 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Lina May Osit*, Joseph Joven Gammad, Olivia C. Flores
University of the East Ramon Magsaysay Memorial Medical Center, Inc.Quezon City, Manila.
Correspondence to: Lina May Osit, University of the East Ramon Magsaysay Memorial Medical Center, Inc.Quezon City, Manila.
Received date: September 18; 2021; Accepted date: October 3; 2021; Published date: October 10, 2021
Citation: Osit LM, Gammad JJ, Flores OC (2021) The Efficacy of Ultrasound-Guided Bilateral Transversus Abdominal Plane (TAP) Block in Decreasing the Pain After
Laparoscopic Cholecystectomy : A Randomized Clinical Trial. J Med Res Surg 2(5): pp. 1-6. doi: 10.52916/jmrs214058
Copyright: ©2021 Osit LM, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License; which permits unrestricted use; distribution and reproduction in any medium; provided the original author and source are credited.
Introduction: Pain after laparoscopic cholecystectomy is complex in nature and several methods are performed to control it. Transversus Abdominis Plane (TAP) block has been used for postoperative pain for some abdominal surgeries. This study was designed to determine the analgesic efficacy of bilateral TAP block for patients undergoing Laparoscopic Cholecystectomy.
Methods: Forty-two patients were randomized into 2 groups. Group 1 received TAP block using bupivacaine 0.25% (n=21), and group 2 received TAP block using saline. Before extubation, blocks were performed bilaterally. Tramadol IV was given for breakthrough pain for the first 24 hours. Pain scores using the visual analog scale (VAS) at 0, 1, 2, 4 ,8 ,12, 24 hour-intervals, number of patient demand for Tramadol and patient satisfaction were collected.
Results: Patients in the control group have higher VAS scores both during rest and on movement. However, pain was significantly reduced only on the 2nd hour at rest and on the 1st to 4th hours on movement among patients who received Bupivacaine 0.25% on TAP block. Furthermore, there was no significant difference in the requirement for rescue analgesics (p=0.1160) and the satisfaction rate (p=0.2849) between the two groups.
Conclusion: TAP block is safe and improved postoperative analgesia in patients receiving laparoscopic cholecystectomy. But its additional analgesic effect in the presence of a dynamic multimodal pain-control regimen is probably rather small and need further investigation in laparoscopic cholecystectomy.
Keywords: Laparoscopic cholecystectomy, Transversus Abdominis Plane (TAP), Surgery, Pain, Treatment.
Laparoscopic cholecystectomy is now the standard surgery for symptomatic gall stone disease and has improved patient satisfaction in terms of early post-operative pain control, need for post-operative analgesia, hospital stay, total cost and return to normal activity when compared to open cholecystectomy [1].
Post-operative pain due to laparoscopic cholecystectomy is less intense and lasts a shorter duration compared to an open surgery which leads to early discharge and return to their normal activities [2]. Pain reaches its peak on the the first few hours after the surgery but decreases on the 2nd or 3rd postoperative day [3]. Its pain is complex in nature and is a conglomeration of three components: Visceral (deep intrabdominal pain), incisional pain (somatic) and referred shoulder tip pain (referred to visceral) [4]. Local effects of pneumoperitoneum causes peritoneal and diaphragmatic stretching, acidosis and ischemia and its systemic effects causes sympathetic nervous system excitation due to hypercarbia with increase local tissue inflammatory response [5,6]. Considering that acute pain post laparoscopic cholecystectomy is complex and has high interindividual variation suggsts [4,7] that effective postoperative analgesia should be multimodal [8] with the least potential side effects. Poor pain control after laparoscopic cholecystectomy may predict the development of chronic pain [9]. Moreover, inadequate pain relief may result in increased morbidity and mortality [10]. Opioid-sparing, balanced analgesia provides better pain control and faster recovery compared with opioids or local anesthetics alone [9].
