 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Guzmán-Casta Jordi1,12, Martínez-Vega Rocío Pamela5, Rubio-Cordero Jairo Aaron2,3, Téllez-Campos Lucía2,3, Carrasco-CaraChards Sonia3, Baltazar-Contreras Rocío del Carmen2 , Riera-Sala Rodrigo Fernando1,12, Guzmán-Huesca Jorge4, González-Araujo Andrea6, Hernández-Dehesa Itzel Ariadna7, Rovelo-Lima José Eduardo9, Correa-Cano Rafael10, Elvira-Fabián Karina11, López-Vrátný Claudia12, Sánchez-Dominguez Gisela14, Alcántar-Lomelí Samantha Lizeth13, Aguilar-Luevano Jocelyn15, Escobar-Gómez Mario2,8, Garnica-Jaliffe Georgina2,8
1Department of Clinical Oncology, Instituto Nacional de Enfermedades Respiratorias, Ciudad de México, México,
2Department of Clinical Oncology, Hospital General de México “Dr. Eduardo Liceaga”, Ciudad de México, México,
3Facultad de Medicina, Universidad Nacional Autónoma de México, Ciudad de México, México,
4Bonita Community Health Center, Internal Medicine, Bonita Springs, Florida, United States,
5Nutritional Department, Hospital General de México “Dr. Eduardo Liceaga” Ciudad de México, México,
6Resident of Primary Care, Instituto Mexicano del Seguro Social “IMSS”, Guanajuato, México,
7Department of Radiology, Hospital Ángeles Acoxpa, Ciudad de México,
8Centro Oncológico Internacional “COI” Ciudad de México, México,
9Deparment of Surgical Oncology Hospital Star Médica Lomas Verdes, Estado de México, México,
10Centro Médico Hospital ABC Santa Fé, Ciudad de México, México,
11Resident of Clinical Oncology, Centro Médico Nacional Siglo XXI “IMSS”, Ciudad de México, México,
12Health Pharma Professional Research, Ciudad de México, México,
13Hospital Del Valle de Atemajac, Guadalajara, Jalisco, México,
14Resident of Clinical Oncology. Centro Médico Nacional Siglo XXI Hospital de Oncología,
15Department of Oncology/Hematology Hospital H + Querétaro, México
Correspondence to: Guzmán-Casta Jordi, Department of Clinical Oncology, Instituto Nacional de Enfermedades Respiratorias, Ciudad de México, México.
Received date: February 23, 2021; Accepted date: March 4, 2021; Published date: March 11, 2021
Citation: Jordi GC, Rocío Pamela MV, Jairo Aaron RC, et al. (2021) Relationship About KI67 and Chemotherapy Regimens About Progression Free Survival in Triple
Negative Breast Cancer. J Med Res Surg 2(1): pp. 1-5. doi: 10.52916/jmrs214040
Copyright: ©2021 Jordi GC, et al.. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Objective: To determine the experience in a public institution (Hospital General de México) the relationship of KI67% and chemotherapy regimens about the progression free survival.
Design: It is a retrospective study in which a total of 64 patients with a 36-month follow-up were evaluated, evaluating the percentage of KI67 and the chemotherapy regimens, which were AC+TXL vs CBP/TXL+AC.
Results: A progression-free survival of 11.9 months was demonstrated in the patients who started with the CBP / TXL-based chemotherapy regimen and sequentially AC versus the 9.7 months achieved with the conventional ACX4 scheme and later add Carboplatin and Paclitaxel, and a Overall in both arms of 10.8 months, the patients who demonstrated the presence of a higher KI67 demonstrated increased progression-free survival compared to those with a low KI67, and with an unexpected surrogate that despite being few patients, those who showed higher levels of Progesterone had a lower survival compared to percentages of 5% or negative.
Conclusions: Despite the fact that the first-line scheme for triple negative breast cancer was sequential and that the sample was only 64 patients, it was shown that adding carboplatin in the first line together with Paclitaxel in patients with high KI67 and without or with a minimal percentage of progresterone receptors increases Progression Free Survival.
