 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Zekeriya Kul*
Department of Plastic and Reconstructive Surgery, Uskudar University, Istanbul, Turkey.
Correspondence to: Zekeriya Kul, Department of Plastic and Reconstructive Surgery, Uskudar University, Istanbul, Turkey.
Received date: January 07, 2025; Accepted date: January 25, 2025; Published date: January 31, 2025
Citation: Kul Z. The Determining of the New IMF and Incision Location in Breast Augmentation Using Ergonomix Model Implants. J Med Res Surg. 2025;6(1):4-8. doi: 10.52916/jmrs254157
Copyright: ©2025 Kul Z. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
This study presents a geometric formula to optimize the location of the Inframammary Fold (IMF) and incision site in breast augmentation with Ergonomix model implants. Traditional volumetric planning can lead to complications, including poor implant positioning and visible scars. By applying a semicircular arc length formula, 30 patients undergoing primary breast augmentation were evaluated between 2018 and 2021. Results showed accurate IMF and incision placement for 29 patients, achieving the desired 45% upper pole and 55% lower pole ratio. The proposed method simplifies surgical planning, improves outcomes, and enhances long-term stability, offering a practical, effective alternative to subjective techniques.
Inframammary Fold (IMF), Breast, Augmentation surgery, Ergonomix implants.
Breast augmentation surgery is the most common surgery among aesthetic surgical procedures [1]. However, the complication rate is significantly high which is related to wrong preoperative planning or surgical technique [2]. Despite the correct implant selection, the incorrect determination of the incision and the new Inframamarian Fold (IMF) location to be created, and the preparation of the pocket incompatible with the implant, will lead to the visibility of the incision scar and an undesirable breast shape.
Both artists and plastic surgeons have argued for many years about how the ideal breast shape should be, and an accepted definition has emerged today [3]. According to this definition; the upper pole of the breast must be flat or light slope, the lower pole must be full and round, the upper pol / lower pol ratio; must be 45/55, and nipple angulation should be 15-20 degrees in the upward direction (Figure 1).
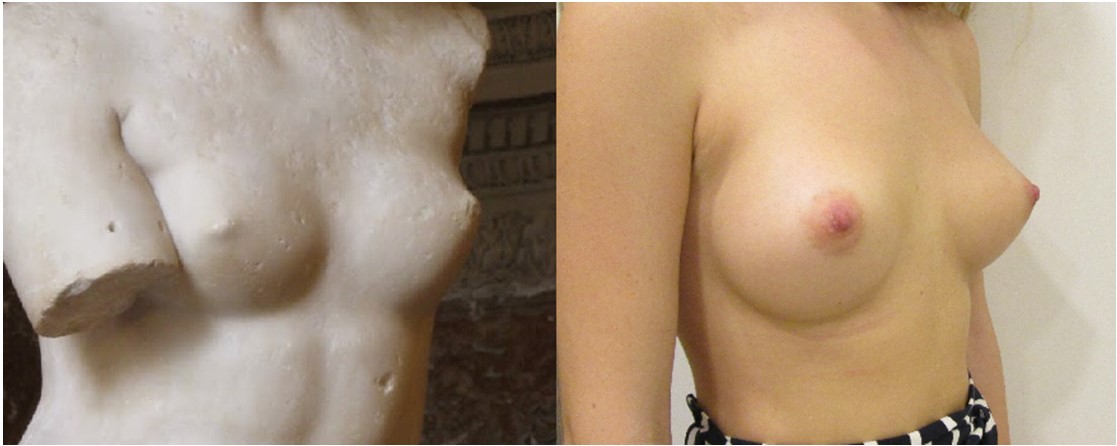 Figure 1: A): As in Milo's Venus sculpture; B): The ideal breast shape has a flat upper pole, a rounded lower pole, and a nipple angled upward.