The Transabdominis Plane Block (TAP) block has been known to be a good analgesic technique for 24 hours11 after abdominal procedures. It could address the complexity of pain of laparoscopic cholecystectomy and decrease the use of opioids and its unwanted side effects as was first described by Rafi in 200112. He illustrated it as a refined abdominal field block, with a targeted single shot local anesthetic delivery into the TAP, a site traversed by relevant nerve branches.
The deposition of local anesthesia within the plane of internal oblique and transversus abdominis muscles can produce sensory block over the anterior abdominal wall from T7- L1.12 This block may be performed in a blind approach or by ultrasonographic guidance.
To date, more than 20 original studies have addressed this technique in laparoscopic cholecystectomy however there are still contradictory results and controversies in reduction of pain scores which is said to be minimally relevant in this population. The objective of this study was to determine the analgesic efficacy of bilateral TAP block for patients undergoing Laparoscopic Cholecystectomy. It aimed to compare postoperative pain scores of patienst who received TAP block versus those who received the placebo using Visual Analog Scale at rest and with movement at the 1st, 2nd , 4th, 8th, 12th, and 24th hour of postoperative period. This study also intended to compare the rescue analgesic (Tramadol) demands of patients who received TAP block versus those who received the placebo. Furthermore, it also aimed to evaluate the over-all satisfaction of patients on pain management who received TAP block versus those who received the placebo using a 6-point Likert scale.
After approval by the local institutional ethical review board, written informed consent was obtained from all participants. Due to national scarcity of local anesthetic Bupivacaine, we stopped patient’s enrollment on the middle of our study. In total, 46 patients were prospectively enrolled with the American Society of Anesthesiologists physical status class I or II. Patients with a history of opioid analgesic abuse, hypersensitivity to opioids or any NSAIDS, chronic pain, or significant systemic disease were excluded. Moreover, patient with coagulopathy, allergies to local anesthetics or local skin infection at the needle puncture site were excluded as well. Laparoscopic cholecystectomy was performed among these patients between November 2017 and August 2018 at University of the East Ramon Magsaysay Memorial Medical Center Hospital, a tertiary care center. A total of 4 patients were excluded in the study: 2 patients had a shift of surgical technique to open cholecystectomy intraoperatively and 2 had mild hypersensitivity reaction to latex and Ketorolac which manifest as erythematous wheal detected intraoperatively prior to TAP block.
The Visual Analog Scale (VAS) scores were explained to all patients, who indicated pain levels by placing a mark in a straight line of 100 mm in length, with one end defined as “no pain” and the other as the “worst imaginable pain.” The distance between the end labeled “no pain” and the mark placed by the patient was measured in millimeter, and pain scores were recorded. Patients were randomized with sealed envelopes, to undergo TAP block (n=21) or to receive a placebo (n=21). Patients, the anesthesiologist, and the staff providing postoperative care and assessing postoperative pain were blinded to group assignment. All patients received a standardized general anesthetic. Standard monitoring, including electrocardiogram, non-invasive blood pressure, oxygen saturation through pulse oximetry, and endtidal carbon dioxide monitoring were used throughout, and patients were placed in the supine position.
Following the induction of general anesthesia, all patients received Dexamethasone 5mg IV and Paracetamol of 1 gm. Once the gallbladder is removed, both groups were given Ketorolac 30mg IV and Tramadol 50 mg IV. Neuromuscular blockade was reversed at the end of surgery.
After the surgery, the patient received his/her intervention according to group assignment. Bilateral TAP block was performed on the experimental group under ultrasonographic guidance with a transportable ultrasound device and a linear 6-13 MHz ultrasound transducer. The external oblique, internal oblique, and transversus abdominis muscles were visualized at the level of the anterior axillary line between the 12th rib and the iliac crest where the ultrasound probe was placed. Sterile preparation of the insertion site was done, and a needle was inserted in-plane and anterior to the probe, and was advanced in a posterolateral direction. The tip of the needle was placed in the space between the internal oblique and transversus abdominis muscles under direct ultrasound guidance, and a total of 20 mL of Bupivacaine 0.25% was injected incrementally after careful aspiration to ensure no vascular injury has occurred. The control group received 20 mL of 0.9% NaCl injected on the same plain of the experimental group. Blocks were performed by the anesthesiologist-in-charge who is blinded by the solution injected on the TAP.
