 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Correspondence to: Loveline R. Pallera, Department of General Surgery, Manila Doctors Hospital, 1000 Metro Manila, Philippines; E-mail: luvlynshaw@yahoo.com
Received date: January 8, 2020; Accepted date: January 15, 2020; Published date: January 22, 2020
Citation: Pallera LR, Salvador RC (2020) Safety of Laparoscopic Surgery in Elderly Population in Manila Doctors Hospital, 2016-2018. J Med Res Surg 1(1): pp. 1-6.
Copyright: © 2020 Pallera M, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited
This study is intended to assess the safety of Laparoscopic surgery in the elderly aged 60 years and older in terms of mortality and morbidity in Manila Doctors Hospital. Since elderly patients are more prone to complications due to the body’s physiological changes and comorbidities.
From January 2016 to December 31, 2018, all patients aged 60 years and above who underwent Laparoscopic Cholecystectomy, Laparoscopic Appendectomy and Laparoscopic Hernia Repair were included in the study. Physiologic and operative scores using P-POSSUM and estimates of patient-specific postoperative complications after the surgical procedure using ACS NSQIP risk scoring were used. The overall morbidity and mortality outcome was compared with a choice of international studies.
A total of 273 elderly patients underwent laparoscopic surgery. Mostly, 53.1% of the population were 60 to 64 years old who underwent cholecystectomy procedure. The study showed that laparoscopic procedures were safe in the elderly patient despite the challenge that the older population has decreased physiologic reserved and with multiple comorbidities. Among 273 elderly patients, only 3 patients had complications. 2 or 0.74% had pneumonia and 1 or 0.36% died.
Laparoscopic surgery; Cancer; Mortality; Morbidity
Laparoscopic surgery is a widely accepted procedure nowadays that uses small incisions and video-assistance. As the incision is smaller than the open cholecystectomy procedure, it leads to a shorter hospital stay, less postoperative pain or discomfort, quicker recovery, earlier return to full activities and smaller scar [1]. In experienced hands, laparoscopic surgery has comparable morbidity and mortality outcomes to open procedures. Moreover, in properly selected individuals, some early cancers have equivalent oncologic outcomes for both open and laparoscopic procedures.
An increasing number of elderly patients are undergoing a variety of surgical procedures. Physiologically, aging is associated with gradual loss of reserve capacity even in individuals without obvious underlying comorbidities and prior surgical procedures [2]. The risk of mortality and morbidity in geriatrics is higher compared to a younger age after elective or emergency procedure due to the physiologic changes in the elderly. Laparoscopic procedures may be particularly challenging given the associated risks with general anesthesia and pneumoperitoneum [3].
Several published studies, however, show the comparability of mortality and morbidity outcomes following open and laparoscopic surgery, with some studies even demonstrating superior outcomes in the latter, due to minimization of surgical trauma and stress [4]. To the authors’ knowledge, there is no published local reports on mortality and morbidity outcomes following laparoscopic procedures specific to the elderly population. Hence, this study aims to investigate the general safety of laparoscopic procedures in patients 60 years old and above in terms of 30-day morbidity and mortality rates and length of hospital stay in Manila Doctors’ Hospital (MDH). The study is unique in that patients will be stratified according to specific laparoscopic procedure done and will include assessment of the patients’ surgical risks using the portsmouth predictor equation for mortality Physiological and Operative Severity Score for the Enumeration of mortality and morbidity (P-POSSUM) and American College of Surgeons’ National Surgical Quality Improvement Program Surgical Risk Scores (ACS NSQIP). Data obtained will serve as a quality indicator for the MDH Department of Surgery and will aid in patient selection for improved outcomes for laparoscopic surgeries.
To assess the safety of laparoscopic surgical approaches for emergency and elective procedures among elderly patients ( ≥ 60 years old) in MDH.
To assess the safety of laparoscopic surgical approaches for emergency and elective procedures among elderly patients ( > 60 years old) in MDH.
The study is an observational, descriptive, prospective study. It was conducted in Manila Doctors Hospital from January 1, 2016, to December 31, 2018.
All patients aged 60 years and older who will undergo laparoscopic surgery in Manila Doctors’ Hospital (private and service cases) January 1, 2016, to December 31, 2018, will be included in the study and will constitute the main study population.
