 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Siddharth Sonwane1* , Shweta Rajendra Kamble2
, Shweta Rajendra Kamble2
1Professor and Head, Department of Orthodontics, Mansarovar Dental College, Bhopal, Madhya Pradesh, India.
2Associate Professor, Department of Oral and Maxillofacial Surgery, Government Dental College, Nagpur, Maharashtra, India.
Correspondence to: Siddharth Sonwane, Professor and Head, Department of Orthodontics, Mansarovar Dental College, Bhopal, Madhya Pradesh, India.
Received date: July 08, 2023; Accepted date: July 19, 2023; Published date: July 26, 2023
Citation: Sonwane S, Kamble SR. The Correlation between Quantitative Cervical Vertebral Maturation and Mandibular Dimensions in Children Aged 8-16 Years: A Cross-Sectional Analytical Study. J Med Res Surg. 2023;4(4):75-79. doi: 10.52916/jmrs234113
Copyright: ©2023 Siddharth S, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted
use, distribution and reproduction in any medium, provided the original author and source are credited.
Background: During growth modification, the mandible plays a crucial role in functional orthopaedic treatment.
To maximize the efficacy and efficiency of functional appliance therapy, one must know when to initiate treatment.
To accurately determine when to initiate functional appliance therapy, the contemporary maturity indicators
utilised are subjective with poor reproducibility and validity. Quantitative cervical vertebral maturity indicators
are quantitative with good reproducibility.
Objective: To determine the correlation between quantitative cervical vertebral maturation and mandibular
dimensional changes in 8–18-year-old growing children.
Material and Method: In this prospective cross-sectional analytical study, 164 samples were employed with an
age range of 8–18 years. Samples were divided into four groups as per the quantitative cervical vertebral maturity
indicator. Pubertal staging was analysed utilising the Li Chang, et al. method on a lateral cephalometric radiograph,
and mandibular dimensions were measured as the total mandibular length of a condylon-gnathion line, the height
of the mandibular ramus from the condylon-gonion intersection line, and the length of the mandibular body from
the gonion intersection-gnathion line.
Statistical Analysis: The data obtained was analyzed using Statistical Package for the Social Sciences (SPSS)
software; descriptive statistics, student t test and bivariant analysis were applied.
Results: The mean total mandibular length was seen at its maximum in periods of high acceleration velocity.
Intergroup analysis shows significant differences between the groups, and there is a strong correlation between
maturational stage and mandibular dimensional change.
Conclusions: During functional orthopaedic treatment planning, the mandible can be utilised as a skeletal
maturity indicator.
Quantitative cervical maturation, Pubertal stage, Mandibular dimension, High velocity acceleration.
The assessment of the mandibular growth is essential to correct Class II skeletal discrepancies using functional appliances. The functional appliances increase growth by stimulating condylar cartilage to induce supplementary lengthening of the mandible [1]. The efficacy of functional appliances therapy firmly depends on the responsiveness of the condylar cartilage, which in turn depends on the growth rate of the mandible. Therefore, the efficacy of functional appliances therapy firmly depends on the responsiveness of the condylar cartilage, which in turn depends on the growth rate of the mandible [1,2].
The growth rate of the human mandible varies throughout development and many previous cephalometric studies have described a peak in mandibular growth (pubertal growth spurt) [3]. Thus, the intensity, onset, and duration of the pubertal peak in mandibular growth are characterized by great individual variations. The greatest effect of functional appliance therapy was observed at the peak mandibular growth period [2,3].
Mandibular skeletal maturity can be assessed by means of a series of biologic indicators, physiologic and biomarkers. With respect to the cervical vertebral method, it has been shown to be useful for the assessment of mandibular skeletal maturation in growing patients, as each stage of this method corresponds to specific anatomic changes in mandibular growth [4].
Hellsing, et al. 1991 showed, there is significant correlation between change in mandibular dimension and length of the cervical vertebral method; the study concluded that reliability and reproducibility of cervical vertebral method is poor (subjective outcome) [1-4].
Hence, the present study objective was to estimate specific mandibular dimensions at specific stage of quantitative cervical vertebral maturation stage. It also aimed to correlate mandibular dimensional changes with various stages of quantitative cervical vertebral maturation.