Time of arrival at the Post Anesthesia Care Unit (PACU) was the time 0 for pain assessments. Pain at rest and upon movement was recorded for each patient using VAS (0-100mm) at time 0 and at 2, 4, 8, 12, and 24 hours after the surgery is completed. The interns-in charge of the patient were instructed on how to use VAS pain score and the 6-point Likert scale. All patients were placed on post-operative analgesic regimen which includes 2 doses of Tramadol 50mg IV, 3 doses of Paracetamol 600mg IV and Ketorolac 30mg IV to cover the analgesia for 24 hours then was shifted to oral analgesics for 7 days. Total Tramadol demands of 50mg IV every 6 hours were given for breakthrough pain and were recorded. On the 24th hour, patient was asked of their satisfaction level on the acute pain management using the 6-point Likert scale. The attending anesthesiologist and the intern who assessed the pain scores and satisfaction level were blinded to the group assignment.
The VAS scores at rest and upon movement, total Tramadol demands and Satisfaction level were recorded and compared among TAP and placebo group.
Data were analyzed using Stata version 13 software. Descriptive statistics entailed use of mean with standard deviation for quantitative variables and use of counts and proportions for qualitative variables.
To determine significant differences between experimental and control groups on quantitative continuous variables (age, duration of surgery, VAS scores), independent t-test was used. Alternatively, Wilcoxon Mann-Whitney test was used for ordinally-scaled or skewed numerical variables. For determining significant differences on qualitative variables between groups (gender, ASA classification, demands for rescue analgesia), chi square test was utilized with Fishers exact test when applicable. A p-value <0.05 was used as cut-off for significance.
The study had 46 enrolled participants but had 2 drop-out in both groups, which yielded a 21 participants in each group for statistical analysis. A sensitivity for assessing if the drop-out rate was significantly done.
In Table 1, baseline comparability studies showed no significant differences between the TAP block group and the control group in their demographic (age and gender distribution) and clinical characteristic (ASA classification and duration of surgery) (p values ≥0.05) (Table 1).
| TAP Block | Control | ||
| Characteristics | Group | Group | p-value |
| n=21 | n=21 | ||
| No. (%) | No.(%) | ||
| Gender | 0.2165* | ||
| Male | 9 (42.9) | 13 (61.9) | |
| Female | 12 (57.1) | 8 (38.1) | |
| Age in years (mean, sd) | 40.4, 11.1 | 35.8, 10.8 | 0.1747 |
| ASA classification | 0.4878ǂ | ||
| 1 | 0 | 1 (4.8) | |
| 2 | 21 (100.0) | 19 (90.5) | |
| 3 | 0 | 1 (4.8) | |
| Duration of surgery in minutes (mean, sd) | 99.3, 36.4 | 107.3, 35.2 | 0.4736 |
| *Chi square test; Independent t-test; ǂFishers exact test | |||
Table 2 and Figure 1 illustrate the differences in postoperative VAS scores at rest between groups. Generally, pain was noted to decrease throughout the 24 hours following the surgery. There was a decreasing trend in VAS scores at rest for both groups, with a noticeable drop observed on the 8th hour by as much as 50-56%. Scores were noted to be higher in the control group from the first to the 8th hour, almost equal by the 12th hour and slightly higher in favor of the TAP block group by the 24th hour The differences, 4though, did not reach statistical significance (p>0.05). The mean VAS score of patients in the control group on the 2nd hour-interval was significantly higher (p<0.0222).
