 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Maroua Rhaouti1*, F Lamouime1, I Arramach1, M Lakranbi1,2, Y Ouadnouni1,2, M Smahi1,2
1Department of Thoracic Surgey, University Hospital Fes, Morocco.
2Sidi Mohamed Ben Abdellah University, Faculty of Medicine (Fes), Morocco.
Correspondence to: Maroua Raouti, Department of Thoracic Surgey, University Hospital Fes, Morocco.
Received date: October 10, 2023; Accepted date: October 24, 2023; Published date: October 31, 2023
Citation: Rhaouti M, Lamouime F, Arramach I, et al. Should There be a Surgical Revision of the Axillary Incisions Prior to a Nuss Bar Extraction?. J Med Res Surg. 2023;4(5):106-107. doi: 10.52916/jmrs234119
Copyright: ©2023 Rhaouti M, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted
use, distribution and reproduction in any medium, provided the original author and source are credited.
The minimally invasive Nuss procedure is currently the preferred surgical approach for treatment of pectus excavatum. During this procedure, a retrosternal bar is inserted which instantly corrects the deformity. The bar typically remains in place for 2 to 3 years, during which time the chest is considered to have adopted its new shape. Removal of the bar is generally considered to be a nondemanding procedure. Notwithstanding, it is associated with rare but potentially life-threatening complications.
Pectus excavatum, Nuss procedure, Bar removal, Complications.
The removal of pectus bars marks the final crucial step in the minimally invasive correction of pectus excavatum. However, in this case report, we intend to shed light on a vital aspect of this process.
The surgical revision of the two axillary incisions that precede the Nuss bars' removal. This surgical revision, often overlooked, plays a pivotal role in ensuring a successful outcome for patients undergoing this procedure. Through this report, we aim to emphasize the significance of this meticulous revision process and its impact on the overall success of pectus bar removal surgery.
We present a 21-year-old male who underwent a Nuss procedure with the positioning of two parallel bars for a pectus excavatum three years ago with satisfactory clinical outcomes, currently admitted for removal of the two bars.
Anteroposterior and lateral chest X-rays showed the position of the two parallel bars with no radiological sign of migration (Figure 1).
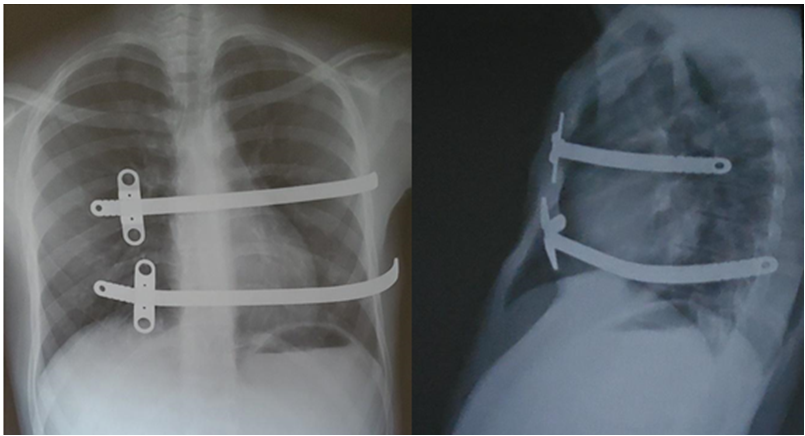 Figure 1: Anteroposterior and lateral chest x-rays showing the two parallel bars with no signs of migration.
Figure 1: Anteroposterior and lateral chest x-rays showing the two parallel bars with no signs of migration.Ablation of the two bars was performed following revision of the 2 axillary incisions. During the procedure, we noted that the inferior bar as well as its stabilizer had perforated the intercostal space and were in contact with the diaphragm. The removal of the bars was done after the upswing of the two bars curvatures (Figure 2).