This was cross-sectional analytical study design, set in the Department of Orthodontics and this study employed 164 samples with age ranges from 8-16 years (12.05 years). Sample included for the study were routine patients visiting the department of orthodontics for orthodontic treatment. Selection criteria for sample was ANB angle should between 0 and 2 degrees.
Subjects were grouped as per the LI-Li Chang, et al. classification into four stages of QCVMI.
|
Group |
QCVMI Stage |
Value |
Sample |
Description of stage |
|
GROUP I |
QCVMI I |
<1.7404 |
41 |
period of accelerating velocity |
|
GROUP II |
QCVMI II |
<2.623 |
41 |
period of high velocity |
|
GROUP III |
QCVMI III |
<3.5199 |
41 |
period of decelerating velocity |
|
GROUP IV |
QCVMI IV |
>3.5199 |
41 |
period of completing velocity |
|
Total |
164 |
|
||
A lateral cephalogram was acquired for each patient using a cephalostat (Panmeca Proline 2015 cc, Finland) and 8 × 10-inch radiography film (Kodak X o mat China). The exposure settings were 72 Kvp, 10 mA, and 1.2 s, with a source-to-mid-sagittal plane distance of 60 inches. To avoid magnification error, all of the cephalometric radiographs were collected from a single machine.
Manual tracings of individual lateral cephalogram by the principal investigator and the cephalometric measuring error was eliminated by repeat random tracing 20% of total lateral cephalograms. The mean value of repeat traced lateral cephalograms were considered for final analysis.
Tracing for QCVMI: Four linear tracing from cervical vertebrae c3 and c4 and one angular tracing from c2 was measured. The tracing and landmarks were shown in Figure 1 and Table 1. The obtained values inserted in below equation and appropriate individual stage was marked. Quantitative cervical vertebral maturation was evaluated from cephalogram by =– 4.13 + 3.57 XH4/W4 + 4.07 X AH3/PH3 + 0.03 X at 2 equation. The measurement based on anterior and posterior borders of C3, C4 and at 2 is angle for at posterior and deepest point and C2. The stages of quantitative cervical vertebral maturation were based on classification of Li Chang, et al. (Figure 1). There were four Quantitative Cervical Vertebral Stages (QCVM), including QCVM I is classified as period of acceleration, QCVM II categorized as high velocity acceleration, QCVM III considered as period of deceleration and QCVM IV classified as period of completion.
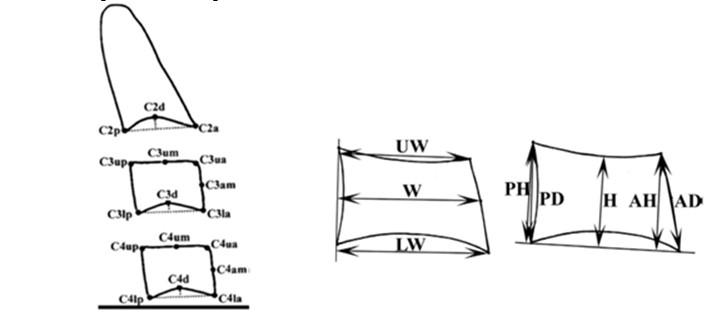 Figure 1: Schematic representation of measuring points used in the cephalometric analysis: C2d, C3d, and C4d.
Figure 1: Schematic representation of measuring points used in the cephalometric analysis: C2d, C3d, and C4d.
|
|
Mandibular dimemsions |
|
||
|
QCVM stage |
Total mandibular Length |
Ramus height |
Body length |
p-value |
|
Stage I (8-11 years) |
9.76 + 115 |
5.07 + 121.46 |
6.115 + 201 |
0.000* |
|
Stage II (12-14 years) |
11.37 + 123 |
6.04 + 106.91 |
7.674 + 631 |
|
|
Stage III (15-16 years) |
10. 22 + 461 |
6.05 + 262.08 |
8.573 + 526 |
|
|
Stage IV (17-18 years) |
10.90 + 192 |
3.78 + 116.25 |
7.932 + 306 |
|
|
Z |
7.818* |
0.000* |
||
|
(Interaction effect p value) |
||||
Statistical analysis: The data obtained were documented onto a Microsoft Excel (2016) worksheet and subjected to descriptive statistical analysis. Shapiro-Wilk analysis used to determine the distribution curve, and kappa value for inter and intra examiner agreement. Student’s t test analysis applied to assess the inter group variation and bivariant correlation was used to determine the difference between QCVM stages and mandibular dimensions.