| Postoperative Period | TAP Block Group | Control Group | p-value |
| n=21 | n=21 | ||
| VAS mean, sd | VAS mean, sd | ||
| 1st hour | 44.4, 28.4 | 58.8, 23.6 | 0.0817 |
| 2nd hour | 44.3, 25.3 | 62.2, 23.6 | 0.0222 |
| 4th hour | 41.1, 28.9 | 56.1, 28.8 | 0.0996 |
| 8th hour | 20.3, 14.5 | 24.6, 17.0 | 0.3902 |
| 12th hour | 19.5, 14.3 | 19.9, 14.4 | 0.9319 |
| 24th hour | 9.8, 16.0 | 8.4, 11.2 | 0.7559 |
| Independent t-test | |||
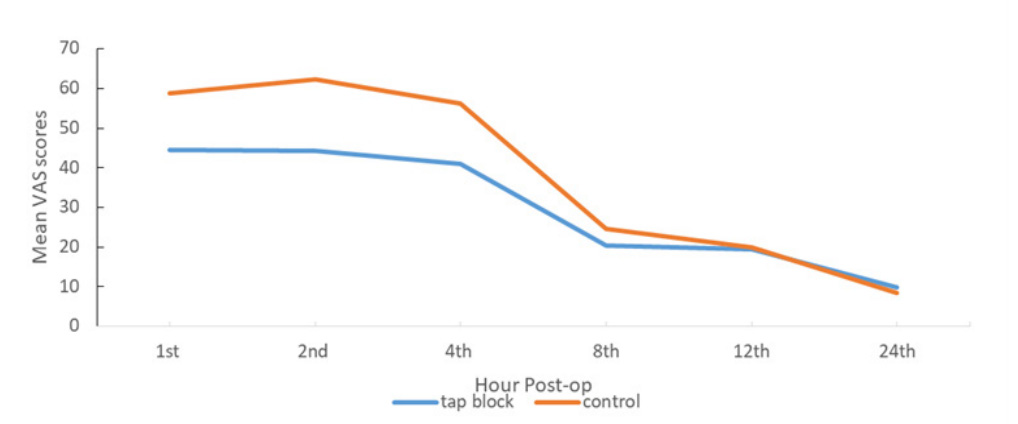 Figure 1: Mean VAS scores at rest throughout 24 hours post-op
Figure 1: Mean VAS scores at rest throughout 24 hours post-opLikewise, table 3 and figure 2 demonstrate a decreasing trend in VAS scores on movement for both groups which was more pronounced on the 8th hour by as much as 40-46%. Scores were noted to be higher in the control group than the TAP block group and were significantly different from each other on the 1st to the 4th hour postop (p<0.05). The succeeding time periods (8th to 24th hour), though, no longer showed significant differences in scores (p≥0.05).
| Postoperative Period | Treatment Group n=21 VAS mean, sd |
Control Group n=21 VAS mean, sd |
p-value |
| 1st hour | 43.7, 23.7 | 60.0, 23.7 | 0.0486 |
| 2st hour | 44.1, 24.6 | 64.2, 22.1 | 0.0081 |
| 4st hour | 43.2, 26.2 | 59.9, 26.0 | 0.0444 |
| 8st hour | 25.7, 12.9 | 32.1, 22.6 | 0.2677 |
| 12st hour | 26.4, 15.2 | 32.3, 23.9 | 0.3444 |
| 24st hour | 19.3, 18.2 | 19.9, 17.9 | 0.9205 |
| Independent t-test | |||
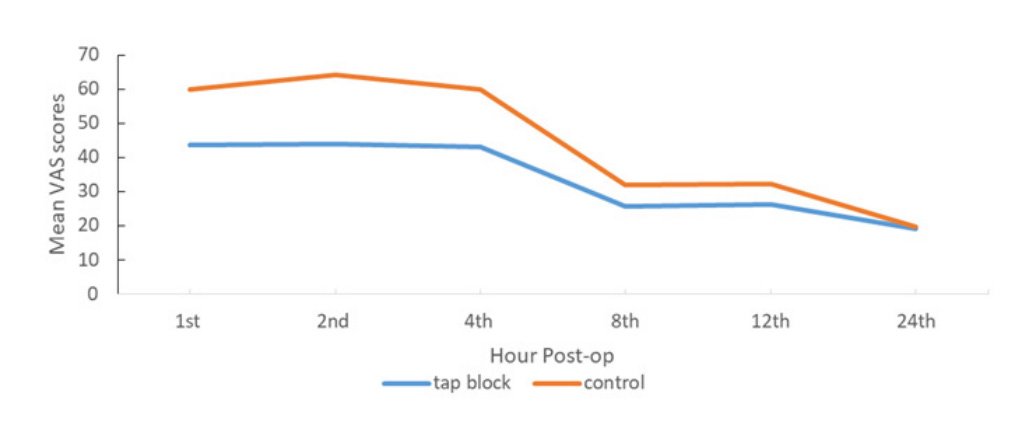 Figure 2: Mean VAS scores on movement throughout 24 hours post-op.