Malignancy, Breast Cancer, Triple Negative Breast Cancer (TNBC), Tumors
Breast cancer is the most frequently diagnosed malignancy and the main cause of cancer-related death in women. Globally, approximately 2.1 million new female breast cancer cases and 627,000 deaths were estimated to have occurred in 2018 [1]. Recurrence and metastasis are the major cause of these deaths. Approximately 15%-20% of these patients could be classified as “triple-negative.” The diagnosis is made by observing exclusion of the expression and/or amplification of three biomarkers (estrogen receptor [ER], progesterone receptor [PR], and Human Epidermal Growth Factor Receptor 2 [HER2] protein [2].
So-called Triple Negative Breast Cancer (TNBC) is more commonly diagnosed in women younger than 40 years compared to hormone-positive breast cancer [3]. The histology is usually high grade and most commonly interpreted as infiltrating ductal carcinoma, which exhibits geographic necrosis, a pushing border of invasion, and a stromal lymphocytic response. Clinically, TNBC tends to act more violently than other types of breast cancer and is characterized by a high risk of relapse, short progression-free survival (PFS), and overall survival (OS) [4]. One-half of patients with earlystage TNBC (stages I to III) experience disease recurrence, and 37% of patients experience a 5-year mortality rate after surgery [5].
Also, patients with metastatic TNBC have short PFS after failure of first-line chemotherapy (median PFS, 3 to 4 months), suggesting the highly unmet need for the development of a drug targeting TNBC [6]. TNBC is clinically heterogeneous, with deviations in morphology, mutational phenotype, and signaling profiles between tumors. Notably, the diagnostic criteria have not been developed to distinguish a distinct biologic subtype of breast cancer-a “triple-negative” phenotype. A histologic subtype, medullary carcinoma, despite generally being triplenegative, has a very good prognosis [7]. Due to next-generation sequencing, our understanding of the heterogeneity of TNBC is evolving. For example, TNBC can be clustered into at least six subtypes on the basis of gene ontologies and expression profiling: basal-like 1, basal-like 2, immune modulator, mesenchymal, mesenchymal stem–like, and luminal androgen receptor [8]. Additional subtypes include claudin-low and interferon-rich subtypes [9,10]. Furthermore, the tumor suppressor gene p53 (TP53) and several DNA repair genes, particularly the BRCA genes, are either mutated or abnormally expressed in TNBC. These molecular characteristics may influence chemotherapy sensitivity to direct DNA-damaging agents such as platinum [11,12].
Triple-negative breast cancers encompass other molecular subtypes of breast cancer. These include the so-called claudinlow tumors, which are reported to be enriched with cells that have properties similar to those of stem cells and to have features of epithelial-to-mesenchymal transition; the interferon-rich subgroup, which encompasses tumors with a considerably better prognosis than that associated with other triple-negative breast cancers; and the normal-breast– like subgroup, which may be an artifact (i.e., it may comprise samples enriched with a disproportionately high content of stromal and normal cells) [13,14]. Similarly, 18 to 40% of basal-like cancers do not have a triple-negative phenotype on immunohistochemical analysis [15]. Up to 20% of basallike cancers express ER or overexpress HER2. At the genetic level, triple-negative and basal-like cancers are remarkably heterogeneous.
negative [18] and basal-like [19] breast cancer occur more frequently in young black and Hispanic women than in young women of other racial or ethnic groups. BRCA1 is an important breast-cancer susceptibility gene; more than 75% of tumors arising in women carrying a mutation in this gene have a triplenegative phenotype, a basal-like phenotype, or both [12,17].
KI-67 is a nuclear protein. Cytoplasmic staining and occasional membrane staining of KI-67 can occur with MIB1 antibody and should be ignored when scoring KI-67. Only nuclear staining (plus mitotic figures stained with KI-67) should be incorporated into the KI-67 score that is defined as the percentage of positively stained cells among the total number of malignant cells scored. Similar to other IHC stains, internal positive controls, such as mitotic figures, normal ducts, and lymphocytes, and endothelial and stromal cells (lesser extent), are helpful [20,21].
KI-67 may predict the pathological remission rate in breast cancer patients following neoadjuvant chemotherapy, as an increased KI67 level following neoadjuvant chemotherapy indicates a poor prognosis [22,23]. Therefore, KI67 is considered to be one of the most significant indicators in detecting the proliferation of tumor cells [24]. The expression of KI67 reliably and quickly reflects the proliferation of malignant cells; it closely correlates with the prediction of the development, metastasis and local recurrence of a variety of malignant tumors [25].