The Spearman bivariate correlation test was employed for assessing the correlations between quantitative cervical vertebral maturation groups (period of velocity of acceleration, period high velocity of acceleration, period of deceleration, period of completion) and changes in mandibular dimensions.
Mandibular tracings: The total length of the mandible was determined by the distance of the condylon-gnathion line, the ramus height by the distance of the condylon-gonion intersection line, and the body length by the distance of the gonion intersection-gnathion line (Figure 2).
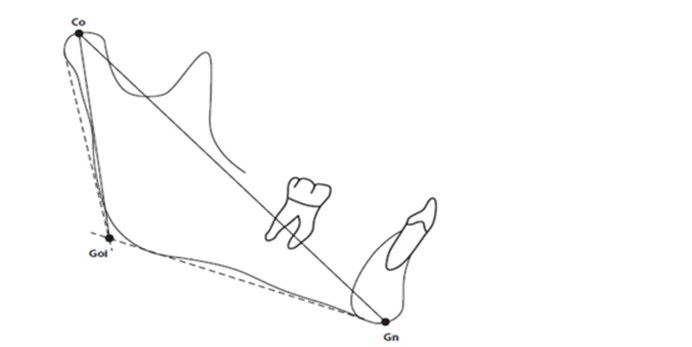 Figure 2: Schematic presentation of Cephalometric measuring points and lines for mandibular dimensions.
Figure 2: Schematic presentation of Cephalometric measuring points and lines for mandibular dimensions.
Table 1 and Graph 1 illustrates differences between the mean values of the total mandibular length, the height of mandibular ramus, and the length of mandibular body with quantitative cervical vertebral maturational stages (QCVM I, QCVM II, QCVM III, QCVM IV). The total mandibular length was the greatest with a mean value of 10.206 with SD 1.204. of mean improvement in the QCVMI stages of children. Furthermore, it shows that mean mandibular total body length was seen greatest in QCVM Stage II i.e., in period high velocity of acceleration and also it demonstrates that there was significant difference with intergroups as the p<0.001 and Z score 7.88 clarify that total mandibular length is maximum and QCVM stage II. Furthermore, the ramus height seems to be very low. Table 2 proves that the strong correlation between total mandibular length and QCVM stages (0.921).
Reliability tests for the determination of quantitative cervical vertebral maturation were conducted by inter-operators (supervisor)between principal investigator and co-guide, with a k value of 0.93 and by intra-operators who performed the test 2 weeks after the first evaluation, with a k value of 1.0. Reliability tests for the total mandibular length measurements between operators (supervisor) and co-guide were conducted using Bland-Altman plots, with mean ± SD values of 0.070 ± 0.079 and limits of agreement values of −0.097 and 0.189.
Table 2: Bivariant correlation between mandibular dimensions and QCVM.|
Variable |
QCVMI |
Total mandibular length |
Ramus length |
Body length |
|
QCVM |
- |
- |
- |
- |
|
Total mandibular length |
0.921 |
- |
- |
- |
|
Ramus length |
0.892 |
0.971 |
- |
- |
|
Body length |
0.941 |
0.973 |
0.978 |
- |
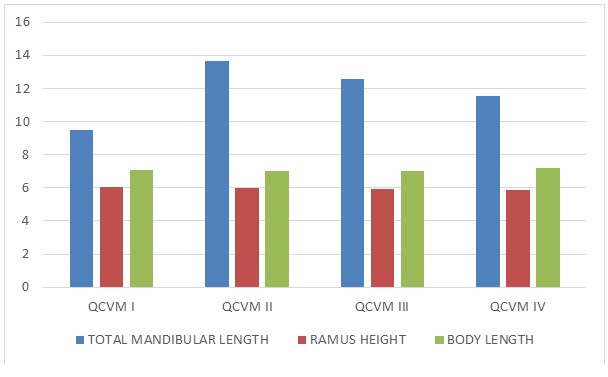 Graph 1: Mean mandibular dimensional changes as per the QCVMI stages.
Graph 1: Mean mandibular dimensional changes as per the QCVMI stages.