Patients who only underwent diagnostic laparoscopy or those who were converted from initially laparoscopic to open surgery will be excluded.
From January 1, 2016, to December 31, 2018, all patients (private and service) aged 60 and above operated initially by laparoscopy will be included in our study. Data relating to age, gender, smoking, functional status (ECOG), American Society of Anaesthesiologist (ASA) Score, co-morbidities such as hypertension, diabetes, Coronary artery disease, COPD, Tuberculosis, Chronic Kidney Disease, Cirrhosis, and others, BMI, previous abdominal or pelvic surgery, receipt of neo-adjuvant chemotherapy, radiotherapy or both for malignant cases, diagnosis whether benign or malignant, elective vs. emergency surgery, type of surgery, operative time, intraoperative blood loss. The surgical risk will be assessed for each patient using the P-POSSUM score (Table 1) and ACS NSQIP Surgical Risk Score [22-23]. Patients were prospectively followed for data on post-operative length of hospital stay, 30- day morbidity and mortality rates. For private patients, consent will be obtained from surgeons for access to follow up data of patients until 30 days post-operatively. Patients were grouped and analysed overall and according to laparoscopic procedures grouped according to treated pathology as follows: Group 1 consisted of all interventions performed in the biliary tree; group 2 all interventions performed in the appendix and group 3 consisted of hernia surgery.
Prospective data entered into a database of all patients who underwent laparoscopic surgery in MDH from 2016-2018. Data were presented as means with standard deviations for continuous variables and frequency or percentages for categorical variables. Data were compared to the international study according to the safety of the procedure.
A total of 273 patient records were included in this study from 2016 to 2018. The majority of patients were 60-64 years old (53.1%) and almost half were females (53.8%). The majority of patients were also non-smokers (86.1%). Most were ASA II (70.7%) and ECOG 0 (57.9%). Also, a majority of patients have normal BMI (96.7%). Table 1 shows the characteristics of elderly patients who underwent Laparoscopic surgery in Manila Doctors hospital, 2016-2018 (Table 1 and 2).
Table 1: Clinical profile of patients who underwent laparoscopic procedures in Manila Doctors Hospital from 2016-2018.| Number of Patients=273 | |
| Age in years | |
| 60-64 | 145 (53.1%) |
| 65-74 | 103 (37.7%) |
| 75-84 | 24 (8.8%) |
| >85 | 1 (0.4%) |
| Sex | |
| M | 126 (46.2%) |
| F | 147 (53.8%) |
| Smoking | |
| Y | 38 (13.9%) |
| N | 235 (86.1%) |
| ASA | |
| I | 28 (10.3%) |
| II | 193 (70.7%) |
| III | 52 (19.0%) |
| IV | 0 (0.0%) |
| ECOG | |
| 0 | 158 (57.9%) |
| 1 | 57 (20.9%) |
| 2 | 58 (21.2%) |
| 3 | 0 (0.0%) |
| 4 | 0 (0.0%) |
| BMI | |
| Underweight | 3 (1.1%) |
| Normal | 264 (96.7%) |
| Overweight | 5 (1.8%) |
| Obese | 1 (0.4%) |
| Diagnosis | |
| Cholecystitis | 260 (95.2%) |
| Appendicitis | 9 (3.3%) |
| Inguinal hernia | 4 (1.5%) |
| Operative time, hours | |
| 01-Feb | 81 (29.7%) |
| >2-3 | 176 (64.5%) |
| >3 | 16 (5.9%) |
| Operative blood loss, ml | |
| < 100 | 273 (100.0%) |
| >100-500 | 0 (0.0%) |
| >500 | 0 (0.0%) |
Postoperative outcomes showed that laparoscopic procedures among the elderly were safe (Table 3). The median postoperative length of stay was only 2 days, which ranged between 1 to 4 days. Only 2 patients had morbidity that underwent laparoscopic cholecystectomy (0.74%) and only 1 patient died (0.36%) (Figure 1-3). In terms of surgical risk using POSSUM scores, the mean POSSUM morbidity scores are as follows: 20.0 ± 4.7 for group 1, 14.2 ± 2.3 for group 2, 16.5 ± 3.6 for group 3, and 19.8 ± 4.5 for all groups.