The study of the 64 patients evaluated during 36 months of follow-up was carried out, where the average progression-free survival of both arms was 10.8 months close to the literature, being higher for the group which started the treatment based on Carboplatin/Paclitaxel and sequentially ACX4 where up to 11.9 months free of progression was obtained compared to the usual scheme of starting with Anthracyclines and without adding Platinums with a survival of 9.7 months (Figure1-4).
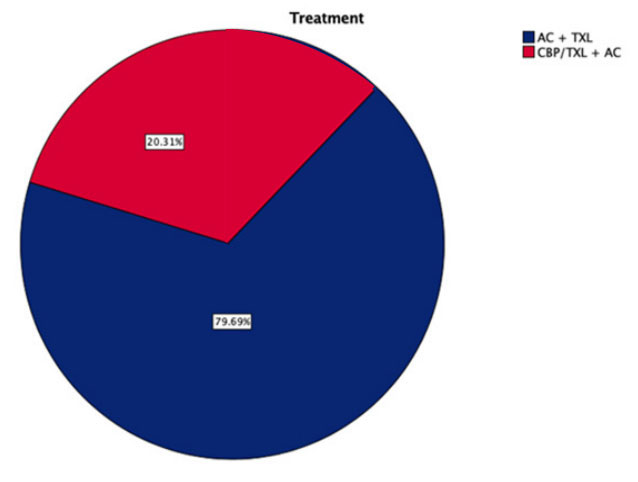 Figure 1: Type of chemotherapy regimens used AC+TXL(Doxorubicin+Cyclophosphamide+sequential Paclitaxel)vs-CBP/TXL+AC-(Carboplatin+
Paclitaxel+Sequential Doxorubicin and Cyclophosphamide).
Figure 1: Type of chemotherapy regimens used AC+TXL(Doxorubicin+Cyclophosphamide+sequential Paclitaxel)vs-CBP/TXL+AC-(Carboplatin+
Paclitaxel+Sequential Doxorubicin and Cyclophosphamide).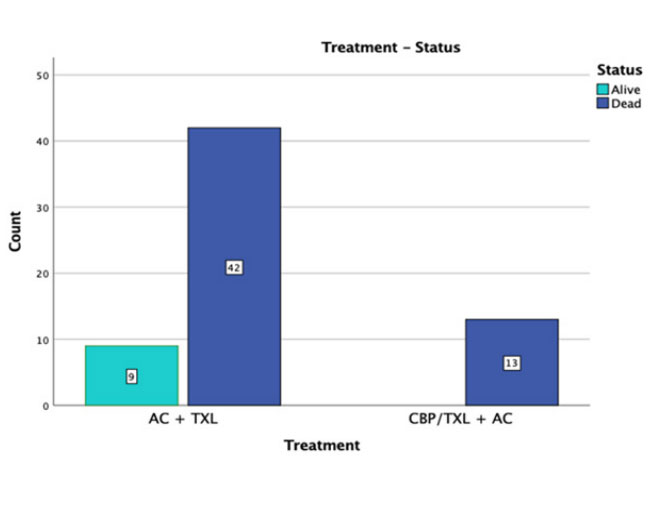 Figure 2: Current patient status after treatment and follow up 36 months.
Figure 2: Current patient status after treatment and follow up 36 months.
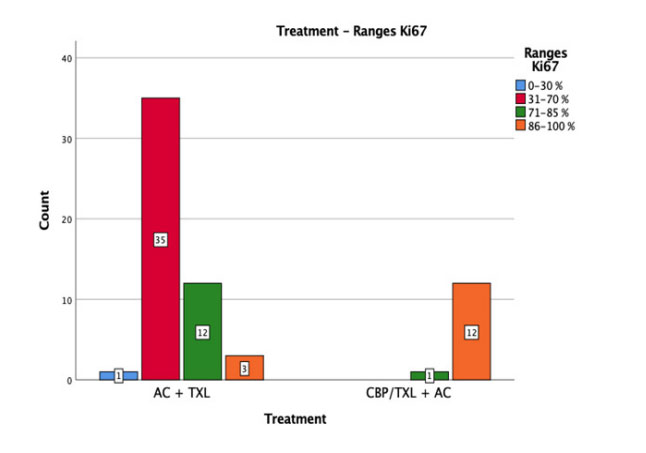 Figure 3: The ranges of KI67 of both arms of treatment AC+TXL vs CBP/TXL
+ AC.