Figure 2: Mean VAS scores on movement throughout 24 hours post-op.Table 4 shows that Seventy-one percent in the control group demanded rescue analgesics at least once. Conversely, 52% in the TAP block group did not require rescue analgesics. However, there was no significant difference in the requirement for rescue analgesics between the two groups (p=0.1160).
| Demands for rescue analgesia | Treatment Group n=21 No. (%) |
Control Group n=21 No. (%) |
p-value |
| 0 | 11 (52.4) | 6 (28.6) | 0.1160 |
| ≥ 1 | 10 (47.6) | 15 (71.4) | |
| *Chi square tests | |||
Table 5 presents the differences in satisfaction ratings. The median satisfaction rating was no different between the two groups (p=0.2849). Both groups were equally “mostly satisfied” with the relief from pain after 24 hours post-op.
| Median Satisfaction Rating | Treatment Group n=21 |
Control Group n=21 |
p-value |
| Median (Interquartile range) | 5 (5 - 6) | 5 (4–6) | 0.2849 |
| §Wilcoxon Mann-Whitney test | |||
The sensitivity analysis for assessing if the drop-out rate was significant showed that the best-case and worse-case scenario assumptions showed the same results. The conclusion did not change with the assumptions made.
The present study compared the efficacy of bilateral TAP block with 0.25% bupivacaine vs saline as adjunct to control postoperative pain in patients who underwent laparoscopic cholecystectomy.
Previous controlled trials by El-Dawlatly et al, Ra YS et al, Petersen PL et al have demonstrated analgesic efficacy of TAP blockade after laparoscopic cholecystectomy [17-19]. Moreover, meta-analysis studies [20-21] on the analgesic efficacy of TAP block demonstrated a reduction of postoperative pain scores, significant opioid sparing, and reduced opioid- associated side effects compared with those receiving conventional treatment alone. This gives credence to our findings of lower VAS scores at all time intervals in those patients given TAP block with local anesthetic compared to the group who received saline solution. Both groups showed decreasing trend in VAS pain scores through the six measured times with a notable drop on the 8th hour post surgery. Additionally, the control group’s VAS scores were higher both during at rest and on movement. The VAS scores at rest on the 2nd hour and VAS scores on movement at the 1st to 4th hour-time intervals were significantly reduced in the experimental group. A similar finding by Peterson, et al [19] reported significantly reduced VAS pain score while coughing in patients who received TAP block versus the placebo group while no significant difference between groups on VAS scores at rest. This may be clinically relevant especially in centers where they do laparoscopic cholecystectomy as a day-surgery procedure in which inadequate pain control is one of the most common reason for delayed discharge and unexpected admission to the hospital [13] And maximum pain intensity in our study was recorded on the 2nd hour post surgery. This could be attributed to the recovery from residual effects of anesthesia and opioids used during surgery.
El Dawlatly et al [17], showed a significant reduction of perioperative administration of sulfentanyl and 24-hour morphine demands in the patients who received TAP block after laparoscopic cholecystectomy. Ra YS et al [18] also demonstrated reduced use of ketorolac and fentanyl after TAP block and significantly low pain scores for 24 hours. Despite the significantly lower pain scores during movement on the first 4 hours in our study, Tramadol demand is not significantly lower in the TAP block group. Most demands of tramadol was at 0 to 2 hours which coincide with the study of Peterson, et al [19] who reported reduction of morphine consumption at 0 to 2 hours postoperatively; however, the actual reduction in morphine was not significant.
