 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Maktum Naik1 , Vageesh BG2*, Naveen Kumar CH2, Anil Agarwal3
, Vageesh BG2*, Naveen Kumar CH2, Anil Agarwal3
1Senior Resident, Department of Gastrointestinal Surgery, Govind Ballabh Pant Institute of Medical Education and Research, New Delhi, India.
2Assistant Professor, Department of Gastrointestinal Surgery, Govind Ballabh Pant Institute of Medical Education and Research, New Delhi, India.
3Professor, Department of Gastrointestinal Surgery, Govind Ballabh Pant Institute of Medical Education and Research, New Delhi, India.
Correspondence to: Vageesh BG, Assistant Professor, Department of Gastrointestinal Surgery, Govind Ballabh Pant Institute of Medical Education and Research, New Delhi, India.
Received date: December 13, 2024; Accepted date: December 22, 2024; Published date: December 29, 2024
Citation: Naik M, Vageesh BG, Naveen Kumar CH, et al. Retroperitoneal Tumors: Insight Gained Over a Decade in a Single Surgical Unit. J Med Res Surg. 2024;5(6):130-135. doi: 10.52916/jmrs244152
Copyright: ©2024 Naik M, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Background: Retroperitoneal tumors (RPTs) are uncommon but varied types of neoplasms, representing 0.1-0.2% of all cancers. They can range from benign to being highly malignant. A significant portion of RPTs are malignant (70–80%), with the majority being sarcomas. Roughly 20% of these tumors are benign, and most retroperitoneal tumors tend to be quite large by the time they are detected. The management of these tumors poses challenges due to their size, intricate anatomy, and their closeness to vital organs and blood vessels. This study intends to share our experiences in dealing with retroperitoneal neoplasms and to provide a detailed understanding of their clinical presentation, surgical management, and outcomes. Methods: A total of 54 patients diagnosed with retroperitoneal tumors were treated in a single gastrointestinal surgery unit from January 2010 to December 2023. We retrospectively analysed the prospectively maintained data of these patients. Results: The median age of the patients was 50 years, with an age range of 15 to 86 years. The ratio of males to females was 33:21. The most frequently reported symptom was abdominal pain, observed in 33 instances (61.2%). The average size of the tumors measured 17.3 cm in diameter, with a range from 7.0 to 36.0 cm. 46 patients (85.1%) underwent surgical resection. Complete resection (R0 resection) was achieved in 41 patients (75.9%). Five patients (9.2%) received debulking procedures for surgical palliation, while eight patients (14.9%) were considered for palliative chemotherapy. Additionally, nine cases (16.6%) necessitated the resection of adjacent organs.The median duration of the surgical procedure was 210 minutes (60-310 minutes). Postoperatively, the median length of hospital stay was 7 days (2 to 37 days). The median follow-up period lasted 62 months (3 to 102 months). Recurrences were noted in 5 patients (9.2%). Median overall survival duration of the patients with malignancy was 58.5 months (12-130 months). Overall suvival was highest for patients with liposarcoma and grade 1 tumors. Conclusion: RPTs are challenging to manage because of their location, locally advanced nature, and heterogeneous pathology. Preoperative imaging is essential for adequate surgical planning. Complete surgical resection is the cornerstone of RPT management and has the potential for curative treatment. Survival rates are better for liposarcoma and Grade I tumors. Given the infrequency of RPTs, there is a necessity for more collaborative research to more precisely determine the best approach to treating these tumors, including the use of perioperative chemoradiotherapy.
Retroperitoneal tumors, RPTs, Leiomyosarcoma, Liposarcoma, Surgical management.