Figure 3: The ranges of KI67 of both arms of treatment AC+TXL vs CBP/TXL
+ AC.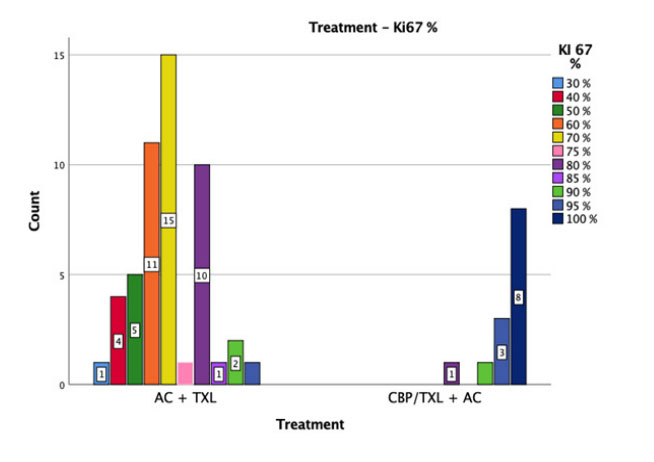 Figure 4: KI67% respect to number of patients in both arms.
Figure 4: KI67% respect to number of patients in both arms.
The relationship between the schemes and the expression of the percentage of KI67 was significant given that in patients with a KI67 of 100% they had the best progression-free survival, as well as the range of 86 to 100% and, on the other hand, Although there were very few patients due to the type of population being treated, those that expressed progesterone receptors for the least (5%) had a worse progression-free survival than the pure triple negatives in which there is no expression of hormonal receptors, making an important distinction that the few patients who came to express progesterone receptors of 15% had their median progression-free not exceeding 4 months (Figure5-9).
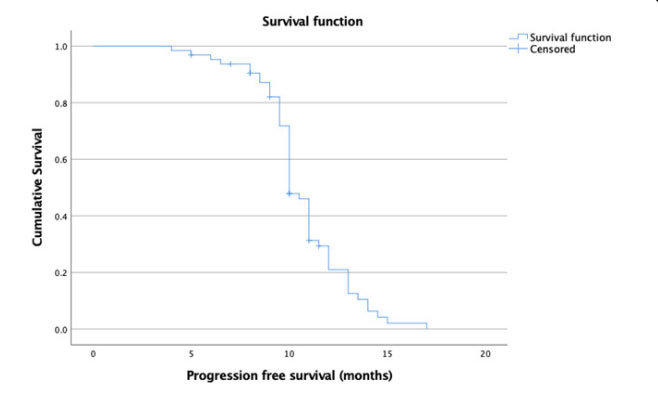 Figure 5: Progression Free survival in both arms.
Figure 5: Progression Free survival in both arms.
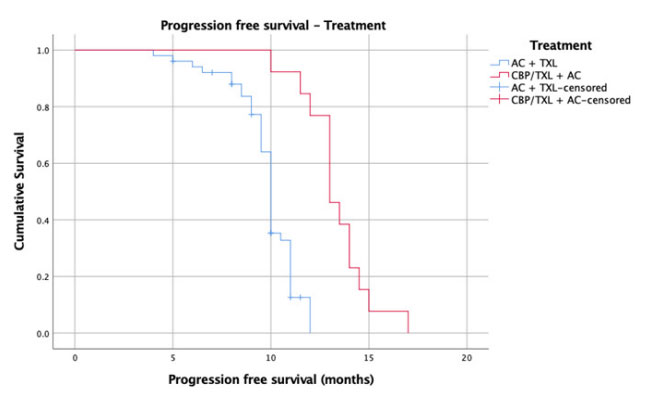 Figure 6: Progression free survival in different arms AC+TXL vs CBP/TXL + AC.
