 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Uzma Panhwer* , Saman Arain, Yussra Khattri, Danial Khalid Siddiqui, Afifa Umar, Muhammad Umer Farooq
, Saman Arain, Yussra Khattri, Danial Khalid Siddiqui, Afifa Umar, Muhammad Umer Farooq
Department of Radiology, Liaquat National Hospital, Karachi, Pakistan.
Correspondence to: Uzma Panhwer, Department of Radiology, Liaquat National Hospital, Karachi, Pakistan.
Received date: January 21, 2025; Accepted date: February 13, 2025; Published date: February 20, 2025
Citation: Panhwer U, Arain S, Khattri Y, et al. Spontaneous Infected Subdural Hematoma in an Infant: A Case Report J Med Res Surg. 2025;6(1):18-21. doi: 10.52916/jmrs254160
Copyright: ©2025 Panhwer U, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Subdural Empyema (SDE) is a rare infection occurring in the subdural space, with a higher incidence rate among infants. Infants typically have a 1%-2% SDE incidence rate. The most common causes of infected subdural hematoma are gastrointestinal or urinary tract infections.
However, there have been few reports of infected subdural hematoma in preexisting chronic subdural hematoma without a known cause, as observed in this case.
Symptoms commonly reported by patients include headaches, fever, altered sensorium, vomiting, and seizures. Notably, only half of the affected individuals experience the classic trifecta of headaches, fever, and vomiting. In severe cases, the mass effect can lead to complications such as hemiparesis, cranial nerve palsy, and papilledema.
To diagnose SDE, a CT scan is typically performed, which may reveal a hypodense area over the hemisphere or along the falx. The use of contrast material can enhance the differentiation of the infected area. However, the preferred diagnostic method is MRI with gadolinium enhancement. In cases where symptoms are limited to headaches and fever without other neurological symptoms, urgent MRI may be necessary, with sedation administered as needed.
Spontaneous subdural empyema in the presence of subdural hematomas is extremely rare. The presented case adds to the limited literature by describing a confirmed infection on the evacuated side of a subdural hematoma.
Physicians should be aware of this potentially life-threatening complication and consider subdural empyema diagnosis in newborns based on strong clinical and radiological suspicion. Early therapeutic drainage is emphasized as the primary mode of treatment for SDE.
Subdural Empyema (SDE), CNS infections, CT scan, Subdural hematoma, Abscess, Burr hole.
Infected subdural hematomas are not prevalent, with just around 50 cases recorded in the literature. The most often reported pathogens were E. Coli and salmonella, with urinary tract infections or gastrointestinal diseases being the most common causes. While most subdural hematomas are produced by trauma or injury, extremely uncommon cases of infected subdural hematomas without a definite source of infection, such as in our case, are documented [1,2]. While subdural empyema predominantly occurs due to spread of infection near the cranium, infected subdural hematomas remain a rare entity that are thought to occur from hematogenous spread of infection. The risk factors for spontaneous subdural hematomas include advanced age, alcohol misuse, hypertension, and use of blood thinners [1,2].
An infection of the potentially extensible subdural area is known as Subdural Empyema (SDE) [3]. Between the meninges' top layer, the dura, and the arachnoid is where subdural empyema or loculated infection, occurs. It's possible for the empyema to form in the spinal canal or intracranially [4]. SDE in older children usually results from the direct extension of sinusitis or otitis media into the extracranial spaces and in infants as a consequence of purulent meningitis [2,3]. Infants typically have a 1%-2% SDE incidence [5]. The uncommon condition known as spinal subdural empyema may arise from osteomyelitis or hematogenous infection [2,4]. This infrequent but potentially catastrophic intracranial infection will always be lethal if untreated [3,5]. The purpose to present this case is to describe the significance of a timely diagnosis of subdural empyema in infants depending on strong clinical and radiological suspicion, as well as urgent therapeutic drainage as a main means of treatment for SDE [5].
Patient is a 11-month-old male baby known case of developmental delay with no significant birth history. Presented to the emergency department complain of left sided hemiplegia and ptosis for 8-month and fever with vomiting for 10 days. The family denied any history of trauma or fall.
Computed Tomography (CT) of the brain was done from periphery 2 months ago which showed a subdural hematoma but baby was on conservative treatment using antibiotics and did not gone evacuation so by time this hematoma eventually developed into empyema. On examination tone was increased and an isocoria and bruises over wrist observed therefore clotting profile was sent which shown deranged INR so vitamin k was given and FFP were transfused CT brain plain was done which showed a well-defined rounded cystic mass lesion in right temporo-parietal region with peripheral slightly thick hyperdense walls (Figure 1).
