 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Aliya Ishaq1* , Yasir Amin Abdellatif2, Syed Mohammed Javed1, Nisha Kunal1, Sameera Naureen2, Muhammad Jamshaid Husain Khan3, Maryum Essa Ali1, Arfan Al Awa4, Esaaf Hassan Ghazi4, Zaid Abdulaziz5
, Yasir Amin Abdellatif2, Syed Mohammed Javed1, Nisha Kunal1, Sameera Naureen2, Muhammad Jamshaid Husain Khan3, Maryum Essa Ali1, Arfan Al Awa4, Esaaf Hassan Ghazi4, Zaid Abdulaziz5
1Specialist General Surgeon, Dubai Hospital, Dubai, UAE
2Senior Specialist General Surgeon, Dubai Hospital, UAE
3Specialist, Internal Medicine, Dubai Hospital, UAE
4Consultant General and Breast Surgeon, Dubai Hospital, UAE
5Consultant General and Bariatric Surgery, Dubai Hospital, UAE
Correspondence to: Aliya Ishaq, Specialist General Surgeon, Dubai Hospital, Dubai, UAE
Received date: August 04, 2022; Accepted date: August 25, 2022; Published date: September 01, 2022
Citation: Ishaq A, Abdellatif YA, Javed SM, et al. Primary Large Diffuse B Cell Lymphoma Presenting as Rapidly Enlarging Thyroid Mass with Compressive Symptoms:
A Case Report. J Med Res Surg. 2022; 3(S2): 8-11. doi: 10.52916/jmrs22S203
Copyright: ©2022 Ishaq A, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted
use, distribution and reproduction in any medium, provided the original author and source are credited.
Background: Primary thyroid lymphoma are seen occasionally accounting for 5% among thyroid tumors.
Commonest of these lymphomas is diffuse large B cell type.
Case report: A 66 years old female presented to our Department with rapidly enlarging thyroid mass
having difficulty in swallowing as well as breathing. She underwent left hemithyroidectomy 30 years ago
for a benign disease. Clinicallly it was a large mass 20 × 20 cm hard inconsistency and clinically attached
to sternocleidomastoid muscles with no skin and lymph node involvement. Computed Tomography (CT)
scan of neck with contrast showed large ill-defined mass noted arising from the right lobe of the thyroid
gland encasing the common carotid with loss of fat planes between the mass and the right jugular vein,
sternocleidomastoid, trachea, esophagus suggesting involvement. She underwent incisional biopsy of
mass which showed Diffuse Large B Cell Lymphoma (DLBCL).
Discussion: Most of thyroid lymphomas originate from B cells. Fine Needle Aspiration Cytology (FNAC)
can diagnose 80-85% of cases but definitive diagnosis can be made by biopsy only. Surgery has a limited
role in treatment and main modality is chemoradiotherapy.
Conclusion: A rapidly enlarged thyroid swelling should be suspected of having lymphoma specially on
the background of lymphocytic thyroiditis and multidisciplinary team approach should be used for
management.
Primary thyroid lymphoma, Diffuse large B cell lymphoma, Hashimoto’s thyroiditis, Rapidly enlarging thyroid mass
Thyroid lymphomas are rare tumors, presenting in middle to older aged females [1]. It accounts for 5% to 15% [2].
It generally originates from B cells. Diffuse B-Cell Lymphoma (DBCL) accounts for 50-80% of all PTL and, thus is considered the most common type of Primary Thyroid Lymphoma (PTL). PTL is diagnosed through biopsy, and its management is decided on the basis of its histological type [3].
We report a case of thyroid lymphoma that presented as a rapidly compressive goiter in a 66 years old woman with no evidence of hashimoto's thyroiditis.
A 66 years old female patient who was diabetic and hypertensive with history of ischemic heart disease and was on anticoagulants presented to Emergency Department of our Hospital with complaints of rapidly enlarging neck mass since past 15 days. She was also having associated symptom of shortness of breath and audible breath sounds with dysphagia to solid food as well, she has to chew the food very nicely to make it finely chopped and nicely mixed with good quantity of saliva other wise the usual chewed bolus was having very pain full swallowing requiring large amount to water to ingest with some discomfort. However, there was no difficulty in swallowing meshed diet and liquids also there was no history of aspiration for any kind of food. She had past medical history of left hemithyroidectomy which was done 30 years for a benign goiter however, she did not have any report with her elaborating her past surgical procedure or histopathology report. On examination she was hemodynamically stable and was maintaining oxygen saturation on room air (98-99% ), she was having expiratory wheeze. Her neck examination showed huge swelling at anterior part of neck around 20 × 20 cm firm to hard inconsistency, not attached to overlying skin however it was fixed to sternocleidomastoid muscles on both sides, clinically retrosternal extension was not appreciated neither any lymph nodes were palpable. There was no bruit audible and overlying skin was normal with out any engorged veins.
