 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Yulia Bogdanova Peeva*
Department of Social Medicine and Public Health, Faculty of Public Health, Medical University, Plovdiv, Bulgaria.
Correspondence to: Yulia Bogdanova Peeva, Department of Social Medicine and Public Health, Faculty of Public Health, Medical University, Plovdiv, Bulgaria.
Received date: September 4, 2024; Accepted date: September 18, 2024; Published date: September 25, 2024
Citation: Peeva YB. Subjective Factors in Orthodontic Treatment, Q-Methodology as a Tool to the Assessment of Motivation, Compliance and Satisfaction in Orthodontic Treatment: Quaestiones Morales et Ethical Communications (ex lat). J Med Res Surg. 2024;5(5):104-109. doi: 10.52916/jmrs244147
Copyright: ©2024 Peeva YB. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Introduction: One of the essential factors for evaluating the successful orthodontic treatment is a patient’s satisfaction. The orthodontist can apply very high clinical performance of the tasks set at the beginning, but they do not always coincide with the patient's requests due to the lack of objective assessment. The Q-methodology offers an innovative and qualitative approach that combines the compatibility of many subjective factors and meets the patient's requirements. The research is sociological, specific problems can be explored in depth and fulfil the patient’s expectations. It works with a small number of respondents, and most importantly, it emphasizes the patient-centered approach. The aim of the present study using Q-methodology was to evaluate the subjective factors in orthodontic treatment and to achieve the best outcomes. Materials and Methods: Data analysis and statistical processing included Factor Analysis, PQ Method 2.35 with PQROT 2.0. 280 children aged 13 to 18 and 325 parents aged 35 to 55 were studied. The average age for the children was 16.67±2.17, and for the parents 42.18 ± 3.17. An interview (the pilot study) was conducted with 40 respondents, on the basis of which 30 evaluation opinions were formed using the Q-methodology. The studied factors that support children's motivation during orthodontic treatment are compliance and satisfaction as a result. Results and Discussions: Three factors are summarized for children - the most important is "aesthetics"; four are the factors for parents "prevention of future oral problems" was rated highest by them. Conclusions: The Q-methodology shares the views of the quantum theory as well, that communicability exists in different probabilistic states. This determines the possibility of subjective factors "to be counted", i.e. to give an objective assessment as a result of subjective factors.
Q-methodology, Subjective factors, Orthodontic treatment.
Q-methodology is known as a tool for evaluating subjective factors in sociology. An extremely up-to-date way of predicting and using motivation as the main factor in starting and conducting orthodontic treatment. Significant advantages of the method compared to traditional research are that it uses a person-centered approach and the opportunities for development and perspective in front of the individual. In this way, the attitudes and expectations of the child and the parents are generalized, and not seen as separate events happening to the child. In addition, social norms that are attractive or important not only to the individual but also to society are included in the communication [1,2,3].
Patient satisfaction is subjective, but it is a sought after factor by the orthodontist. In the long run, it is a lack of communication problems, more referrals and last but not least, it is related to the orthodontist's satisfaction. Ethical relationships with people can be compromised when there is payment for a health service or product. The legislation and the health insurance system place the doctor into a specific position. Contrary to the Hippocratic Oath and commitment to humanism, which medicine postulates (lex postulate), orthodontic (and not only) treatment is paid for [4,5,6]. And while the surgeon must solve his emotional problems for the view that his work offers, the psycho-emotional problems of the orthodontist refer to the responsibility to the treatment undertaken and above all to the patient [7]. This puts the doctor's satisfaction in question. Is dealing with emotions a waste of time? The patient's and their own? Definitely, it is a waste of time because knowledge is a norm that is not measured by emotions. Now, more than ever, human being suffers from the lack of good word and kind relationships.
The patient's knowledge is non-medical and limited to that of the physician. However, the knowledge of both doctors differs. When the patient is a doctor, is communication expected to be more difficult? Emotionally, doctor and patient are one because knowledge is infinite but concrete and everyone has a right to be informed. This is the point of trust.
In 1996, analyzing the Roman foundations of civil traditions in Lex Aquilla II, Zimmerman was primarily concerned with the protection of the free man's bodily integrity. The final section explores various contributions to the modern, generalized law of torts [8].
The behavioral algorithm for exploring awareness, motivation and cooperation, etc. factors for successful orthodontic treatment using Q-methodology includes a preliminary interview. The pilot study was conducted personally involved children - n1=15; parents - n2=25. Next, a list of reasons is generated that potential patients consider being the factors that are important to them and define the need for orthodontic treatment. There are several key points when constructing the Q-matrix.