This study was aimed to evaluate the correlation between quantitative cervical vertebral maturation and the sequential mandibular growth in individuals of 8 to 18 years. This was a prospective cross-sectional analytical study. The selected samples were included and grouped as per Li-Li Chang, et al. The radiographic quality was of standard without any magnification error. The reliability between the inter and intra examiners was most acceptable with a k value of 0.09.
The statistical outcomes present a strong association, with a grater correlation attained between the quantitative cervical vertebral maturation stage and the total mandibular length (r=0.921), followed by the length of mandibular body (r=0.941) and the height of mandibular ramus (r=0.892).
The maximum volume of mandibular growth appeared during the period of high velocity acceleration (QCVM II). This phase of QCVM II simulates the pubertal phase in cervical maturity indicators and in hand wrist radiograph method [6]. Thus, this type of mandibular dimensional changes has been observed in and reported in previous studies. Furthermore, in most of the cervical vertebral maturity indicators, researchers have observed that the width of the vertebral growth stops and creates chaos in identification of further stages.
In our present study we have taken QCVM maturational stage prescribed by Li Chang, et al. which is objective and can be reproducible. Our objective was to determine both (vertebrae and mandibular dimensions) the variables that are objective rather than subjective. This method of measurement eliminates the demerits of subjective measurement and has good reliability, validity, and reproducibility.
Mandibular development begins with bone remodelling [7]. Mandibular height increases predominantly as a result of alveolar bone growth; however, some bone deposition occurs at the mandibular lower boundary. The mandibular length grows due to bone deposition on the ramus's posterior surface as well as resorption as compensation for the anterior surface. It is accompanied by bone deposition on the coronoid process's posterior surface and conduction on the condyle's anterior surface8. The mandibular breadth grows as a result of bone deposition on the mandible's outer surface and resorption of the mandibular surface. As a result, the mandible grows posterior-superior (backward-upward), resulting in anterior-inferior displacement [4-7].
The literature evidence reveals that mandibular dimensional change attained its maximum size during the pubertal growth phase [4-9]. Thus, most of the investigators suggest that mandibular growth spurts occur, but they show individual variations10. The relationship between maturational stages and mandibular growth has received much attention. However, most of the contemporary maturity indicators are subjective, but the QCVM maturity indicator is the object, and it has been demonstrated to be clinically effective and reliable for the estimation of mandibular skeletal maturation in puberty.
In the pubertal phase of any subject, there is a complex process of morphologic and physiologic changes, and these associated changes are under the influence of multiple factors such as genetic, nutritional, socioeconomic, and environmental aspects, which facilitate both physiological and hormonal processes [11]. An increase in the level of sex hormones triggers bone remodelling, and it is observed that bones grow at a constant rate in the pubertal phase [12]. Therefore, a comparison between patients in the four stages of maturation, i.e., period of velocity, high accelerated velocity, deceleration, and period of completion, could assist a clinician in analyzing the substantial changes in mandibular dimensions so that functional jaw correction would substantially contribute to achieving an effective and efficient [9-12].
In our study, we have observed that total mandibular length was greater in QCVM stage II, the period of high velocity of acceleration. This is because of the mandible (condyle) cartilage, which regulates the various bone formation as per requirement. In high velocity acceleration stage of QCVM, there is greater hormonal release due to which condylar cartilage get ossified on peripheral surface of head of the mandible pushing it downward forward direction resulting in increase in total length [13,14]. This confirms the perception of maximum increase in mandibular length along high velocity acceleration period in accordance with quantitative cervical vertebral maturation. Therefore, the quantitative cervical vertebral maturation method is an effective indicator of mandibular growth during puberty [14]. The application of growth indicators is suggested in clinical practice and research in cases of malocclusion demanding interceptive or functional treatment. The accomplishment of functional appliance can be evaluated by mediation in mandibular length, indicating a relationship between mandibular growth ability and treatment response.
This was a prospective cross-sectional analytical study in which two dimensional measurements were done. The obtained results were implicated in at that time. However, the longitudinal study confirms individual variation in mandibular dimensional change, which can be generalized and applied to everyone.
First time in the research of maturity indicator the variables were objective. The major advantage is good reproducibility and repeatability. In this research mandibular and vertebral bone remodeling can be evaluated. There is 100% elimination of subjective error, hence study can be generalized.
A multi centric longitudinal study is required.
The authors have no conflicts of interest to report.
No