Figure 1: A): As in Milo's Venus sculpture; B): The ideal breast shape has a flat upper pole, a rounded lower pole, and a nipple angled upward.The ideal implant to obtain such a breast anatomy is the anatomically shaped implant. However, the difficulties of planning anatomical implants, rotation or lateral displacement, and risks such as malposition caused the distance approach of plastic surgeons to anatomical implants. In a prospective study, the malposition rate of anatomical implants within 10 years was found to be 4.7% after primary breast augmentation surgery and 9.1% after revision surgery [4]. This situation led plastic surgeons and implant manufacturers to research and Ergonomix implants were born as a result of this search. Ergonomix model implants are fully filled and because of the rheological properties of the gel in their contents, their shapes change to anatomical when standing and round when lying down (Figure 2).
 Figure 2: Ergonomix model implants are round implants that mold to the natural shape of the breast to mimic the appearance of teardrop-shaped implants.
Figure 2: Ergonomix model implants are round implants that mold to the natural shape of the breast to mimic the appearance of teardrop-shaped implants.Incorrect planning of the new IMF and improper placement of the incision will cause migration of the implant inferiorly (Bottom-out deformity) or stay most part at the upper pole (Figure 3).
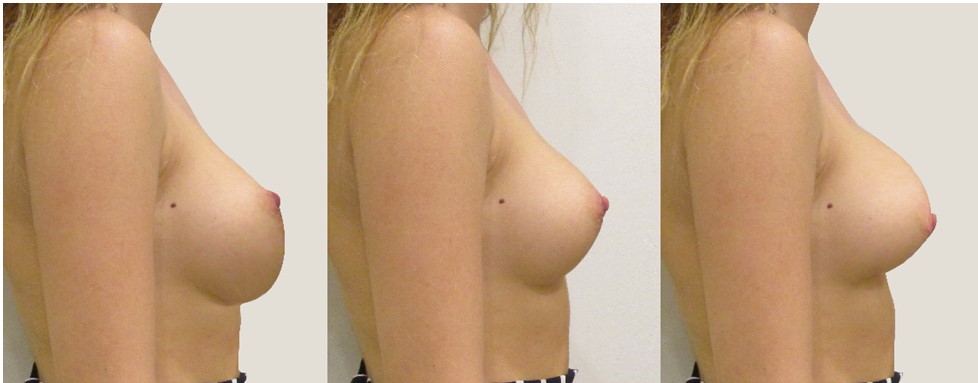 Figure 3: A): Bottom-out deformity occurs as a result of the downward migration of the implant; B): Ideal breast shape; C): The big part of the implant remaining in the upper pole causes a short lower arch.
Figure 3: A): Bottom-out deformity occurs as a result of the downward migration of the implant; B): Ideal breast shape; C): The big part of the implant remaining in the upper pole causes a short lower arch.Although the use of bi-dimensional methods instead of volumetric methods for implant selection and preoperative planning has reduced the complication rate, a simple and mathematical formulation has always been needed to ensure that planning is as objective as possible. Therefore, we thought that the geometric formula used to calculate the arc length of semicircular structures could be used to determine the new IMF location and incision location during preoperative planning of breast augmentation. So, we used this geometric formula to determine the new IMF and incision locations of 30 patients who had primary breast augmentation surgery with an inframamarian approach between 2018-2021, as an alternative to the methods used for this day (Figure 4). This geometric formula uses the radius, Pi value, and the angle of this semicircular structure to calculate the arc length. Since the vertical projection of the nipple corresponds to the center of the Ergonomix implant, which takes a rounded shape in the lying position, the radius is equal to the sum of implant projection and tissue thickness according to the geometric rule we have adapted. (Figure 5).
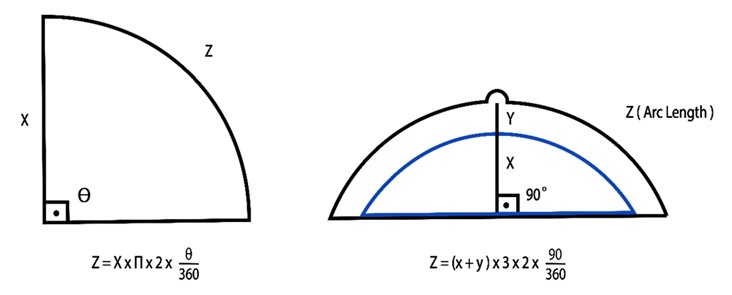 Figure 4: The geometric formula to calculate the arch length of a semicircular structure and adaptation to breast augmentation planning.
