 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Imran Qureshi1*, Hamed Sultan Albusaidi Hamed1, Parmanand Nathani1, Fatema Mohammed Khamis Al Sadairi1, Sanobar Bughio2
1Department of Radiology, Royal Oman Police Hospital, Muscat, Oman.
2Department of Radiology, Dr Ziauddin Hospital, Karachi, Pakistan.
Correspondence to: Imran Qureshi, Department of Radiology, Royal Oman Police Hospital, Muscat, Oman.
Received date: November 19, 2023; Accepted date: November 30, 2023; Published date: December 07, 2023
Citation: Qureshi I, Hamed HSA, Nathani P, et al. Solitary Osteochondroma of Scapula: A Common Entity at an Uncommon Location. J Med Res Surg. 2023;4(6):115-117. doi: 10.52916/jmrs234122
Copyright: ©2023 Qureshi I, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted
use, distribution and reproduction in any medium, provided the original author and source are credited.
Introduction: Introduction: Osteochondroma are benign bone tumours that often affect the metaphysical region of long bones; the scapula is rarely affected. Owing to its bulk effect, scapular osteochondroma may frequently present with symptoms. These tumours typically damage the skeleton's developing ends and stop becoming larger once the skeleton reaches maturity.Suspicion of a cancer should be raised by any increase in size.
Case Report: A female patient, age 25, complained of a hard lump on her shoulder posteriorly on further imaging it was confirmed as an osteochondroma of scapula.
Discussion: Osteochondromas must exhibit continuity with the underlying parent bone cortex and medullary canal. They are made up of cortical and medullary bone with an overlaying hyaline cartilage cap. They have a very minimal potential for malignancy and are often asymptomatic.
Conclusion: The cases of osteochondromas in the scapula are relatively rare, it is crucial to remain vigilant and consider the possibility of malignancy if there are concerning changes in symptoms or size.
Osteochondroma, Scapula, Bony tumor, Outgrowth, Endochondral, Ossification.
Osteochondromas are benign bone tumors that most commonly occur in the metaphyseal region of long bones, such as the femur or tibia. However, they can also occasionally affect other bones, including the scapula.When osteochondromas develop in the scapula, they can often cause symptoms due to their mass effect on the surrounding tissues. These symptoms may include pain, limited range of motion, or even nerve compression if the tumor grows in close proximity to nerves [1,2]. It is important to note that while osteochondromas are generally benign, any increase in swelling or changes in symptoms should raise a level of suspicion for malignancy. It is interesting to mention that osteochondromas predominantly affect the growing ends of the skeleton, commonly during childhood or adolescence. As an individual reaches skeletal maturity, the growth of these tumors typically ceases [3]. However, in some cases, osteochondromas can continue to grow even after skeletal maturity. When evaluating a scapular osteochondroma, imaging studies such as X-rays, CT scan or MRI scans are commonly used to assess the size, location, and integrity of the tumor [4]. These studies help determine the best course of action, whether it be close monitoring, surgical removal, or further investigation if malignancy is suspected.While cases of osteochondromas in the scapula are relatively rare compared to other locations, it is crucial for healthcare providers to remain vigilant and consider the possibility of malignancy if there are concerning changes in symptoms or size. Timely diagnosis and appropriate management are essential for ensuring the best possible outcomes for patients.
This case report presents a 25-year-old female who presented in the OPD with complained of a hard lump on her posterior shoulder, accompanied by nonspecific pain in the shoulder and neck for at least one year. The patient denied any history of weight loss, trauma, loss of appetite, or other constitutional symptoms. Additionally, there was no family history of similar complaints. Physical examination revealed no other swelling in the body, except for a non-mobile, painless, hard lump located on the body of the right scapula dorsally, which moved with the scapula. Her plain radiograph of chest Figure 1 shows a single elongated bony outgrowth which was seen projecting on medial margin of the scapula and extending superiroly most likely orginating from medial border of right scapula. There was no fracture seen. To further investigate this intriguing finding, we decided to conduct a Computed Tomography (CT) scan Figure 2 and Figure 3 which confirmed our initial observations the continuous medullary cavity further highlighted the cohesion between the two structures which is key feature of osteochondroma.