Retroperitoneal Tumors (RPTs) are quite uncommon, representing 0.1-0.2% of all cancer cases. These tumors can vary from benign to highly malignant forms. They originate from different types of soft tissues located in the retroperitoneal area, including fat, muscle, fibrous tissue, lymph nodes, and bone [1]. The retroperitoneum is the space bound anteriorly by the posterior parietal peritoneum and posteriorly by the transversalis fascia, extending from the diaphragm at the top down to the pelvic brim at the bottom [2]. A significant portion of retroperitoneal tumors are malignant (70-80%), with most classified as sarcomas [3]. Approximately 20% of these tumors are benign [4], and many retroperitoneal tumors tend to be large by the time they are detected. Treating these tumors is difficult due to their size, intricate anatomy, and closeness to essential organs and blood vessels. Nevertheless, surgery remains the preferred treatment for RPTs, which has a notable impact on post-operative survival [5]. This study seeks to share our insights gained from managing retroperitoneal neoplasms and offer a thorough understanding of their clinical features, surgical treatment options, and survival rates, taking into account their varied pathologies.
This study is a Retrospective analysis of prospectively maintained data from a single Gastrointestinal surgical unit of a tertiary care institute. From January 2010 to December 2023, a total of 54 cases of retroperitoneal tumors managed in our unit were identified. 46 patients (85.1%) managed surgically. 41 cases (75.9%) underwent complete surgical resection (R0), and five patients (9.2%) underwent only debulking surgery. Eight patients (14.9%) had unresectable tumors on imaging and were considered for palliative chemotherapy. Data was collected regarding patient demographics, clinical presentation, tumor characteristics, radiological reports, operative details, perioperative outcome, hospital course, histopathology, and survival outcomes.
Categorical data were expressed as numbers (percentages), and continuous data were expressed as Mean (SD) if it is normal distribution and median (range) if it is non normal distribution. Statistical test was performed using the Microsoft excel for Windows v10.
From January 2010 to December 2023, a total of 54 cases of Retroperitoneal Tumors (RPTs) managed in our unit were analyzed (Table 1). Among these 54 patients, 33 were male and 21 were female. The median age of the patients was 50 years, with a range of 15 to 86 years. The main presenting complaint was abdominal pain in 33 patients (61.2%), followed by abdominal mass in 17 patients (31.4%), fever in 2 patients (3.7%), and incidental detection in 2 patients (3.7%).
Table 1: Characteristics of the patients and tumors.|
Characteristics (n=54) |
Value |
|
Age |
|
|
Male |
47 (15 to 86) |
|
Female |
53 (28 to 58) |
|
Gender |
|
|
Male |
33 (61.1%) |
|
Female |
21 (38.9%) |
|
BMI |
|
|
>25 |
35 (64.8%) |
|
<25 |
19 (35.2%) |
|
Tumor size |
|
|
≤ 10 cm |
21 (38.9%) |
|
11 to 20 cm |
20 (37.0%) |
|
>20 cm |
13 (24.1%) |
|
Grade of Tumors (n=39) |
|
|
Grade I |
13 (33.3%) |
|
Grade II |
16 (41.1%) |
|
Grade III |
10 (25.6%) |
|
Nodal Disease (n=39) |
|
|
No |
33 (84.6%) |
|
N1 |
06 ( 15.4%) |
|
Surgical management |
46/54 (85.1%) |
|
Complete resection (R0) |
41 (75.9%) |
|
Debulking surgery (R2) |
5 (9.2%) |
|
Unresectable |
8 (14.9%) |
|
Additional organ resection |
9 (16.6%) |
|
Nephrectomy |
3 |
|
Colectomy |
2 |
|
Splenectomy |
1 |
|
Distal pancreaticosplenectomy |
1 |
|
Small intestine |
1 |
|
Gastric wedge |
1 |
Out of the 54 patients, 46 underwent surgical management. Of these, 41 patients (75.9%) had complete resection (R0 resection), while five patients (9.2%) underwent debulking as a form of surgical palliation. Eight patients (14.9%) were considered for palliative chemotherapy due to distant metastasis. To ensure a complete and safe resection, preoperative bilateral ureteral stenting was performed in 11 cases. Nine cases (16.6%) required resection of adjacent organs, including left nephrectomy in three cases, colectomy in two cases, splenectomy, distal pancreatosplenectomy, small intestine resection, and gastric wedge resection each in one case.