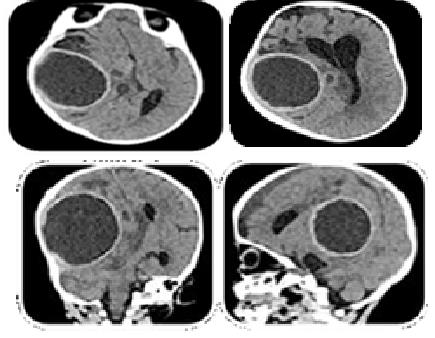 Figure 1: Pre-operation CT scan axial, coronal and sagittal view.
Figure 1: Pre-operation CT scan axial, coronal and sagittal view.
Neurosurgery review taken for suspected abscess on CT brain plain. For which parents were counseled for surgical evacuation. Before which MRI brain contrast was done showing a large well defined, extra axial abnormal signal intensity area in right fronto-parieto-temporalregion. which showed thick T2 hypointense rim, tiny lobulations along its posterior aspect and measures 5.8 × 5.5 × 6.1cm (AP × TS × CC). It was causing significant displacement and compression over adjacent brain parenchyma, right basal ganglia, thalamus, body of right lateral and 3rd ventricles and mid brain with midline shift of 2.8cm towards left. It also showed restricted diffusion and appeared heterogeneous with predominantly iso to hyperintense signals on T1 and inhomogenous low signals on T2 weighted images with negligible peripheral post contrast enhancement. It was confirmed as an organized subdural/extra dural hematoma.
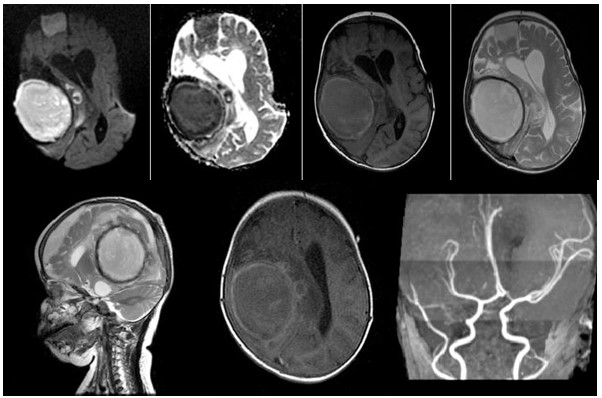 Figure 2: Pre-Operation MRI with DWI, ADC, T1, T2 (axial), sagittal T2, axial T1+C and MRV.
Figure 2: Pre-Operation MRI with DWI, ADC, T1, T2 (axial), sagittal T2, axial T1+C and MRV.
Multiple small areas of similar signal characteristics are were also seen adjacent to it and on MRA right posterior cerebral artery and most of peripheral cortical branches of right middle cerebral artery were compressed (Figure 2). Patient undergone right parieto-occipital craniotomy and evacuation of abscess with excision of capsule. Post operatively patient was vitally stable and repeat scan showed post-surgical changes with areas of haemorrhage (Figure 3). Intraoperative cultures were sent from the subdural space grew penicillium species and blood cultures grew coagulase negative styphylococcus.
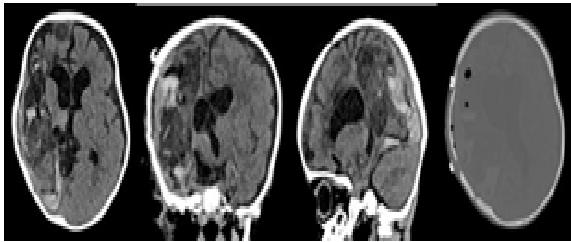 Figure 3: Post-operation CT scan axial, coronal sagittal and axial bone window.
Figure 3: Post-operation CT scan axial, coronal sagittal and axial bone window.
Infected subdural hematomas being uncommon, with only about 50 instances reported in the published literature. The most commonly reported pathogens were E. Coli and salmonella, with urinary tract infections or gastrointestinal illnesses being the most prevalent origins. While most subdural hematomas are caused by trauma or injury but exceedingly rare instances of infected subdural hematomas without a clear source of infection, like in our case, are known [1,2].
A neurosurgical emergency called subdural empyema still has a fatality rate of up to 40% if not diagnosed early [6]. With timely investigation, prompt treatment, and sufficient post-operative rehabilitation, severe neurological consequences and subdural empyema fatalities can greatly be decreased with a survival rate of more than 90% [5]. It comprises 20% of all intracranial abscess cases. According to studies, intracranial subdural empyema poses a risk to two different age groups Children and young adults. Commonly effected age group is 10 to 40 years old represent about two thirds of patients. Men can account for up to 80% of cases compared to women [7,8].