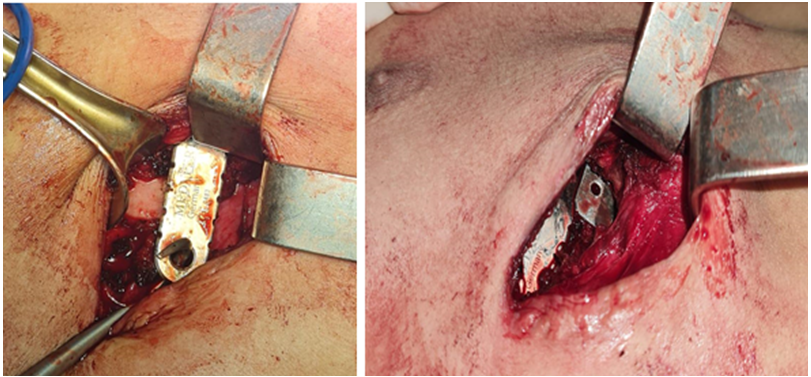 Figure 2: The inferior implant and its stabilizer perforating the intercostal space.
Figure 2: The inferior implant and its stabilizer perforating the intercostal space.The Nuss procedure, a minimally invasive surgical technique for correcting chest wall deformities, has garnered significant attention in the field of thoracic surgery. Its unique approach offers an optimal correction of chest wall defects while minimizing scarring and avoiding the need for cartilaginous resection. This innovative procedure has proven to be a game-changer for individuals dealing with conditions like pectus excavatum.
The bar ablation is conducted under general anesthesia and relies on using the previous incision sites on both sides to mobilize and adjust the bars before removing them [1].
The use of metallic bars inserted endoscopically behind the sternum is a hallmark of the Nuss procedure. This approach allows for precise placement of one or more bars, effectively restoring the anatomical shape of the growing thorax. Endoscopic techniques offer surgeons direct visualization of the surgical site [2-4], enhancing accuracy and reducing the risk of errors during placement.
The removal of the implanted bars, an essential step in the process, demands a high level of skill and precision. The text rightly emphasizes the necessity of conducting bar ablation in specialized medical centers equipped with the necessary tools and personnel, including cardiac surgeons. The removal process can be intricate and carries the risk of damaging surrounding anatomical structures, highlighting the importance of specialized care.
This procedure is not without risks. Eventual complications of this surgery include: pneumothorax, pleural effusion, infection, shifting (and/or breaking of the bars), recurrence of pectus excavatum and more importantly, potentially mortal hemorrhaging. The prevalence of these complications is further increased in complex cases of pectus excavatum for which the corrective surgery requires multiple bars [5].
Some authors suggest removal of the implanted bars after the revision of only one axillary incision. However, we deem such practice [6], as do several studies, quite dangerous. Removing the bar with a folded extremity can skewer different sources of hemorrhagia (intercostal or internal mammary artery pedicle, lung, diaphragm and in some cases the heart).
Our case perfectly illustrates this risk, as neither anteroposterior nor profile chest X-rays could show the ruptured intercostal space, and even without such rupture, one extremity of the bar could still skewer different anatomical structures and organs on its removal trajectory.
The reconsideration of old axillary incisions assumes paramount importance. This approach is particularly relevant when assessing the potential risks associated with the removal of the Nuss bars. During scheduled bar extraction, it becomes apparent that the trajectory of the bar's end, upon removal, may intersect with various adjacent anatomical structures and organs, potentially leading to unintended complications. By revising and optimizing the axillary incisions in advance of the removal procedure, surgical teams can strategically mitigate these risks. This pre-emptive measure aims to ensure that the incisions are precisely positioned, allowing for safer and more controlled bar removal. Moreover, it provides an opportunity to assess the condition of the incisions and address any unforeseen changes or adhesions that may have occurred since the initial surgery. While introducing an additional surgical step, this approach is rooted in the principle of proactive risk management and can significantly enhance the overall safety and precision of scheduled Nuss bar removal for deformity correction.
We henceforth recommend that the ablation of Nuss bars be conducted in a specialized medical center with adequate tools and trained personnel including cardiac surgeons available. Should postoperative outcomes be satisfactory, the patient can be discharged on the same day.
The minimally invasive surgery of chest wall defects, including post-correction bar removal has to adhere to strict management and surveillance protocols. The bilateral revision of the axillary incisions is considered to be a fundamental pillar of these protocols to reduce morbimortality and optimize postoperative rehabilitation.
The authors have no conflicts of interest to report.
No