The median operative time was 210 minutes, with a range of 60 to 310 minutes. Eighteen patients received adjuvant treatment. Postoperatively, ten patients (18.5%) experienced complications classified as Clavien-Dindo grade I/II. Five patients had surgical site infections, three patients developed fever due to minor fluid collections at the operative site, which was managed conservatively with intravenous antibiotics, and two patients experienced prolonged postoperative ileus, which was managed conservatively.
Pathologically, 39 patients (72.2%) had malignant etiologies, while 15 patients (27.8%) had benign etiologies. In the malignant group, the diagnoses included 16 cases of liposarcoma, 10 cases of leiomyosarcoma, five cases of malignant fibrous histiocytoma, four cases of non-Hodgkin lymphoma, three cases of fibrosarcoma, and one case of malignant paraganglioma (Figure 1). In the benign group, there were seven cases of lipoma, two cases of dermoid cyst, two cases of fibroma, and one case each of benign paraganglioma, schwannoma, neurofibroma, and mesothelial cyst (Table 2). The median tumor diameter was 17.3 cm, with a range of 7.0 to 36.0 cm. In terms of pathological grading, there were 13 cases with Grade I, 16 cases with Grade II, and 10 cases with Grade III disease, with five patients undergoing R2 resection.
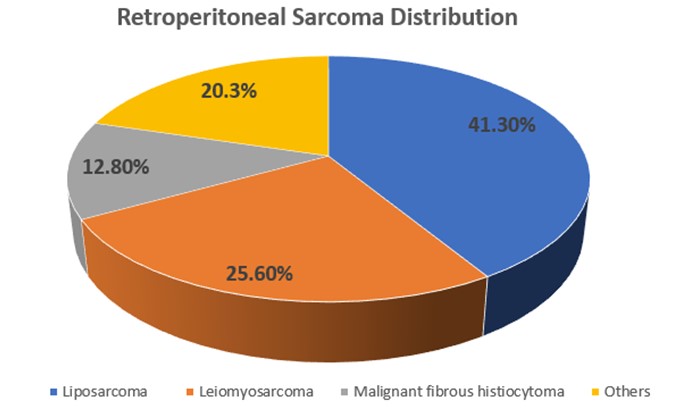 Figure 1: Distribution of malignant RPTs.
Figure 1: Distribution of malignant RPTs.|
Tissue type |
Number (%) |
|
Malignant (n=39) |
72.20% |
|
Liposarcoma |
16(41.3%) |
|
Leiomyosarcoma |
10(25.6%) |
|
Malignant fibrous histiocytoma |
5(12.8%) |
|
Non-Hodgkins lymphoma |
4(10.2%) |
|
Fibrosarcoma |
3(7.6%) |
|
Malignant paraganglioma |
1(2.5%) |
|
Benign (n=15) |
27.80% |
|
Lipoma |
7(46.6%) |
|
Dermoid cyst |
2(13.3%) |
|
Fibroma |
2(13.3%) |
|
Benign paraganglioma |
1(6.6%) |
|
Schwannoma |
1(6.6%) |
|
Neurofibroma |
1(6.6%) |
|
Mesothelial cyst |
1(6.6%) |
The median postoperative hospitalization duration was 7 days, ranging from 2 to 37 days. The median follow-up period was 62 months, with a range of 3 to 102 months. Recurrence occurred in 5 patients, specifically 3 with high-grade leiomyosarcoma and 2 with liposarcoma. The median survival for patients with malignant tumors (n=39) was 58.5 months (range 12 to 130 months), while patients with liposarcoma (n=16) had a median survival of 92.2 months (range 42.5 to 128 months) and those with Grade I tumors had a median survival of 96.5 months (range 44.5 to 130 months). The overall survival rates, categorized by tumor type and grade, are detailed in Table 3.
