 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Siddharth Sonwane1* , Shweta Rajendra Kamble2
, Shweta Rajendra Kamble2
1Professor and Head, Department of Orthodontics, Mansarovar Dental College, Bhopal, Madhya Pradesh, India.
2Associate Professor, Department of Oral and Maxillofacial Surgery, Government Dental College, Nagpur, Maharashtra, India.
Correspondence to: Siddharth Sonwane, Professor and Head, Department of Orthodontics, Mansarovar Dental College, Bhopal, Madhya Pradesh, India.
Received date: July 08, 2023; Accepted date: July 24, 2023; Published date: July 31, 2023
Citation: Sonwane S, Kamble SR. The Management of Vertical Maxillary Excess with Orthodontic Mini Screws to Achieve a Pleasant Smile: A Two Year Follow Up Case Report. J Med Res Surg. 2023;4(4):80-83. doi: 10.52916/jmrs234114
Copyright: ©2023 Siddharth S, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted
use, distribution and reproduction in any medium, provided the original author and source are credited.
Background: In gummy smile subjects with short clinical crown periodontal surgeries are the classic
essential aesthetic approach. However, in gummy smile caused by vertical maxillary excess Le Fort I
osteotomy, but patient refuse to go for Le Fort I osteotomy, then orthodontic treatment alone doesn’t
restore the complete esthetic. Currently mini screw with orthodontic treatment is the best choice.
Objective of Case Report: To determine the outcome of gummy smile managing with orthodontic
treatment and mini screw.
Methodology: A 35-year-old female patient with skeletal class II malocclusion, convex profile, and
noticeable gummy smile. The case was treated with first premolar extraction and mini screw for intrusion
and retraction. Followed by plastic periodontal surgery to increase crown length and accumulated
gingival overgrowth.
Conclusions: The case was completed with class I malocclusion with restoring acceptable gum visibility.
Gummy smile, Plastic periodontal therapy, Orthodontics, Orthognathic surgery, Vertical maxillary excess.
The term Gummy Smile (GS) is defined as "gum exposure of 3 to 4 mm in a smile" [1]. This is known as a gummy smile, and about 10% of the population between 20 and 30 years of age present excessive gingival display, which is more prevalent in women [1-2]. 7% of the 10% gingival exposure self-reduces by forceful closure of the upper and lower lip by reducing incisor display [3].
The etiological factors of a gummy smile are Hypermobile Upper Lip (HUL), Altered Passive Eruption (APE), Vertical Maxillary Excess (VME), Dentoalveolar Extrusion (DAE), and Gingival Hyperplasia (GH) [1-4]. There are two phases of tooth eruption: active tooth eruption and altered passive tooth eruption. In the active tooth eruption phase, the gingival tissue migrates towards the apical area of the erupting crown, which results in full clinical crown visibility4. However, in APE, the gingival tissue is unable to migrate apically, resulting in a squarish shape and more Gingival Display (GD). Anterior dentoalveolar extrusion causes maxillary incisor overeruption and increased gingival display due to coronal gingival margins [5]. The role of HUL in GS is not clear due to scanty literature reports. VME is the most common cause of GD. In VME, excessive growth of the maxilla and dentoalveolar structures occurs in an inferior direction, which can occur in the entire maxilla, posteriorly or anteriorly. This condition may result in a long face, a gummy smile, and an open bite. Furthermore, in VME, pseudo-incisor over eruption and short upper lip length are most commonly seen, but cephalometric evaluation confirms that both incisor display, and upper lip length are normal. Thus, excessive GD is considered unaesthetic and has a negative impact on a subject's oral health-related quality of life, including aspects of functional limitation, psychological discomfort and disability, and social handicap [1-7].
Management of GS is purely based on its underlining cause, but in most of the subjects, GS is multifactorial, such as VME, APE, and HUL. In this condition, a multi-disciplinary approach is required such as lip repositioning, crown lengthening, by periodontist and orthognathic surgery and incisor intrusion by orthodontist [7].
Presently, a case of such multifactorial aetiology has been reported to the department of orthodontics, with the chief complaint of excessive gum display and forwardly placed upper incisors. The objective of this case report is to determine the impact of simultaneous intrusion and retraction using an orthodontic screw in the management of GS. This case report aimed to highlight the side effects of simultaneous intrusion and retraction using an orthodontic screw to bypass orthognathic surgery in VME.
A 35-year-old female presented with a chief complaint of forward-placed teeth and excessive gummy display. A meticulous examination revealed that it was bimaxillary protrusion, a gummy smile, lip incompetence, and short clinical crowns. For accurate diagnosis, the patient was referred to oral diagnosis for lateral cephalogram and orthopantomogram radiographs.