Figure 4: The geometric formula to calculate the arch length of a semicircular structure and adaptation to breast augmentation planning. Figure 5: To find the implant diameter, we subtract the lateral+medial breast tissue thickness from the desired postoperative breast base diameter.
Figure 5: To find the implant diameter, we subtract the lateral+medial breast tissue thickness from the desired postoperative breast base diameter.Using the formula of calculating the sum of these two values and the length of the semicircular arc, we were able to determine the new IMF and incision location in the lying position, under maximum traction.
As a prospective, 30 patients who had primary breast augmentation surgery with an inframammary approach were included in the study. We used the base diameter of the implant as the primary variable when selecting implants. We found the implant base diameter by subtracting the lateral+medial breast tissue thickness from the desired postoperative breast base diameter, which we measured between the medial breast border and the posterior axillary line. (Figure 6).
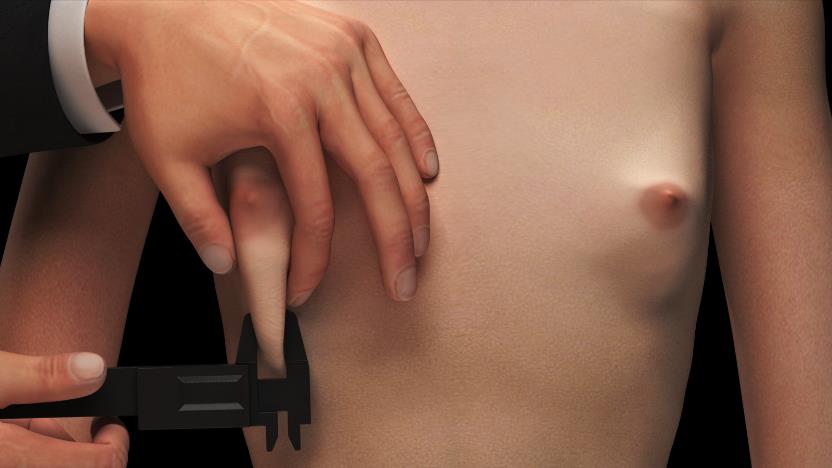 Figure 6: We perform a pinch test on the lower pole to determine the average tissue thickness of the breast.
Figure 6: We perform a pinch test on the lower pole to determine the average tissue thickness of the breast.The second variable parameter for implant selection is the projection. We determined the projection based on tissue elasticity and patient expectations.We used an external sizer system and 3D imaging technology (Axis Three, AX3 Technologies, Miami, FA, USA) to determine patient expectations (Figure 7).
 Figure 7: Understanding the patient expectations is very important during the selection of the implant, therefore we use an external sizer system and 3D scanning.
Figure 7: Understanding the patient expectations is very important during the selection of the implant, therefore we use an external sizer system and 3D scanning.Using the data we obtained, the formula used to measure the arch lengths of semicircular structures was used to determine the new IMF and incision location. Preoperative and postoperative images of the patients were taken from the front-oblique and lateral angles (with a Canon EOS 600D digital camera) at 3-6-12-18-24 months (Figure 8-9) and checked the position of the new IMF level and incision scar.