Table 3: Overall survival outcomes.|
Overall Survival |
Median (months) |
|
Total malignant cases (n=39) |
58.5 (12-130) |
|
Liposarcoma (n=16) |
92.2( 42.5-128) |
|
Leiomyosarcoma (n=10) |
56.5 (24.5-120.5) |
|
Malignant fibrous histiocytoma (n=5) |
42.5 (21.5-80.5) |
|
Based on Grade |
|
|
G1 (n=13) |
96.5 (44.5-130) |
|
G2 (n=16) |
55.2 (36.5-79.5) |
|
G3 (n=10) |
23.5 (12-49.5) |
Based on our analysis of 54 cases of retroperitoneal tumors (RPTs), the average age was 50 years, with a slight male predominance (33 males to 21 females). Sassa et al. [6], in their review of retroperitoneal tumors, noted a median age of 52 years with no observable gender difference. Tseng et al. [7], examining 56 patients, reported a median age of 52 years with an even distribution between male and female patients. In a series of 28 patients with retroperitoneal tumors, Gemici et al. [8] observed a predominance of female patients (71.4% female versus 28.6% male), with the mean age being 55 years for females and 38 years for males. The median age in our cohort aligns with what has been documented in existing literature. The retroperitoneal space is generally viewed as “adaptable” [9]. Typically, retroperitoneal tumors exhibit few symptoms until they become large enough to compress or invade adjacent structures. The majority of our patients reported vague abdominal discomfort, specifically 33 cases (61.2%). Pain has been recognized as the most frequent presenting symptom of retroperitoneal tumors, with incidence rates ranging from 40% to 75%, alongside various other symptoms. Seventeen patients (31.4%) came forward with an abdominal mass. The average tumor diameter was 17.3 cm (ranging from 7 to 36 cm). In a study involving 165 French patients, Stoeckle et al. [10] noted a median tumor size of 15 cm. Most patients did not manifest symptoms until they developed large abdominal masses. A larger tumor size is associated with an increased probability of malignancy. Marcu et al. [9] highlighted the impact of retroperitoneal tumors on the digestive system, citing that over time, more than half of these tumors will exhibit symptoms related to the gastrointestinal tract. Other gastrointestinal symptoms such as early satiety and bleeding may also arise. In our analysis, 3.7% of the cases (2 patients) were discovered incidentally. Radiographic imaging is essential not only for diagnosis but also for assessing retroperitoneal masses. Our investigation of choice is a high-quality contrast-enhanced CT scan of the abdomen and pelvis (Figure 2).
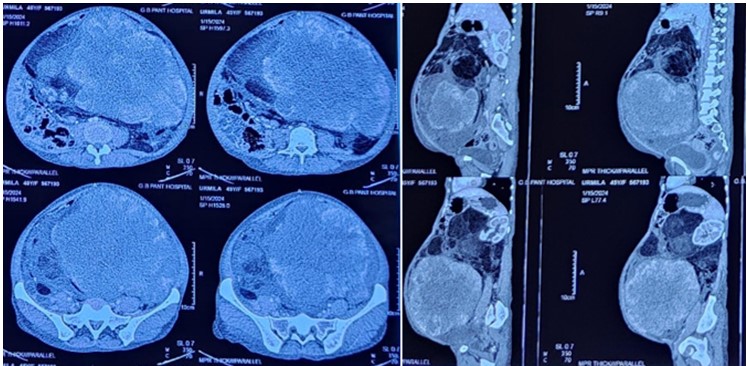 Figure 2: Preoperative CT abdomen and pelvis.
