surgery, Conakry Enta Nord Regional Hospital, Guinea.
Received date: August 18, 2024; Accepted date: August 27, 2024; Published date: September 4, 2024
Citation: Barry TI, Diakité SY, Sow Z, et al. Torsion of Right Paratubal Cyst Discovered During Appendectomy about an Observation at Conakry University Hospital: A Case Report and Review of the Literature. J Med Res Surg. 2024;5(4):98-100. doi: 10.52916/jmrs244145
Copyright: ©2024 Barry TI, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Introduction: The paratubal cyst is a latero-uterine mass independent of the ovary, tubular, with thick, hypervascularized walls. It may be responsible for progressive complications such as Fallopian tube torsion.
Observation: Mrs FBD, 52 years old, admitted for abdominal pain in the Right Iliac Fossa (RIF) with episodes of fever. Course: 3 days. Past history: gastritis. Gestites: 5, parity: 4, alive: 4, dead: 1.
Examination: general condition satisfactory, integument and mucous membranes normocolored. BP=120/70. Temperature: 36°C, pulse: 80/min. Symmetrical abdomen participates in breathing, painful in IDF with parietal defense. Audible peristalsis. Pelvic touch was unremarkable. The rest of the examination was unremarkable. Biology: inflammatory biological syndrome: hyper leukocytosis (17.60G/L) with 84% neutrophils (14.78G/L). Through an approach in the lower abdominal fold, appendectomy followed by detorsion and right paratubal cystectomy. Good postoperative outcome.
Conclusion: Paratubal cysts and their complications are rarely diagnosed preoperatively. In our case, the diagnosis was made intraoperatively. Treatment consisted of right paratubal cystectomy with ovarian conservation.
Cyst, Paratubal, Torsion, Diagnosis, Treatment.
The paratubal cyst is a latero-uterine mass independent of the ovary, tubular, thick-walled and hypervascularized [1]. It can cause progressive complications such as torsion of the fallopian tube, which is difficult to diagnose [2]. We report a rare case of right tubal cyst torsion with necrosis of difficult diagnosis, discovered intraoperatively during an appendectomy.
Mrs FBD, 52 years old, housewife, admitted for abdominal pain in IDF with episodes of fever. Course: 3 days. History: gastritis. Gestites: 5, parity: 4, alive: 4, dead: 1. Examination: general condition satisfactory, integument and mucous membranes normocolored. BP=120/70. Temperature: 36°C, pulse: 80/min. Symmetrical abdomen participates in breathing, painful in IDF with parietal defense. Audible peristalsis. Pelvic touch was unremarkable. The rest of the examination was unremarkable.
Inflammatory biological syndrome: hyperleukocytosis (17.60G/L) with 84% neutrophils (14.78G/L). Abdominopelvic ultrasound suggested uncomplicated appendicitis.
Horizontal laparotomy in the lower abdominal fold, aspiration of odourless brown peritoneal fluid (150cc), demonstration of a large appendix covered with false right iliac membranes. Appendectomy without stump burial plus mesoplasty. Exploration of the right adnexa revealed a right adnexa with a twisted, necrotic paratubal cyst with two anticlockwise turns (Figures 1,2). Detorsion then cystectomy with conservation of the right ovary, which was macroscopically unremarkable.
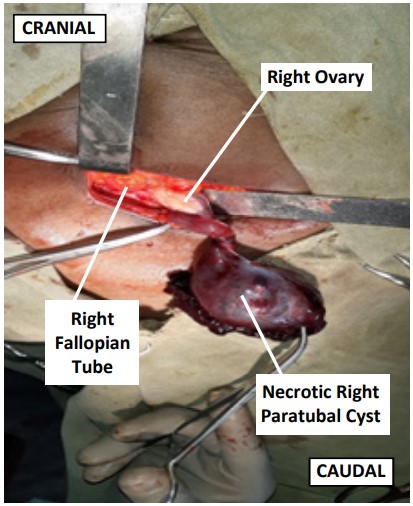 Figure 1: Twisted and necrotic right paratubal cyst (operative view).
Figure 1: Twisted and necrotic right paratubal cyst (operative view). Figure 2: Surgical specimen of right paratubal cyst twisted and necrotic.
Figure 2: Surgical specimen of right paratubal cyst twisted and necrotic. Figure 3: Appendectomy operative specimen.