 Figure 1: Percentage of Laparoscopic procedures by group done in
Manila Doctors hospital from January 2016- December 2018.
Figure 1: Percentage of Laparoscopic procedures by group done in
Manila Doctors hospital from January 2016- December 2018. Figure 2: Average Surgical Risks in >60 stratified according to Laparoscopic Procedures using POSSUM in Manila Doctors Hospital, 2016-2018
Figure 2: Average Surgical Risks in >60 stratified according to Laparoscopic Procedures using POSSUM in Manila Doctors Hospital, 2016-2018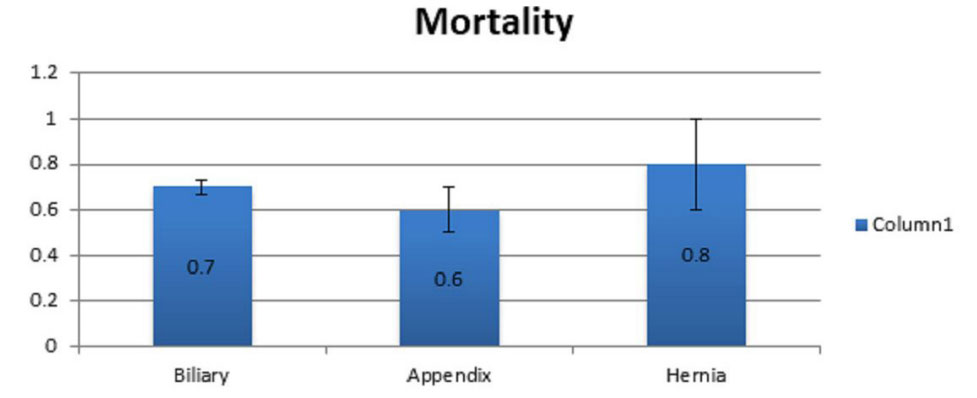 Figure 3: Average Surgical Risks in >60 stratified according to Laparoscopic Procedures using POSSUM in Manila Doctors Hospital, 2016-2018./span>
Figure 3: Average Surgical Risks in >60 stratified according to Laparoscopic Procedures using POSSUM in Manila Doctors Hospital, 2016-2018./span>| No adjustment necessary N=226, 82.8% | Risk somewhat higher than expected N=47, 17.2% | |
|---|---|---|
| Group 1: Biliary | 214 (82.3%) | 46 (17.7%) |
| Group 2: Appendix | 8 (88.9%) | 1 (11.1%) |
| Group 3: Hernia | 4 (100.0%) | 0 (0.0%) |
| Postoperative length of hospital stay (days) (Median, Range) | |
| Group 1: Biliary | 2 (1-4) |
| Group 2: Appendix | 2 (1-4) |
| Group 3: Hernia | 2 (1-2) |
| All | 2 (1-4) |
| Morbidity Rate (n,%) | |
| Group 1: Biliary | 2 (0.74%) |
| Group 2: Appendix | 0 (0.0%) |
| Group 3: Hernia | 0 (0.0%) |
| All | 2 (0.74%) |
| Mortality Rate (n,%) | |
| Group 1: Biliary | 1 (0.36%) |
| Group 2: Appendix | 0 (0.0%) |
| Group 3: Hernia | 0 (0.0% |
| All | 1 (0.36%) |
This table showed that out of 273 patients who underwent laparoscopic procedure only 3 patients had complications, 2 or (0.82%) had morbidity and 1 or 0.41% died and all were under the elective procedure (Table 4 and 5).