Thirty different opinions are offered for children and parents. After carrying out interviews in the dental office, those that are most important for children and parents were specified. The categories used were 11 (with scale values from -5 to +5 and 0 as the neutral position). A Q-matrix is being built, in which 280 children and 325 parents take part. The success of the methodology is due to the diversity of categories used in the studies [9,16,17].
Cooperation during orthodontic treatment determines the duration, results and satisfaction of the patient and parents. Orthodontic services provided can lead to functional limitations, discomfort and pain, as well as increase the child's anxiety in the office. Negative experiences are a reason for refusal of cooperation and empathy on the part of the patient [9,10,11,12]. According to other researchers, the relationship between the patient's expectations at the beginning of ortho treatment, his ability to cope with the discomfort, the type and severity of the noted discomfort and its overall impact on the patient's consent is significant and direct [13].
So far, most studies on patients' subjective experiences of orthodontic treatment have been conducted using oral health and anxiety assessment questionnaires - SF-36, MHI-5, CHQ-12, etc. [10,14,15]. In order to reduce subjectivity when evaluating the children's opinion, the parents were also surveyed. Researchers of the psychological characteristics of patients, by means of questionnaires, find that a major drawback of this type of study is the large sample size. Another disadvantage is considering one opinion in isolation, when it is quite often related to or dependent on other factors. It does not go into the essence of the problem due to the subjectivity of the factors on which it depends. Significant and painful problems in society are often not analyzed, because their determining factors cannot be evaluated objectively [17,18]. The following authors are of significant interest for the improvement of the Q-methodology (Table 1):
Table 1: Characteristics and differences in Q-methodology research.|
Author |
Prabakaran R, Seymour S, Moles D, Cunningham S. Motivation for orthodontic treatment investigated with Q-methodology: patients’ and parents’ perspectives. American Journal of Orthodontics and Dentofacial Orthopedics, 2012; 142:213–220.[9] |
Yao L, Xu X, Ni Z, et al. Use of Q methodology to assess the concerns of adult female individuals seeking orthodontic treatment. Patient preference and adherence, 2015; 9:47-55.[16] |
Tang X. Motivation of adult female patients seeking orthodontic treatment: an application of Q-methodology. Patient Preference and Adherence 9 (2015): 249-256.[15]
|
Batra P, Daing A, et al. Impact of altered gingival characteristics on smile aesthetics: Laypersons' perspectives by Q sort methodology, American Journal of Orthodontics and Dentofacial Orthopedics, 2018, Vol 154, Issue 1,pp 82-90.[18] |
|
Material and methods |
1. Interview conducted and formation of 32 opinions with 60 respondents; 2. Q-methodology |
1. The researchers formed 41 opinions without conducting an interview; 40 women were studied; 2. Q-methodology |
1. Conducted interview and formation of 35 opinions with 42 women; 2. Q-methodology |
1. 45 men and 55 women. The effectiveness is higher with a smaller participant group - 40 to 60 p. The study was done by having laypersons rate 67 img of smiles, 2 were not modified. 2. Q - methodology |
|
Data and statistical processing |
Factor analysis, SPSS software (version 17.0; SPSS, Chicago, Ill) |
Factor analysis, PQ Method 2.35 with PQROT 2.0 |
Factor analysis, PQ Method 2.35 with PQROT 2.0 |
t-tests or non-parametric Wil-coxon signed rank sum tests, ver. 16.0; SPSS, Chicago III. |
|
Derived factors |
Three factors were derived for children - the most important is "aesthetics"; four are the factors for parents - "prevention of future oral problems" was the most significant. |
1st factor: Lack of awareness about orthodontic treatment, 2nd factor: Impact on "social contacts" in unmarried women, 3rd factor: Importance of "dento-facial vision and speech", 4th factor: The cost, pain and oral hygiene. |
1st factor: Self-perception of oral vision, 2nd factor: Aesthetics and function, 3rd factor: Importance of circulation, 4th factor: To increase future satisfaction with dento-facial aesthetics. |
-Variation in interdental papilla (black triangles) was the most negatively ranked gingival factor closely followed by color changes of the gingiva caused by inflammation and pigmentation; -Gingival contour and gingival zenith had the least impact on smile aesthetics rankings; -Changes in the free gingival margin with and without recession were moderately perceived. |
The studies that combine quantitative and qualitative methods and make it possible to systematically study subjectivity on a scientific basis are very relevant. The Q-methodology allows for an overview of subjective viewpoints. Enables psychological research of the subjective sensations and perceptions of the participants, as well as their evaluation for analysis.
