 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Yussra Khattri* 1, Ayesha Shayan1, Raisa Altaf1, Rabiya Siraj1, Imran Siraj2, Muhammad Ayub Mansoor1
1, Ayesha Shayan1, Raisa Altaf1, Rabiya Siraj1, Imran Siraj2, Muhammad Ayub Mansoor1
1Department of Radiology, Liaquat National Hospital, Karachi, Pakistan.
2Department of Surgery, Liaquat National Hospital, Karachi, Pakistan.
Correspondence to: Yussra Khattri, Department of Radiology, Liaquat National Hospital, Karachi, Pakistan.
Received date: January 13, 2023; Accepted date: January 31, 2023; Published date: February 07, 2023
Citation: Khattri Y, Shayan A, Altaf R, et al. The Case Report of an Intra-Abdominal Organized Gossipiboma: An Incidental Subsidiary Finding. J Med Res Surg. 2023; 4(1):5-7. doi: 10.52916/jmrs234097
Copyright: ©2023 Khattri Y, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted
use, distribution and reproduction in any medium, provided the original author and source are credited.
Post-operative and intraoperative complications of surgery are encountered commonly, often serious and unavoidable [1]. One of the rare complications is a gossypiboma, which is frequently not reported to avoid medicolegal implications. Gossipiboma is a rare complication that can occur due to human negligence. Gossipiboma’s form as a complication of inflammatory reaction to a surgical sponge or a laparotomy pad left mistakenly in the body of the patient after a surgical procedure. The term Gossipiboma is a combination of two words from two different languages; Gossypium a Latin word which mean cotton and boma a Kiswahili word which means plan of concealment. Their incidence is reported to be 1 in 1000 to 1500 surgery. We present here a case of a 67-year-old male who had a history of right-sided Percutaneous Nephrolithotomy (PCNL) five years back. No immediate post procedure complications occurred however the patient presented to the Outpatient Department (OPD) with left flank pain and his Computed Tomography (CT) scan was done which showed an organized Gossipiboma.
Gossypiboma, Computed Tomography (CT) imaging, Human error, Postoperativen
Post-operative and intraoperative complications of surgery are encountered commonly, often serious and unavoidable [1]. One of the rare complications is a gossypiboma, which is frequently not reported to avoid medicolegal implications. Gossypiboma is also called textilomas, cottonied and guazemo. Patients with a retained surgical sponge may or may not be symptomatic [2]. Therefore the diagnosis is often incidental. Computed Tomography (CT) is the best method for the detection of gossypiboma and their complications [2]. majority of the cases demonstrate non-specific CT appearances as an abnormal density or complex mass. The mass may contain wavy, striped, high-density areas that represent the sponge itself. After contrast administration it show high-density capsule with low density center which is characteristic of gossypiboma but it is difficult to distinguish from a hematoma and abscess [1,3-5]. This condition can be prevented by regular practice of counting instruments and gauze pieces before and after surgical procedures.
A 67 year old male patient presented in the out patient department of our hospital with complains of left flank pain and burning micturition. His vitals on arrival were blood pressures of 130/80 mmhg, pulse 85 beats/min, respiratory rate 19 breaths per min and temperature 98°F. On examination abdomen was soft non-tender, chest unremarkable, Central Nervous System (CNS) unremarkable. He had a past history of right-sided Extracorporeal Shock Wave Lithotripsy (ESWL) 5 years back from periphery hospital. The differentials of the clinician included renal calculi, prostatic cause and a possible retroperitoneal mass. His baseline investigations were unremarkable however his TLC count was 11.4. His CT pyelogram showed a well-defined rounded mass with curvilinear metallic density in it in the retroperitoneal region on right side. It was abutting the psoas muscle medially, colon laterally and lower pole of right kidney superiorly however was separate from right kidney representing a gossipiboma. On exploratory laparotomy a retained gauze piece was seen in right retroperitoneal region with no evidence of surrounding adhesions. The patient had an uneventful postoperative course and was discharged well (Figure 1 and 2).
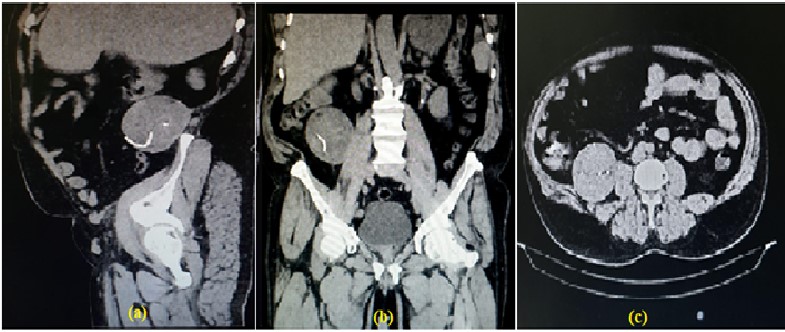 Figure 1: Shows (a) saggittal, (b) coronal and (c) axial cute of the same patient showing a well defined hypodense mass in retroperitoneum on right side with a curvilleniar mettalic density within it.