Figure 2: Preoperative CT abdomen and pelvis.Careful planning before surgery aids in anticipating possible operative scenarios and deciding on any additional procedures. A preoperative needle biopsy is performed to achieve histological typing and grading in select patients. Some studies have indicated a recurrence rate at the needle biopsy site ranging from 0.37% to 2% [11], while other studies report an insignificant recurrence rate through the needle biopsy route [12]. In managing Retroperitoneal Tumors (RPTs), surgical resection remains the only viable curative option. The significance of complete resection has been emphasized in numerous studies [13-15]. In our study, 41 patients (75.9%) underwent complete R0 resection (Figure 3), whereas only tumor debulking was performed in 5 patients (Figure 4).
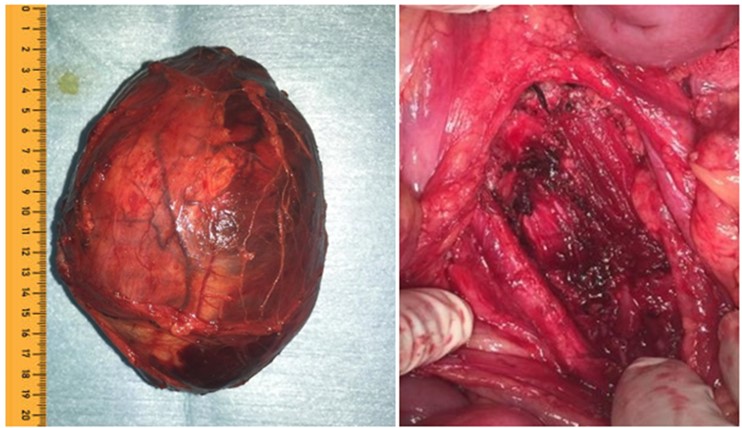 Figure 3: Specimen and operative bed.
Figure 3: Specimen and operative bed.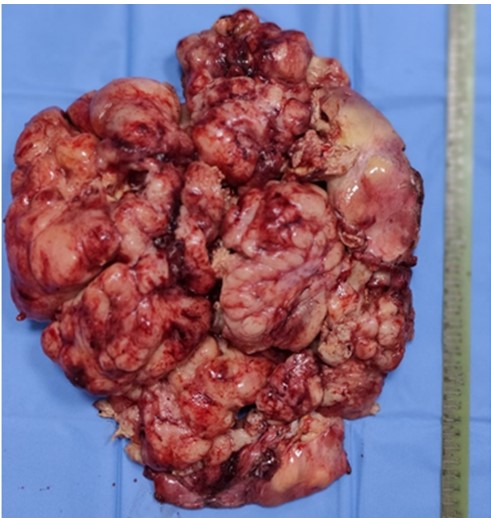 Figure 4: Tumor debulking.
Figure 4: Tumor debulking.The surgical method employed for the tumor is influenced not just by its location but also by its malignant characteristics and how it involves neighboring organs. Often, collaboration with other specialties such as urologists and interventional radiologists is essential during the preoperative preparation for ureteral stenting and the embolization of blood vessels supplying the tumor. In our study, 11 patients received bilateral ureteral stenting to facilitate identification and protection of the ureters. Associated organ resections were conducted in 9 cases in our series. Addressing retroperitoneal tumors is intricate and demanding. A multidisciplinary strategy is required to manage these cases, which involves not just surgeons but also radiation and medical oncologists. Adjuvant chemotherapy was administered to 18 of the patients in our study. There are no standard guidelines for adjuvant systemic therapy for retroperitoneal sarcoma. Treatment approaches are based on past experiences with soft tissue sarcomas. However, applying findings from soft tissue sarcomas to retroperitoneal sarcomas is challenging due to the differences in the diseases and their anatomical limitations. The STRASS 2 randomized control trial aims to assess the oncologic impact of neoadjuvant systemic chemotherapy in retroperitoneal sarcoma. This trial commenced in 2020 and is projected to conclude in 2028 [16].