The American Pain Society in Quality Assurance Standards for Relief of Acute and Cancer-related pain stated clearly that patient satisfaction with pain management must be examined and recorded in clinical practice [22]. Patient satisfaction has been claimed by many authors as a degree to which patient expectations are fulfilled [14-16]. Despite the moderate pain levels reported by patients in both groups, all claimed to be mostly satisfied which imply that their expectations on pain management were met. Cultural and religion influence might have played a great role in their expectations on their pain experience, since Filipinos are known to be stoic in the face of pain and for Catholic Filipinos suffering is an opportunity to show their virtue [23].
Our results although promising had limitations. First, our sample size was small; secondly, despite US-guidance of the block, sensory block can not be ascertained; thirdly, we performed the lateral approach of the TAP block at the level of the umbilicus which could have limited the sensory coverage above it where the upper port holes or incisions were situated [24]. Subcostal TAP block, a variation of TAP block, would have been more appropriate to produce reliable supraumbilical analgesia [25]. And TAP block was limited to somatic anesthesia to abdominal wall which failed to address the visceral analgesia of the abdominal wall. Lastly, the TAP block was done postincision, in contrast to previous studies where TAP block was done prior to incision. Pre-incisional TAP block appeared to reduce the severity of acute pain and analgesic requirements in one study [26].
To address the abovementioned limitations, we recommend further studies. Moreover, pharmacodynamic characteristics of TAP block, sensory blocking range of local anesthetics, and the analgesic mechanisms of the TAP block would be important considerations in future investigations.
TAP blocks is an acceptable and safe choice for postoperative analgesia. It improved postoperative analgesia in patients receiving laparoscopic cholecystectomy, especially during movement on the acute postoperative hours. Its analgesic effect in the presence of a dynamic multimodal pain-control regimen is probably rather small. Further investigation is needed to fully explore the benefits of TAP block as an the sole pain control management or at the least an adjunct to a parenteral or oral multimodal pain control regimen in laparoscopic cholecystectomy.
1. Starasberg SM (2011) Clinical Practice Acute, Calculus Cholecystitis. New England Journal 358(26): pp. 2804.
2. Prabhu R, Singh DR, Krishnaveni N (2017) A Comparative Study of Postoperative Analgesia Provided by Ultrasound-Guided Transversus Abdominis Plane Block Using Two Concentrations of Bupivacaine in Patients Undergoing Inguinal Hernia Repair. Anesth Essays RES 11(4): pp. 934-939.
3. Inan A, Sen M, Dener C (2004) Local Anesthesia Use For Laparoscopic Cholecystectomy. World J Surg 28(8): pp. 741-744.
4. Bisgaard T, Klarskov B, Rosenberg J, et al. (2001) Characteristics And Prediction Of Early Pain After Laparoscopic Cholecystectomy. Pain 90(3): pp. 261-269.
5. Joris J, Thiry E, Paris P, et al. (1995) Pain After Laparoscopic Cholecystectomy: Characteristics And Effect Of Intraperitoneal Bupivacaine. Anesth Analg 81(2): pp. 379-384.
6. Mouton WG, Bessell JR, Otten KT, et al. (1999) Pain After Laparoscopy. Surg Endosc 13(5): pp. 445-448.
7. Wills VL, Hunt DR (2000) Pain After Laparoscopic Cholecystectomy. Br J Surg 87(3): pp. 273-284.
8. Bisgaard T (2006) Analgesic Treatment after Laparoscopic Cholecystectomy: A Critical Assessment of the Evidence. Anesthesiology 104(4): pp. 835-846.
9. Katz J, Jackson M, Kavanagh BP, et al. (1996) Acute Pain After Thoracic Surgery Predicts Long-Term Post-Thoracotomy Pain. Clin J Pain 12(1): pp. 50-55.