Lateral cephalometric evaluation (Table 1) determined that protrusion of maxillary base with protrusion of dentoalveolus of mandibular jaw, creating convex profile, protrusion of lips, proclination of upper incisors and an exaggerated maxillary gingival show when smiles. On profile analysis reveals that increased nose length, flat zygoma and decreased alar base; also, lower third of the face was more than two third. Thus, the overall cephalometric evaluation reveals that the subject was diagnosed as skeletal class II malocclusion with bimaxillary dentoavelar proclination with increased lower height of facial height, an incompetent lip, and a noticeable Gummy Smile (Figure 1).
Table 1: Cephalometric pre-treatment values.|
Measurement |
Normal value |
Pre-treatment |
|
Skeltal |
||
|
SNA |
82 |
83 |
|
SNB |
79 |
76 |
|
ANB |
2 |
6 |
|
FMA |
23 |
32.3 |
|
Z-Angle |
60 |
56.5 |
|
Dental |
||
|
Overbite (mm) |
1.8 |
3.5 |
|
Overjet (mm) |
3.5 |
3 |
|
FMIA |
59.8 |
59.7 |
|
1-FH |
116 |
114.5 |
|
Inter-Incisol |
123.8 |
125.1 |
|
Soft-tissue |
||
|
Upper lip-E line |
-0.9 |
-0.5 |
|
Lower lip-E line |
0.6 |
0.5 |
 Figure 1: Pre-treatment.
Figure 1: Pre-treatment.
This case was planned to be treated orthognathically, as per the cephalometric analysis. However, the subject was not interested in orthognathic surgery so, the treatment plan was changed to camouflage treatment plan. In this we decided to extract upper first maxillary premolars and lower second premolars. As the incisor crown length was clinical under normal, we decided to retract and intrude anterior maxillary segment with orthodontic mini screws.
Following the extraction of upper first premolars and lower second premolars with absolute anchorage preparation, using the 0.022 × 0.028 Roth (dentos bracket) bracket systems case was strapped up, and a 014" NiTi wire was used in both archways along with lace back and cinch back distal to the first molars. Every month, in a sequence of 014", the wire changing routine was followed. The prefabricated arch wires were used with sequence of Nitinol (NITI) wire 0.014, 0.016, 0.018. With these sequence of wire teeth was aligned and leveled for next phase.
Total time lapsed for leveling and alignment was five months, later, under submucosal local anesthesia in between second premolar and first molar of maxillary arch minis crews of 2mm dimeter and 8 mm length was inserted into maxillary arch for intrusion and retraction. 0.019 × 0.022 stainless steel wire was used as base wire for retraction and intrusion. And 3mm closed coil spring was used from min screw to distal of lateral incisor where retraction hooks were crimped. This procedure took seven months to complete the extraction space closure and intrude/ shorten anterior maxillary length.
 Figure 2: After space closure.
Figure 2: After space closure.
Total time lapsed for intrusion and retraction was 18 months from date of strap up. The objective achieved was leveling and alignment of teeth, reduced gummy smile and class I malocclusion. However, we found that reduced clinical crown lengths, gingival overgrowth and noticeable gingival bulge was seen in anterior region of maxillary arch (Figure 2) (Table 2). A high smile line (gummy smile) was developed that shows complete the crown embedded in an excessive amount of gingiva.
Table 2: Cephalometric pre-treatment and post-treatment values.|
Measurement |
Normal value |
Pre-treatment |
Post-treatment |
|
Skeltal |
|||
|
SNA |
82 |
83 |
82.3 |
|
SNB |
79 |
76 |
76.5 |
|
ANB |
2 |
6 |
5.8 |
|
FMA |
23 |
32.3 |
32.5 |
|
Z-Angle |
60 |
56.5 |
70 |
|
Dental |
|||
|
Overbite (mm) |
1.8 |
3.5 |
2 |
|
Overjet (mm) |
3.5 |
3 |
2.5 |
|
FMIA |
59.8 |
59.7 |
51 |
|
1-FH |
116 |
114.5 |
111.8 |
|
Inter-Incisal |
123.8 |
125.1 |
119.4 |
|
Soft-tissue |
|||
|
Upper lip-E line |
-0.9 |
0 |
-o.5 |
|
Lower lip-E line |
0.6 |
0.5 |
0.5 |
After the occlusion settling, an exaggerated high smile line was developed due to the intrusion of anterior maxillary segment, hence, we required both crown lengthening and cortical shaving to achieve good smile and reduce gingival display. Thus, we planned for plastic periodontal therapy a new approach where in both gingivectomy and a full-thickness periodontal flap combined with osteotomy was performed as described by Cairo F, et al. [10] (Figure 3).