The incidence of local recurrence is highest in the early period after surgery, with two-thirds of recurrences occurring within 2 years. In our series, 5 cases had recurrence (3-high grade leiomyosarcoma, 2-liposarcoma) within 2 years of follow-up despite adjuvant chemotherapy. Local recurrence remains the main reason for failure. One of the objectives of radiotherapy is to decrease the likelihood of local recurrence. Typically, preoperative external beam radiotherapy is employed [17]. The STRASS-1 trial, a multicenter randomized phase 3 trial, compared neoadjuvant radiation therapy to surgery alone. It showed no benefit of preoperative radiation therapy in decreasing abdominal recurrence-free survival compared to surgery alone irrespective of retroperitoneal sarcoma histology. The combination of external beam radiotherapy, surgery, and intraoperative radiation therapy appears to achieve better local control compared to surgery alone or surgery with external beam radiotherapy [18]. Because retroperitoneal tumors are rare, it is challenging to establish consensus guidelines for managing this disease. A global collaborative group, The Transatlantic Australasian Retroperitoneal Sarcoma Working Group (TARPSWG), comprising 150 tertiary centers, has integrated data and produced consensus guidelines, resulting in advances and understanding of the rare sarcoma [19]. Although there are various histological types of sarcomas, liposarcoma, and leiomyosarcoma constitute the majority of retroperitoneal sarcomas. In general, the majority of liposarcomas are usually low to intermediate-grade lesions. Also, liposarcoma is associated with better survival in comparison to other pathologies. Leiomyosarcoma has a worse prognosis in comparison to liposarcoma [20]. Several cohort studies have reported the postoperative morbidity rates from 13% to 26% [21]. Our findings align with the existing literature, showing grade I/II morbidity at 21.7%.
The local recurrence rate is more shortly after surgery, with approximately two-thirds of recurrences occurring within the first 2 years. In our study, there were five cases of recurrence (three high-grade leiomyosarcomas and two liposarcomas) within 2 years of follow-up despite the use of adjuvant chemotherapy. These patients also had node-positive disease in CT. Local recurrence continues to be the primary reason for treatment failure. One goal of radiotherapy is to reduce the chances of local recurrence [17]. Generally, preoperative external beam radiotherapy is used. The STRASS-1 trial, a multicenter randomized phase 3 study, evaluated the effectiveness of neoadjuvant radiation therapy versus surgery alone. The trial found no advantage of preoperative radiation therapy in improving abdominal recurrence-free survival when compared to surgery alone, regardless of the histology of retroperitoneal sarcoma. The combination of external beam radiotherapy, surgery, and intraoperative radiation therapy appears to enable better local control than surgery alone or surgery combined with external beam radiotherapy [18]. Due to the rarity of retroperitoneal tumors, it is difficult to establish universal guidelines for their management. A global collaborative entity, The Transatlantic Australasian Retroperitoneal Sarcoma Working Group (TARPSWG), which includes 150 tertiary centers, has combined data to create consensus guidelines, leading to progress and improved understanding of this uncommon sarcoma [19]. While various histological types of sarcomas exist, liposarcoma and leiomyosarcoma make up the majority of retroperitoneal sarcomas. In general, most liposarcomas are typically low to intermediate-grade tumors. Additionally, liposarcoma is linked with a better survival rate compared to other types. Conversely, leiomyosarcoma has a poorer prognosis compared to liposarcoma [20]. This goes in line with the results of this study. Several cohort studies have indicated postoperative morbidity rates ranging from 13% to 26% [21]. Our results are consistent with the existing literature, showing grade I/II morbidity at a rate of 21.7%.
Retroperitoneal tumors present significant management challenges due to their tendency to grow large and invade nearby organs and major blood vessels. Preoperative imaging is crucial for effective surgical planning. Complete surgical resection remains the primary treatment approach and offers the potential for a cure. Our findings indicate that liposarcoma and Grade I tumors are associated with better survival outcomes. There is a need for further collaborative studies to better establish optimal management strategies for these tumors, including the use of perioperative chemoradiotherapy.
None.
None declared.