10. Bisgaard T, Rosenberg J, Kehlet H (2005) From Acute To Chronic Pain After Laparoscopic Cholecystectomy: A Prospective Follow-Up Analysis. Scand J Gastroenterol 40(11): pp. 1358- 1364.
11. Caius M, Ciobano L, Hadade A. The Efficacy of Oblique Subcostal Transversus Abdominis Plane Block In Laparoscopic Cholecystectomy. Rom J Anaesth Intensive Care 23(1): pp. 12-18.
12. Young M, Gorlin A, Modest V, et al. (2012) Clinical Implications Of The Transversus Abdominis Plane Block In Adults. Anesthesiol Res Pract 2012: pp. 731645.
13. Tenconi SM, Boni L, Colombo EM et al,. Laparoscopic cholecystectomy as day-surgery procedure: current indications and patients’ selection. Int J Surg. 2008;6 Suppl 1:S86-8.
14. Abramowitz S, Cote A, Berry E (1987) Analyzing patient satisfaction: A Multianalytic Approach. Quality Review Bulletin 13(4): pp. 122-130.
15. Greeneich D (1993) The Link Between New And Return Business And Quality Of Care: Patient Satisfaction. Adv in Nurs Sci 16(1): pp. 62-67.
16. Williams B (1994) Patient satisfaction: A valid concept?. Soc Sci Med 38(4): pp. 509-516
17. El-Dawlatly AA, Turkistani A, Kettner SC, et al. (2009) Ultrasound-guided trans- versus abdominis plane block: description of a new technique and comparison with conventional systemic analgesia during laparoscopic cholecystectomy. Br J Anaesth 102(6): pp. 763-767.
18. Ra YS, Kim CH, Lee GY, et al. (2010) The analgesic effect of the ultrasound-guided transverse abdominis plane block after laparoscopic cholecystectomy. Korean J Anesthesiol 58(4): pp. 362-328.
19. Petersen PL, Stjernholm P, Kristiansen V, et al. (2012) The Beneficial Effect of Transversus Abdominis Plane Block After Laparoscopic Cholecystectomy in Day-Case Surgery: A Randomized Clinical Trial. Anesth Analg115(3): pp. 527-533.
20. Siddiqui MR, Sajid MS, Uncles DR, et al. (2011) A metaanalysis on the clinical effectiveness of transversus abdominis plane block. J Clin Anaesth 23(1): pp. 7e14.
21. Ke P, Fu-hai J, Hua-yue L, et al. (2016) Ultrasound-Guided Transversus Abdominis Plane Block for Analgesia in Laparoscopic Cholecystectomy: A Systematic Review and Meta-Analysis. Med Princ Pract 25(3): pp. 237–246.
22. Bond MR, Charlton GE, Wolff C, et al. (1992) Proceeding of the Sixth World Congress on Pain. New York: Elsevier; American Pain Society. Quality assurance standards for relief of acute pain and cancer pain: pp. 185–189.
23. Galanti G (2000) Filipino Attitude Toward Pain Medication. West J Med 173(4): pp. 278-279.
24. Tran TM, Ivanusic JJ, Hebbard P, et al. (2009) Determination Of Spread Of Injectate After Ultrasound-Guided Transversus Abdominis Plane Block: A Cadaveric Study. Br J Anaesth 102(1): pp. 123-127.
25. Tolchard S, Davies R, Matindale S (2012) Efficacy Of The Subcostal Transversus Abdominis Plane Block In Laparoscopic Cholecystectomy: Comparison With Conventional Port-Site Infiltration. J Anaesthesiol Clin Pharmacol 28(3): pp. 339-43.
26. Amr Y, Amin S (2011) Comparative study between effect of pre- versus post-incisional transversus abdominis plane block on acute and chronic post-abdominal hysterectomy pain. Anesth Essays Res 5(1): pp. 77–82.
PDF Google Scholar 10.52916/jmrs214058