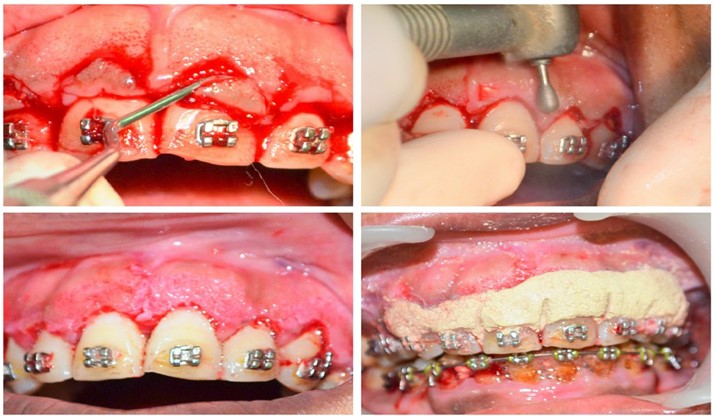 Figure 3: Plastic periodontal surgery.
Figure 3: Plastic periodontal surgery.
A total of 27-month time duration was taken to complete the VME case to its normal physiological state. After the periodontal surgery case left under observation for two months. After the confirmation of surgical wound heal by periodontist, and clinical examination of occlusion settling case was set to debond after placing permanent lingual retainers (Table 2) (Figure 4 and Figure 5).
 Figure 4: After debonding.
Figure 4: After debonding.
 Figure 5: Two years follow up.
Figure 5: Two years follow up.
Treatment of Gummy Smiles (GS) is more challenging to meet the expectations of patients seeking cosmetic treatments [8]. Both surgical and non-surgical methods are generally available for managing GS. Non-surgical includes Botulinum toxin type A injections as well as orthodontics, whereas surgical includes orthodontic treatment with orthognathic surgery [9].
Today, the wide range of mini screws has made it possible to avoid Lefort surgery and treat a gummy smile with minor gingival surgeries like clinical crown lengthening, gingivectomy, or positioning of an apical flap with or without bone resection [1-9].
The contemporary treatment for VME is orthodontic with orthognathic surgery. In this surgery maxilla is impacted to reduce the gingival exposure on smile, long face and restore aesthetic facial profile. The most accepted and followed treatment for VME is Le Fort I osteotomy of maxilla. The potential limitation of Le Fort I osteotomy is that as it impacts maxilla it reduces the bone between the nasal floor and the maxillary teeth resulting in flaring nose, surgical trauma, and associated inflammatory problems of bone plates [10].
In our case, the subject was skeletal class II malocclusion with long and broad nose appearance with GS, long clinical crown lengths, and most important is that patient rejected orthognathic surgery hence we thought of impacting maxilla using mini screws. We were able to impact maxilla to patient satisfaction but also it created gingival hyperplasia resulting in short clinical crowns, gingival bulging in between the upper central incisors. The total outcome of orthodontic treatment with mini screw was exaggerated GS.
The exaggerated GS is a multifactorial which is resulted from patient’s poor oral hygiene and habits of betel nut chewing, and relative intrusion also. Hence, we opted for minor and new periodontal surgery, i.e., plastic periodontal surgery. The outcome of periodontal surgery was most accepted by subject, even after two years of follow up the results don’t show any gross relapse.
Through this treatment procedure we successfully avoided Le Fort I osteotomy along with its potential disadvantages. The nose bridge was not altered, and it flares in Le Fort I osteotomy. Minimal trauma to patient. Results are more acceptable.
Case selection the subject age 35 years, poor oral hygiene, tobacco, and betel nut chewer. Secondly, mini screw used, whereas currently available infra-zygomatic bone screw would have avoided plastic periodontal surgery.
To improve smile aesthetics, in gummy smile cases, mini screws are a feasible option for skeletal class II malocclusion. However, the potential side effect of the mini screw is that it develops gingival hyperplasia, but the most advantageous part of our treatment plan is that it bypasses major surgery and its associated demerits. Only plastic gingival therapy helps overcome excessive gum disorders.
In the present case, we have achieved pleasant permanent facial aesthetics with mini screws in skeletal class II malocclusion after converting into class I. Still, this case report warns readers that the outcome of the case depends on proper case selection, the experience of the supervisor, and clinicians.
The authors have no conflicts of interest to report.
No