No lymph node were palpable clinically. She had an FNAC done in another facility a couple of days ago and it was showing non diagnostic aspirate for left thyroid gland and lymphocytic (hashimoto’s thyroiditis ) for right thyroid gland.
Her thyroid function tests showed Thyroid Stimulating Hormone (TSH) level of 5.420 uIU/mL (normal range 0.27-4.2 uIU/mL) with normal T3 and T4 levels and she was not on any treatment.
A contrast CT scan of her chest was done which showed.
Large ill-defined mass noted arising from the right lobe of the thyroid gland encasing the common carotid with loss of fat planes between the mass and the right jugular vein, sternocleidomastoid, trachea, esophagus suggesting involvement. The mass lesion appears to be neoplastic.
Left lobe of the thyroid gland is also enlarged which may be secondarily involved. Level V lymphadenopathy noted in the neck. Mass effect noted over the trachea and the esophagus as described. Visualized lungs and brain appears normal (Figure 1-4).
 Figure 1: CT scan neck of same patient showing diffuse thyroid mass with tracheal compression and narrowing
Figure 1: CT scan neck of same patient showing diffuse thyroid mass with tracheal compression and narrowing Figure 2: CT scan neck with contrast of same patient diffusely enlarged
thyroid showing airway compromise in coronal view.
Figure 2: CT scan neck with contrast of same patient diffusely enlarged
thyroid showing airway compromise in coronal view.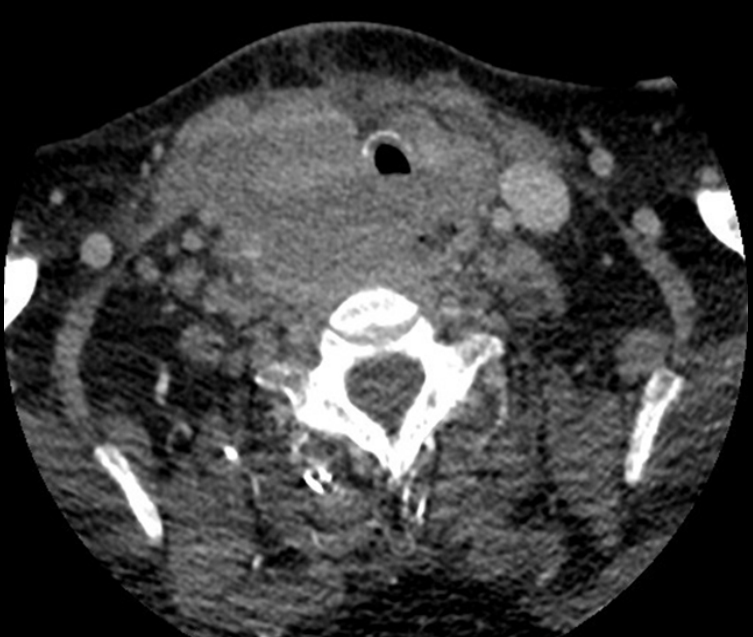 Figure 3: Diffusely enlarged thyroid showing airway compromise in another
view for same patient.
Figure 3: Diffusely enlarged thyroid showing airway compromise in another
view for same patient.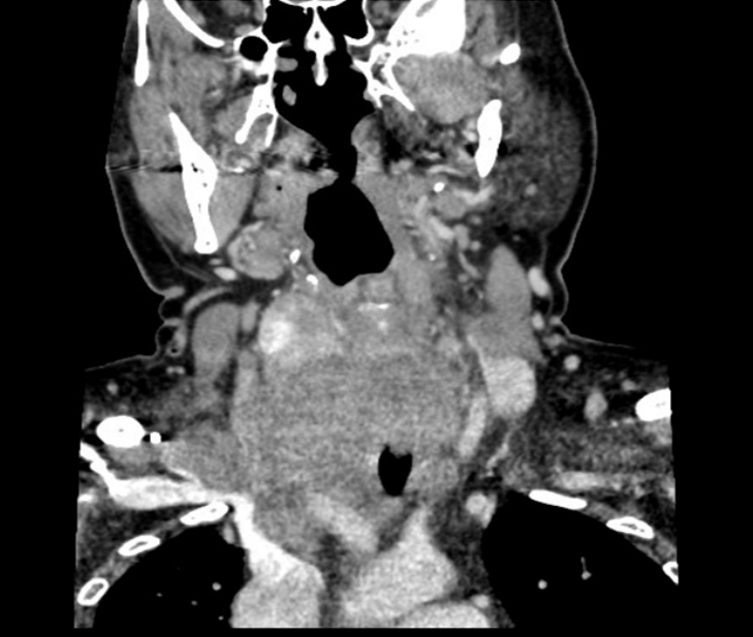 Figure 4: Diffusely enlarged thyroid showing airway compromise in sagittal
view.