Figure 3: Appendectomy operative specimen.Post-operative course was favourable. The patient was reviewed after 1 year with no particularities.
The paratubal cyst is a frequent pathological entity. It accounts for 10% of adnexal masses [1]. The age of onset is 30 to 40 years, but there are cases in postmenopausal women, as in the case of our 50-year-old patient.
Symptoms depend on the evolution of the cyst. The clinical symptoms of a torsion of a paratubal cyst may be pain in the IDF with a sudden onset, continuous or rapidly worsening. Pelvic touch reveals lateralized pain over a painful mass on pelvic palpation (Warneck's sign). This mass corresponds to the twisted pedicle, difficult to identify by rectal examination [4]. Evolving complications include haemorrhage, rupture and torsion. In our case, the torsion was discovered intraoperatively. These cysts are fortuitously diagnosed intraoperatively for other diagnoses [5]. In our case, the diagnosis of acute appendicitis was made preoperatively.
Ultrasound was used to make a differential diagnosis with a peritoneal inclusion cyst [12], acute appendicitis or EP. Abdomino-pelvic Computed Tomography (CT) is of vital importance in cases of obesity. It enables positive diagnosis and excludes other causes of pain (appendicitis) [12].
In our case, preoperative abdominopelvic ultrasound was not helpful in diagnosing the pa cyst. Early diagnosis is essential to preserve ovarian function in the future. Treatment is surgical. It consists of detorsion and cystectomy, as in our case.
Our patient would have benefited from laparoscopy, but the latter is not available in the hospital. The circumstances of diagnosis are preoperative and intraoperative. Preoperatively, the diagnosis can be evoked on the basis of clinical data (sudden painful mass in the IDF) and imaging data, notably the CT scan, which confirms the presence of a twisted cyst with or without necrosis. In our case, the diagnosis of acute appendicitis was evoked preoperatively on the basis of clinical data (abdominal pain in the IDF, fever, parietal defense) and paraclinical data (PNN hyperleukocytosis). the diagnosis of acute appendicitis. The diagnosis of a twisted para-tubal cyst was therefore made intraoperatively. In our case, the appendix was pathological (phlegmonous). Anatomopathological examination concluded to a tubal cyst without signs of malignancy and a suppurated appendix. The differential diagnosis of the cyst must be made with acute appendicitis (progressive nature of pain and fever), Extra-Uterine Pregnancy (EUP) (BHCG assay and pelvic ultrasound are contributory), urinary tract infection (ECBU), salpingitis (presence of pathological leucorrhoea). An abdominal CT scan in our case would certainly have enabled us to evoke the diagnosis of a twisted tubal cyst preoperatively, as is the case in the study by Bouguern et al [4].
Complications of paratubal cysts include rupture, haemorrhage and torsion [15]. In our case, the torsion evolved over 72 hours.
The classic causes of isolated tubal torsion are parovarian or tubal masses [6]. This is the case of Bouguern et al [4]. Other causes include hemosalpinx, hydrosalpinx, tubal adhesions and tubal plasty. The main organic cause is excess mesosalpinx length (tube length >12 cm) [14]. There are also hemodynamic causes which result in veins being longer and more flexible than arteries [14]. In our case, laparotomy revealed a right paratubal cyst torsion with necrosis on hydrosalpinx. Paratubal cyst torsion is treated surgically. It consists of detorsion, assessment of recoloration and cystectomy. If there is no recoloration, salpingectomy is indicated. In our case, after detorsion, there was progressive recoloration, followed by cystectomy, which enabled us to preserve the right tube and ovary. The contralateral adnexa was unremarkable.
The patient should be monitored clinically and ultrasonographically, and informed about the contralateral adnexa. Laparoscopy is a preferred approach used by many teams, especially in cases of co-morbidities (obesity, hydronephrosis) [9,10]. In our case, laparoscopy is not available at our university hospital. When possible, laparoscopy has the advantage of reconciling the diagnosis with that of ovarian cysts [10]. Treatment should be as conservative as possible, as in our case.
The diagnosis of paratubal cysts and their complications (torsion) is rarely made preoperatively. Our observation showed that the diagnosis of a twisted paratubal cyst was made intraoperatively by exploring the right adnexa during appendectomy. Imaging (ultrasound or abdominal computed tomography) can contribute to the diagnostic approach for better therapeutic management.
Author declares there is no conflicts of interest.
No source of funding.