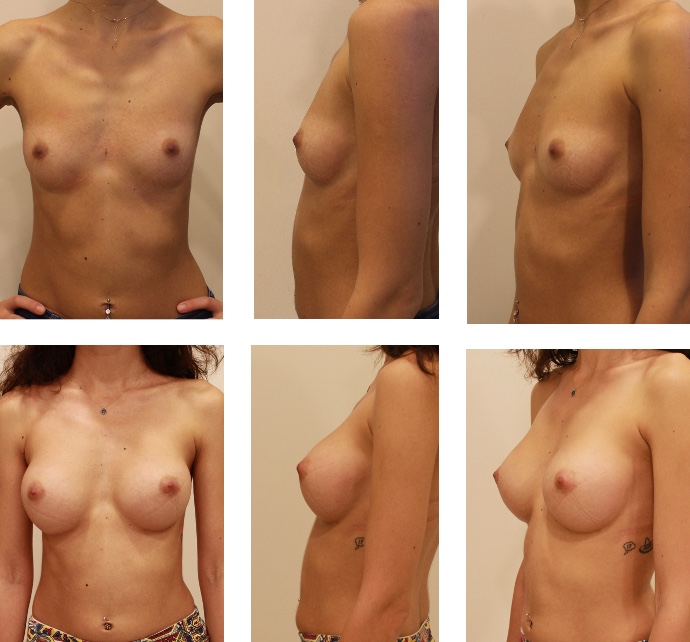 Figure 8: Pre-operative (top) and post-operative (bottom) 2nd years photos of a patient (335 cc ERSF , Dual Plan 2).
Figure 8: Pre-operative (top) and post-operative (bottom) 2nd years photos of a patient (335 cc ERSF , Dual Plan 2).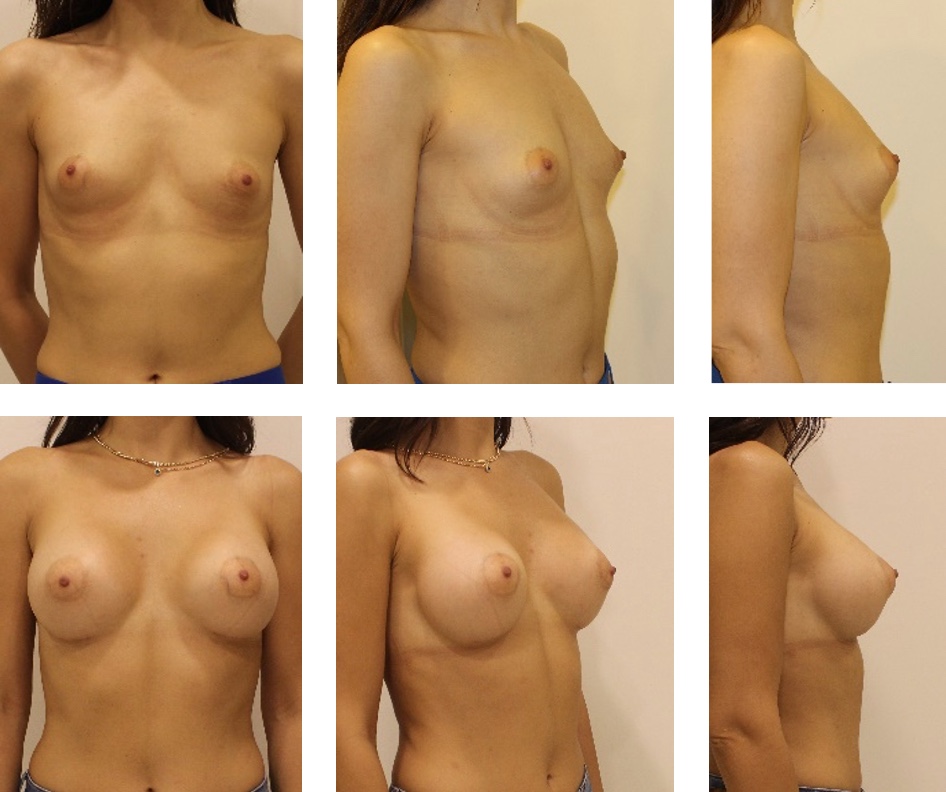 Figure 9: Pre-operative(top) and post-operative(bottom)2nd years photos of a patient(355 cc ERSF , Dual Plan 2).
Figure 9: Pre-operative(top) and post-operative(bottom)2nd years photos of a patient(355 cc ERSF , Dual Plan 2).An Example of Using the Arch Length Calculation Formula
For example, the projection length of anErgonomix model full projection(ERSF) implant with 315 cc, is 4.6 cm (X). If the patient has 2 cm of tissue thickness (Y), we calculate the Z value as 4.6+2:6.6. Then, we find the arch length of the postoperative lower pole as 9.9 cm using the geometric formula ((X+Y) * pie * 2 * 90/360.): 6.6 * 3 * 2 * 1/4: 9.9 cm. We apply maximum traction between the nipple and IMF and determine the new level of Inframamarian Fold (IMF) and incision location (Figure 10). Figure 10: The marking of the new IMF and incision line.