Figure 1: Shows (a) saggittal, (b) coronal and (c) axial cute of the same patient showing a well defined hypodense mass in retroperitoneum on right side with a curvilleniar mettalic density within it. Figure 2: Shows the postoperative image of the gauze piece.
Figure 2: Shows the postoperative image of the gauze piece.Gossypiboma is an avoidable iatrogenic error that may cause severe immediate or delayed complications. It is caused by forgotten gauze in the patient’s body intra-operatively. It’s occurrence is often more usual than reported, in lieu of its medicolegal repercussions. It inadvertently adds to morbidity and, in severe cases, mortality. The misdiagnosis with malignant lesions and their consequent unnecessary and/or invasive investigations, or undergoing a second surgery in order to resect the foreign body takes a toll on the patient, psychologically and economically. The process of counting the gauze according to World Health Organization (WHO) protocol is, before incision, before the closure of cavity within a cavity, as wound closure begins and at skin closure or end of procedure. Lastly, at the time of permanent relief of either the scrub person or the circulating nurse. Civil lawsuits are being taken up against surgeons more frequently. According to Article 21, there are many medicolegal implications of medical negligence. Article 21 of the Constitution says, ‘No person shall be deprived of his life or personal liberty except according to procedure established by law’. The Supreme Court held that ‘Thus, a doctor can’t be held criminally responsible for patient death, unless his negligence or incompetence showed such disregard for life and safety of his patient as to amount to a crime against the State’. Court further says that, ‘Thus, when a patient agrees to go for a medical treatment or surgical operation, every careless act of the medical man can’t be termed as “Criminal”. It can be termed as “Criminal” only when the medical man exhibits a gross lack of competence or inaction and wanton indifference to his patient’s safety and which is found to have arisen from gross ignorance or gross negligence. The legal position is almost firmly established that where a patient dies due to the negligent medical treatment of the doctor, the doctor can be made liable in civil law for paying compensation and damages in “Tort” and at the same time, if the degree of the negligence is so gross and his act was reckless as to endanger the life of the patient, he would also be made criminally liable for offense under section 304-A of IPC’. Hence a medical doctor or officer is liable to punishment as per the Article 21 for medical negligence [6].
Gossypibomas are the most common retained surgical items, among others including forceps and needles [7]. A cotton gauze will easily stain with blood and mould into an unrecognizable form that can easily be missed. Its estimated occurrence is about 1 out of 1,000– 1,500 intra-abdominal operations and 1 out of 300–1,000 of all operations [8]. The burden of the mistake is on the surgeon and staff while the various possible reasons of sponge retention include emergency surgery, unexpected change in the surgical procedure, disorganization (e.g. poor communication), hurried sponge counts, long operations, unstable patient condition, inexperienced staff, inadequate staff numbers, and obesity [9]. Following the misadventure of a retained laparotomy sponge, some patients are asymptomatic for many years after surgery while others present with various clinical presentations. the main signs and symptoms are abdominal pain (42%), palpable abdominal mass (27%), and fever (12%) [10]. The reaction to a retained sponge may either be exudative or aseptic fibrous type. Of these, the exudative reaction presents early with symptoms of generalized sepsis or abscess formation. The delayed response involves formation of adhesions, granulomas or pseudo tumors. The patient may present with non healing wounds or discharging sinuses, or develop secondary complications like intestinal obstruction and fistula formation [11]. Their radiological features may simulate a hydatid cyst or tumors such as retroperitoneal tumors, desmoid tumors, ovarian teratoma, mesenchymal tumors and pancreatic tumors [12]. Characteristic finding on CT includes heterogeneous mass, enhanced wall, multiple air foci and hyperdense linear structure (radiopaque strip marker). 7 emphasis should be made on counting sponges before closing the incision, as well as a thorough check of the body cavity should be done to minimize such unwarranted mishaps. Radiographically marked sponges paired with intra-or post-surgical X-ray surveillance can be used to aid in their localization [13-14].
Gossypiboma should be considered one of the differentials in those patient who present with unexplained fever or abscess in postoperative period. Radio imaging studies are valuable tools to aid in diagnosis. This avoidable condition can be eradicated by improving surgical practice.
The author declare no competing financial interest.
Written informed consent was obtained from the participant’s parents for publication of this study.
No.