 Figure 1: X-Ray (PA view) chest shows bony out growth from medial border of right scapula.
Figure 1: X-Ray (PA view) chest shows bony out growth from medial border of right scapula.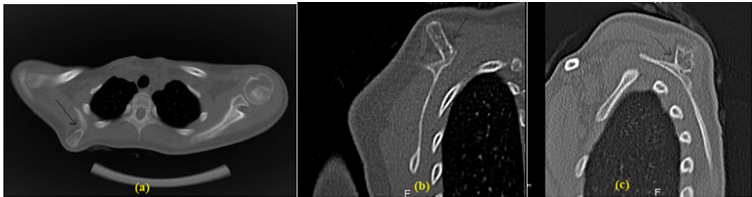 Figure 2: CT scan shows lesion originating from medial portion of the scapula and extending superiroly, having continuous medullary cavity with the parent bone.
Figure 2: CT scan shows lesion originating from medial portion of the scapula and extending superiroly, having continuous medullary cavity with the parent bone.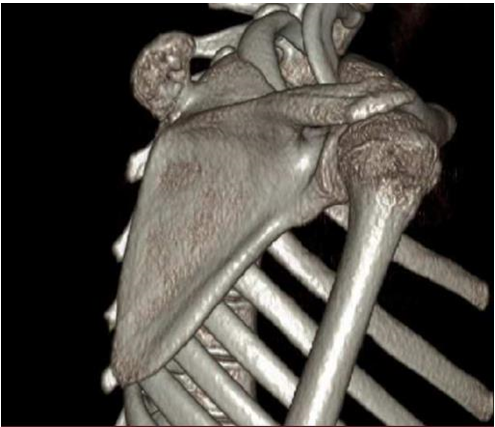 Figure 3: 3D image of bony outgrowth from superior medial portion of the scapula with preserved cortical continuity.
Figure 3: 3D image of bony outgrowth from superior medial portion of the scapula with preserved cortical continuity.Osteochondroma is a condition that occurs when trapped growth plate cartilage herniates through the cortex and grows beneath the periosteum via endochondral ossification [1]. It is characterized by the presence of cortical and medullary bone with a hyaline cartilage cap, which must demonstrate continuity with the underlying parent bone cortex and medullary canal. Osteochondromas are typically asymptomatic and have a very low likelihood of becoming malignant. However, if malignant transformation does occur, it is usually within the cartilage cap. Osteochondromas can be either single or multiple [1,2].
The most common symptom of osteochondroma is a nontender, painless cosmetic deformity caused by the slow enlargement of the exophytic mass. Complications associated with osteochondromas include deformity, fracture, vascular and nerve compromise, bursitis, and malignant transformation [2,3]. Rarely reported complications include osteomyelitis, infarction of the cartilage cap or osseous component, muscle impingement, and hemarthrosis [3].
Osteochondromas commonly arise from the appendicular skeleton, particularly around the knee. The most common locations include the distal femur, proximal tibia, proximal femur, and proximal humerus [4]. However, osteochondroma can occur in any bone where endochondral ossification takes place. The growth of osteochondroma parallels the growth of the patient and will cease once the physis closes [4,5].
There are two main types of osteochondroma: sessile and pedunculated. Sessile osteochondromas have a wider base and are associated with a higher risk of malignancy. On the other hand, pedunculated osteochondromas have a narrow stalk and typically grow away from the joint [2].
Radiographic findings of osteochondroma include bony outgrowth, which can be either sessile or pedunculated, typically seen in the metaphyseal region, away from the epiphysis [3,4]. The osteochondroma also contains a variable cartilage cap, which can appear thin or thick with rings and arcs of calcifications. Additionally, new cortical irregularity or continued growth after skeletal maturity, as well as aggressive features, may be present [5,6].
The cases of osteochondromas in the scapula are relatively uncommon compared to other areas, it is of utmost importance for healthcare providers to maintain a vigilant approach and consider the potential for malignancy if there are any worrisome changes in symptoms or size. Timely diagnosis and appropriate management are absolutely crucial in order to ensure the best possible outcomes for patients.
The authors have no conflicts of interest to report.
No.