Figure 10: The marking of the new IMF and incision line.The surgery was performed according to the 14 rules described by technical Deva et al(5). Inframamarian incision was preferred for all patients. Dissection was performed with mono-polar cautery instead of blunt dissection. After careful bleeding control, the implant was washed with a 3-course antibiotic solution (Gentamycin, Cefazolin, Betadine), and was inserted with a funnel aid. The drain was not used. Before the incision line was closed, the Scarpa fascia was fixed to the thoracic fascia with a 3-point 2/0 vicryl.
30 patients were included in the study throughout 3 years (from January 2018 to December 2021). The patient's demographic and postoperative complications are summarised in Table 1.
In all patients, it was determined that upper pole fullness was decreased flat or light concavity was obtained with lateral and oblique photo images during the postoperative period and lower pol convexity was increased over time (Figure 11).
 Figure 11: A): Pre-operative; B): 3rd months; and C): 2ndyear post-operative result pictures of a patient for whom we used 335 cc ERSF.
Figure 11: A): Pre-operative; B): 3rd months; and C): 2ndyear post-operative result pictures of a patient for whom we used 335 cc ERSF.We found that the inframamarian incision has remained inside of the new IMF fold for 29 patients, and 1 cm displaced superiorly for the left breast of 1 patient.
The most important factor that determines the outcome after breast augmentation is the choice of the correct implant and the alignment of the implant with the physical properties of the breast and body. What is the ideal breast implant shape should be in that way? In the last scientific study in which the definition of the ideal breast was made and published by Dr. Malucci et al. [3] proportionally, the lower pole should have 55% and the upper pole should have 45%. Therefore we aim to achieve that the upper pol should have a flat or slightly concave appearance, while the lower pol should have a fuller and rounded appearance. So, to understand the patients' expectations correctly or to bring their expectations to a realistic point, 3D imaging systems or external sizers must be used.
Traditional volumetric planning methods for anatomical implants do not work and dimensional planning requires special methods that are difficult to apply, which has caused plastic surgeons to stay away from the use of anatomical implants. Especially in recent years, this situation has increased even more due to late complications(capsule contracture, late seroma, rotation)caused by the macrotexture surface and physical properties of anatomical implants.At this point, Ergonomix model implants started to be produced with round shapes but mimicked the shape of the anatomic implants. Due to the rheological properties of the gel in their contents and their mimicking of the anatomical implants, the use of dimensional planning methods is required during implant selection and surgical planning.
The prediction of the amount of expansion that will occur in the lower pole and ensuring that the new IMF remains at the planned level and that the incision scar remains within the new IMF is crucial to obtaining the ideal breast shape and proportions (45/55). Since Ergonomix implants have a round base and change to a round shape in the supine position, the geometric formula we applied to determine the new IMF and incision location both simplified the surgical planning and made the result long-lasting. Also, fixing the Scarpa fascia to the thoracic fascia firmly and securely is crucial, the new IMF location and the location of the incision scar do not change.
According to the results we obtained, the fact that the incision remained in the new IMF significantly in the majority of patients shows the effectiveness and importance of this fixation. Also, the majority of patients had a flattening or minimal concavity at the end of the first year and a plump at the lower pole at the end of the first year in addition, the projection of MPP, which corresponds to the lower boundary of the areola, causes angulation in the nipple, indicating that the simple and applicable mathematical formula we use is effective.
Unlike the volumetric and subjective planning methods, tissue-based planning methods that use mathematical values,provide to obtain a more natural and aesthetic breast shape. We believe that using the mathematical formula described for measuring arc lengths of semicircular structures in preoperative planning will reduce both complication rates and provide easy, practical, and effective planning in primary breast augmentation cases where Ergonomix implants will be used.
The authors have not received any funding for this paper.