| N= 273 | Group 1 | Group 2 | Group 3 |
|---|---|---|---|
| Morbidity | |||
| Pneumonia | 2(0.74%) | 0 | 0 |
| Surgical site infection | 4 (100.0%) | 0 | 0 |
| CBD Injury | 0 | 0 | 0 |
| Myocardial Infarction | 0 | 0 | 0 |
| Pulmonary Embolism | 0 | 0 | 0 |
| Urinary Tract infection | 0 | 0 | 0 |
| Mortality | |||
| Sepsis | 0 | 0 | 0 |
| Myocardial Infarction | 1 (0.36%) | 0 | 0 |
| N=273(%) | Emergency | Elective | Total |
|---|---|---|---|
| Group 1 | 16(6.2%) | 244 (93.8%) | 260 (100%) |
| Morbidity | 0 | 2 (0.82) | 2 |
| Mortality | 0 | 1 (0.41) | 1 |
| Group 2 | 4 (44.4%) | 5 (55.6%) | 9 (100%) |
| Morbidity | 0 | 0 | 0 |
| Mortality | 0 | 0 | 0 |
| Group 3 | 0 | 4 (100%) | 4 (100%) |
| Morbidity | 0 | 0 | 0 |
| Mortality | 0 | 0 | 0 |
| Values in parentheses are percentage Group 1=Biliary surgery; Group 2=Appendix surgery; Group 3= Hernia surgery | |||
Due to the improving levels of the primary prevention and advancement of medical care, people’s life expectancy has also increased. The World Health Organization (WHO) has defined elderly people aged more than 60 years. Hence, this study used 60 years old and above as the cut off age of the elderly. These elderly patients are more susceptible to adverse surgical outcomes because of the associated co-morbidities and decreased functional reserve
I have used P-POSSUM in the study to better quantify and assess the risk of morbidity and mortality of the elderly patients who underwent laparoscopic surgery and ACS- NSQIP to estimate the possible post-operative risk in developing complication after the operation.
The overall results of this single-centre study consisting of 273 laparoscopic interventions on patients aged 60 years old and above with an ASA 2 of 70.7% of a total population and an ECOG 0 (zero) with 57.9% and mostly under elective operation during the time period of 3 years confirms the safety of laparoscopic approach in elderly. Among 273 patients, we had 2 or 0.77% morbidity cases in a biliary group and the observed cause was Pneumonia and for Mortality, 1 or 0.38% died due to myocardial infarction post-operatively under biliary group.
This study supports that laparoscopic surgery is indeed safe for the elderly population with the study done by Cuelemans et al, in Strasbourg, France. A single-centered study with 166 laparoscopic interventions of patients 75 years and older for a time period of 18 months. Physiologic and operative scores according to the POSSUM scoring system were used and mortality and morbidity by both POSSUM and P-POSSUM to compute the predicted outcome. They observed that they can do a laparoscopic procedure even in patients with ASA 3 and 4, in emergency and elective cases and their overall morbidity was 14.5% and mortality of 1.8%.
Another study made by Bhandari et al in Nepal, wherein, they compared the safety of laparoscopic surgery in elderly aged 60 years and above from those patients below 60 years old. From July 2015 to July 2016, they had 78 elderly and 164 young patients. They observed that there is no significant difference rate for elderly and young patients (17.9 and 14.6% P=0.508). The complications among the elderly were lower respiratory tract infection and superficial thrombophlebitis in the young.
In conclusion, this study describing the data observed in the patient population aged 60 years and older, included 70.7% of ASA 2 and 19.0% of ASA 3 and 21 or 7.7% of emergency cases, reports and overall morbidity of 0.74% and mortality rate of 0.37%. In this study, there was no noted morbidity and mortality in emergency cases. The 2 morbidity cases are under the elective procedure and aged 65 to 74, while the mortality patient who had Myocardial Infarction was also under the elective procedure and 84 years old. Using the P-POSSUM scores the patient population seemed to benefit from the laparoscopic approach, showing significantly lower morbidity and mortality rate predicted. The surgical risk using ACS NSQIP showed that the majority of the patient needed no adjustment prior to the surgery. It showed that the elderly patients have below to average chance of developing serious complications post-operatively. Therefore, we recommend a laparoscopic approach to be used in the elderly population in elective as well as emergency cases with ASA 2 and 3 classifications in our daily practice.
A potential bias in this study is that using the P-POSSUM scores may over predict the mortality and morbidity rate. Most of the patients in this study are under biliary surgery and elective procedure hence we cannot really define the risk of mortality and morbidity on an emergency basis.
I would recommend for the future researchers, to make a onger timeline to get more subject population for both elective and emergency laparoscopic procedure and to include laparoscopic colon resection.