Dentofacial problems can affect patients' daily life. These in turn influence social functioning and behavior; in a school or group setting. The impact on quality of life was examined in a study from 2015 [19]. Of particular interest are the results, as they support the idea of improving oral health through selfregulatory behavior. In the present study, the assessment of the child is very important. There are separate opinions in the literature about the positive example that the dentist, and in particular the orthodontist, sets through his personality [20]. The doctor educates behavioral, hygienic, educational, etc. habits of their patients. However, the rate of failure to complete treatment is also high and common. Failure came with patient non-compliance or dissatisfaction, incorrect diagnosis and treatment. In all respects, the successful outcome of treatment depends mainly on the patient's attitude towards orthodontic treatment. Unconscious oral problems, low level of motivation and unfavorable personal and social relationships are the main and most important factors for unsatisfactory treatment results [15,21]. The efforts of orthodontists to seek and satisfy patient expectations can be realized with both clinical and sociological research methods in medicine. Q-methodology allows subjective factors to be evaluated as objective. Q-methodology is a potential tool for upgrading data in order to objectify it. For example, satisfaction rating comes after motivation. The cooperation of the patient is very important and its chronological and natural place in the treatment processis between motivation and satisfaction Figure1: Figure 1: Chronological and natural place in the treatment process.
Figure 1: Chronological and natural place in the treatment process.In the present study, the relationship between the child's cooperativeness, formed as a result of upbringing in the family, and the desire to undergo orthodontic treatment was sought.
Data analysis and statistical processing included Factor Analysis, PQ Method 2.35 with PQROT 2.0. 280 children aged 13 to 18 and 325 parents aged 35 to 55 were studied. The average age for the children was 16.67 ± 2.17, and for the parents 47.18 ± 2.14, P>0.05. An interview (the pilot study) was conducted with 40 respondents, on the basis of which 30 evaluation opinions were formed using the Q-methodology, P(u)=0.95, Sx=6.35 and Δ=1.214. The studied factors that support children's motivation during orthodontic treatment are compliance and satisfaction as a result. Data are presented in Table 2 and 3:
Table 2: Socio-demographic characteristics of the observed children.|
Age (years) |
Sex |
Total |
% |
Sp |
|||||
|
Boys (n) |
% |
Sp |
Girls (n) |
% |
Sp |
||||
|
13 |
7 |
5.00 |
1.84 |
11 |
7.86 |
2.27 |
18 |
6.43 |
1.47 |
|
14 |
26 |
18.57 |
3.29 |
22 |
15.71 |
3.08 |
48 |
17.14 |
2.25 |
|
15 |
28 |
20.00 |
3.38 |
32 |
22.86 |
3.55 |
60 |
21.43 |
2.45 |
|
16 |
39 |
27.86 |
3.79 |
33 |
23.57 |
3.59 |
72 |
25.71 |
2.61 |
|
17 |
21 |
15.00 |
3.02 |
23 |
16.43 |
3.13 |
44 |
15.71 |
2.17 |
|
18 |
19 |
13.57 |
2.89 |
19 |
13.57 |
2.89 |
38 |
13.57 |
2.05 |
|
Total |
140 |
50.00 |
2.99 |
140 |
50 |
2.99 |
280 |
100 |
- |
|
Age (years) |
Sex of the parents |
Total |
% |
Sp |
|||||
|
Fathers (n) |
% |
Sp |
Mothers (n) |
% |
Sp |
||||
|
35 |
27 |
22 |
3.61 |
24 |
12.18 |
2.33 |
51 |
15.69 |
2.02 |
|
45 |
67 |
52.34 |
4.41 |
97 |
49.24 |
3.56 |
164 |
50.46 |
2.77 |
|
55 |
34 |
26.56 |
3.90 |
76 |
38.58 |
3.47 |
110 |
33.85 |
2.62 |
|
Total |
128 |
39.38 |
2.71 |
197 |
60.62 |
2.71 |
325 |
100 |
- |
According to Lewit and Verolainen, parents have the most essential role in motivating and obtaining consent from the child for the upcoming long-term treatment [15]. Other motivational researchers support the idea that they can predict some negative changes in a child's mood and thus thwart treatment compromise as well as neutralize factors that impaircommunication [19,20,21].
The first step of the Q-methodology involves a preliminary conversation with the parents. Questions discussed: "Why do you want your child to wear braces?" and "What you don't like in your child's smile?". However, according to the parents, it is not so much the aesthetics that are important as the prevention of future functional problems if their child is not treated. Three factors are summarized for children - the most important is "aesthetics"; four are the factors for parents- "prevention of future oral problems" was rated highest by them (Figure 2).