Subdural empyema refers to intracranial purulent material discovered between the dura and arachnoid mater. SDE is classified anatomically in three types 1; Supratentorial 2; Infratentorial, and 3; Spinal canal-related [3,5]. Any infection when entering the subdural area takes up this potential space until constrained by certain boundaries, such as the falx cerebri, tentorium cerebelli, base of the brain and foramen magnum remain limited. It can bursts through the dura and spreads throughout the brain if not have boundaries [7]. There are numerous routes for infections to enter the cerebral space. The haematogenic route, which involves cerebral arteries like the diploe veins or endolymphatic pathways, is one such approach. The second pathway originates in the suppurative process occurring in the sinus and ear. Osteomyelitis and direct invasion into the intracranial compartment are caused by the infection's progression [5,8]. The most frequent symptoms reported by patients are headaches (78-83%) fever (72-96%) abnormal sensorium (56-67%) vomiting (50%) and seizures (29-56%). Only 50% of individuals exhibit the clinical triad of headaches, fevers, and vomiting. The mass effects sometimes can lead to papilledema, cranial nerve palsy and hemiparesis [8,9]. The SDE appears like a developing mass lesion as it advances, which happens following trauma-related increased intracranial pressure and cerebral intraparenchymal penetration.
Secondary to the interruption of blood or Cerebrospinal Fluid (CSF) flow brought on by the elevated intracranial pressure, cerebral edema and hydrocephalus may also be present [9].
Rarely, subdural empyemas may form over the course of two to three weeks. As a result, the empyema may emerge with symptoms that are suspicious of a brain abscess since specific cranial pain may not develop in these circumstances and previous antibiotic treatment for sinusitis or otitis may conceal basic symptoms [6].
White blood cell count, erythrocyte sedimentation rate, and C-reactive protein level can all be noticeably raised and can be used as screening methods to determine whether patients need to have imaging done. Children who have hyperglycemia may be more susceptible to sinogenic cerebral empyema [8,10]. Once increasing intracranial pressure has been ruled out, lumbar puncture will be useful in determining whether meningitis is present or not [5]. Polymicrobial infections are quite prevalent. Although the Streptococcus milleri group predominates in cultures, there are also additional streptococcus species, staphylococcus species, and anaerobic gramme positive and negative species that have been cultured [6,10] On radiological imaging the MRI with gadolinium enhancement is the preferred diagnostic method for intracranial and spinal SDE. SDE is characterized by a fluid collection with a contrast enhanced rim. The extraaxial fluid and its rim enhancement can be seen more clearly on the MRI than on the CT. When it comes to identifying the intraaxial involvement, diffusion-weighted imaging sequence has proven to be more accurate. The interhemispheric collections and convexity have signals that are low on T1 weighted pictures and somewhat high on T2 weighted images. T1 weighted images show cerebral edema as hyperintensity. A Magnetic Resonance Venography (MRV) can be performed concurrently to check for venous sinus thrombosis [8-10].
The CT scan will show the empyema as a narrow, hypodense subdural lesion with linear enhancement of the medial surface. Because cerebral ischemia and cerebritis have a greater impact on edema and consequent mass effect than the abscess's actual volume does, the mass effect that is present is typically disproportionate to the abscess's volume. If an MRI is not possible or is not recommended due to the patient’s condition like comatose or very unwell CT scan is done. In spinal SDEs, CT myelography is recommended [3,7,8].
A bulging fontanelle can be seen in infants but transillumination might not be positive because the empyema is too thick. Ultrasonography has been applied here as a quick diagnostic technique that show convexity collections that are more echogenic, which consist of thick hyperechoic inner membranes or fibrinous threads that are hyperechoic, and the pia-arachnoid that is more echogenic [4,8].
Subdural empyema is an acute emergency and should be treated surgically. Extensive craniotomy with irrigation is the preferred method because it improves the outcome in SDE by permitting wide exposure and better evacuation of subdural purulent material.
However, imaging can correctly localize the collecting pus that can be emptied by burr hole implantation as in our case [7,8,11]. Early introduction of antibiotics has cut mortality and lowered complication rates in ISE to 15-41% [8]. When the pus is in thin liquid form, burr hole aspiration is sufficient to remove it; but, as the condition progresses to thick pus, craniotomy is required to remove the greater amount of contaminated material [5]. The recurrence rate has been found more in the burr-hole surgery than craniotomy [11].
In the presence of subdural hematomas, spontaneous subdural empyema is extremely uncommon. To the best of our knowledge, this is the rare instance of spontaneous subdural hematomas reported in the literature. Subdural empyema is linked to a high rate of mortality if left undiagnosed and morbidity because complications can lead to live with deficits. Early diagnosis and therapy, more precise localization of empyema by imaging techniques, early sinus drainage, and identification of the significant contribution of anaerobes to the disease have all helped to lower the mortality rate in SDE. Physicians should be aware of this uncommon but probable consequence of chronic subdural hematomas for a timely diagnosis.
The authors declare no conflict of interest.