Figure 6: Progression free survival in different arms AC+TXL vs CBP/TXL + AC.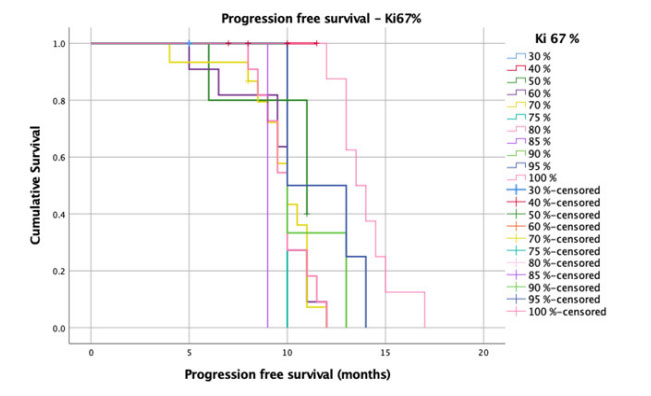 Figure 7: Progression Free survival depending KI67%
Figure 7: Progression Free survival depending KI67%
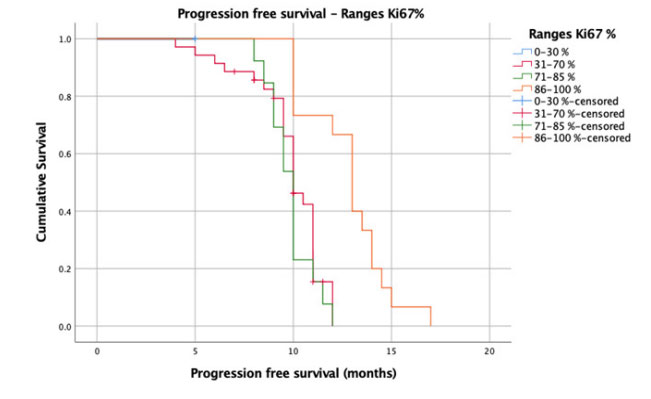 Figure 8: Progression free survival depending range of KI67%.
Figure 8: Progression free survival depending range of KI67%.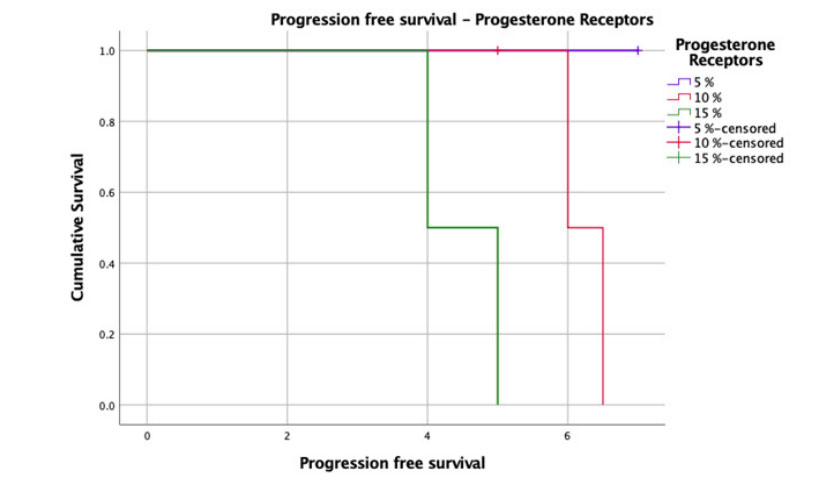 Figure 9: Progression free survival depending Progesterone receptors status.
Figure 9: Progression free survival depending Progesterone receptors status.It is interesting to know the biology and behavior that triple negative breast cancer can have, both in the response to different chemotherapy treatment schemes that are currently the mainstay that options such as starting with an “inverted therapy” adding an agent such as Platinum we know that there is a decrease in intraluminal pressure added to taxane and subsequently the sequence with anthracyclines or the conventional and accepted worldwide scheme such as the start of Anthracyclines and later Taxanes without adding platinum, which has been shown to increase response rates .
The implication of KI67 was observed that the higher the proliferation rate these tumors have, they will have a greater objective response and in our study, it was demonstrated in progression-free survival with a platinum-based and more “aggressive” scheme where the prolongation in months of 2.2 was observed. months compared to the conventional scheme and a lower KI67.
The fact that they express progesterone receptors gives us a poor prognosis in progression-free survival, as we observed, the vast majority of our patients were a “pure” triple negative with months of survival described in the literature, however the fact that they have expressed estrogen receptors from 5% to 15%, knowing that there are other signaling pathways for expression, these patients had progression-free survival of 4 to 5 months, practically half the months established for the rest of the patients.