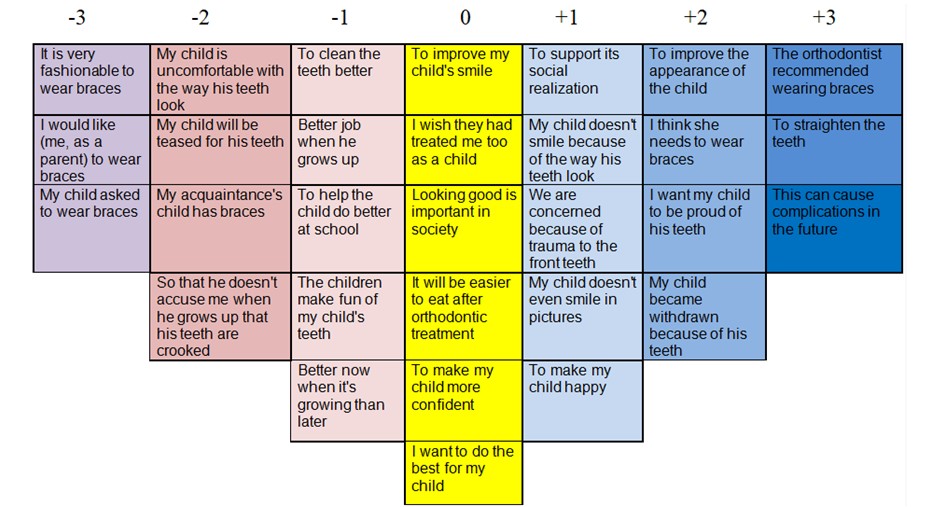 Figure 2: Q-matrix to study the subjective factors for orthodontic treatment.
Figure 2: Q-matrix to study the subjective factors for orthodontic treatment.Motivation and cooperation for the actively seeking treatment are the basis of ultimate satisfaction. Improving appearance and achieving functional oral health are important motivations for orthodontic treatment. Social and cultural factors have also been shown to influence perceived need [9,13,18,19]. In recent years, due to increased awareness, the demand for orthodontic services has increased significantly. No difference was observed in the registered satisfaction of patients of both sexes, P>0.05 (χ2=0.29).
The opinion, "It is very fashionable to wear braces" relies on approval and socially accepted norms. It does not coincide categorically with the main reasons for seeking orthodontic treatment, but it was brought out after the interviews with the parents as important for them.
The task to assess the motivation of parents through Q-methodology is possible on the basis of drawn high correlations (with ratios above rxy=0.7) in the following statements:
The parents’ examination of motivation with Q-methodology (Table 4) also shows reasonable assumption. Namely, "It can cause complications in future without treatment.", P>0.05 for both sexes. Four factors have been determined for the parents’ motivation and their position at Q-matrix are presented at Table 4.
Table 4: Factors evaluating subjective factors for children and parents.|
Q-matrix |
Factor 1: “Esthetics and needs of orthodontic treatment”
|
Factor 2: “Positive attitudes from orthodontic treatment” |
Factor 3: “The choice through informed consent” |
Factor 4: “The importance of social environment” |
|
+3 |
It can cause complications in future without treatment, rxy=0.81
|
|
|
|
|
+2 |
|
I want my child to be proud with its teeth, rxy=0.87 |
To improve the facial appearance of my child, rxy=0.74 |
|
|
+1 |
|
To support its social realization in the future, rxy=0.91 |
|
|
|
0 |
I want to do the best for my child, rxy=0.66 |
|
|
|
|
-1 |
|
|
Better now, when growing, than later, when he/she grows, rxy=0.79 |
|
|
–2 |
|
|
|
The child of my friends has brackets, rxy=0.92 |
|
-3 |
It is very cool to wear braces, rxy=0.76 |
|
|
|
The results obtained when determining the two factors using the Principal Components technique provide information about the reasons that motivate parents to start orthodontic treatment. The names of each factor confirm the opinions that most accurately characterize the factors themselves (Table 5).
Table 5: Initial solution with two factor conditions using Factor analysis.|
No. |
Factors |
Initial status |
Factor’s weight (rxy) |
P |
|
1 |
Better now, when growing, than later when he/she grows up |
1 |
0.85 |
P=0.001 |
|
2 |
To improve the facial appearance of my child |
1 |
0.83 |
P=0.001 |
|
3 |
I think it is necessary to wear braces |
1 |
0.79 |
P=0.001 |
|
4 |
To support its social realization in the future |
1 |
0.86 |
P=0.001 |
|
5 |
I want my child to be proud with its teeth |
1 |
0.86 |
P=0.001 |
|
6 |
It is very cool to wear braces |
1 |
0.66 |
P=0.001 |
|
7 |
The child of my friends has brackets |
1 |
0.86 |
P=0.001 |
The Q-methodology shares the views of the quantum theory as well, that communicability exists in different probabilistic states. This determines the possibility of subjective factors "to be counted", i.e. to give an objective assessment as a result of subjective factors.
None.
The authors declare no conflicting interest.