Figure 4: Diffusely enlarged thyroid showing airway compromise in sagittal
view.Patient was admitted from emergency and was co-managed with endocrinology, medical, cardiology and Intensive Care Unit (ICU) team and after multidisciplinary team meeting it was decided go for surgical exploration.
Nasopharyngoscopy revealed:
She was taken to operation and per operatively it was found to be a huge thyroid gland morphologically whitish in color, heard and cheesy in nature/anaplastic, invading surrounding structure right and left carotid and jugular vessels and muscles being inoperable so decision made to take thyroid biopsy only from left lobe.
Incisional biopsy was taken and wound was closed. Patient did not show any signs of respiratory distress so was extubated and tracheostomy was not made as well and patient was kept in high dependency.
Patient during admission never showed any signs of hypoxia and oxygen saturation levels were within normal limits with out supplemental oxygen so tracheostomy was not done also she was used to her way of chewing food nicely and swallowing the food therefore she refused for nasogastric tube or any other intervention.
Histopathology showed diffuse large B-cell lymphoma of nongerminal center origin profile, which is probably arising in a background of lymphocytic fibrosing thyroiditis. Epstein-Barr Virus (EBV) positivity may raise the possibility of EBV-associated diffuse large B-cell lymphoma of the elderly. Clinical, serologic and radiologic correlation is recommended.
Immune histochemistry showed Immunohistochemistry (IHC) for the following markers (CD20, CD3, Ki67, bcl2, bcl6, CD10, MUM1, c-myc, CD30, CD5, EBV and CD23) was performed. The foci of tumor cells showed diffuse and strong staining for CD20 and EBV. These foci showed variable staining for bcl2, bcl6, MUM1, c-myc (30%) and CD30 (30%). They showed 80% Ki67 proliferation index. They were negative for the remaining markers. CD3 and CD5 showed prominent background inflammatory T-lymphocytic background. The IHC results are consistent with diffuse large B-cell lymphoma of non-germinal center origin profile, which is probably arising in a background of lymphocytic fibrosing thyroiditis. EBV positivity may raise the possibility of EBV-associated diffuse large B-cell lymphoma of the elderly. Clinical, serologic and radiologic correlation is recommended.
Patient was referred to Hematology Department for further management by chemotherapy and through out this period did not show any signs of respiratory compromise. Patient however, left against medical advice and lost follow up.
Primary thyroid lymphoma is an uncommon lymphoma that develops in the thyroid gland, accounting for 2-5% of cases . Diffuse large B cell lymphoma is the main type, other pathological subtypes include follicular lymphoma, mucosa-associated lymphoid tissue lymphoma, small lymphocytic lymphoma, and T-cell lymphoma [4]. Primary thyroid lymphomas usually have a widespread expression of B-cell antigens [5]. IL-7 expression can be used to differentiate between lymphocytic thyroiditis and primary thyroid lymphomas [6]. There is no specific image feature for these malignancies hence making there differentiation difficult from other thyroid disorders. Ultrasound is the basic initial investigation to look for thyroid abnormalities and it will either show well defined nodular lesion or well differentiated nodules with hypoechoic and internal echoes versus lesions with indistinct borders or multiple irregular hypoechoic lesions [7].
CT scan is used to elaborate more about thyroid lesions details and to look for anatomy and relationship to adjacent structures as well as pressure effects and retrosternal and primary thyroid lymphomas usually have a density lower than the adjacent muscles [8].
The diagnosis of primary thyroid lymphoma is usually made after thyroidectomy on histopathological basis. FNAC can diagnose 50-90% cases of thyroid lymphoma however it shows many similar features hashimoto's thyroiditis, anaplastic carcinoma, and riedel's thyroiditis hence, making lobectomy and core biopsy the preferred diagnostic modalities [9].
Optimal treatment for diffuse large B cell lymphoma has not been establishes and role of surgery is mainly limited to biopsy of specimen, some literature has reported surgical excision [10]. However, even with surgical excision patients have no significant prognostic advantage.
A study from the Mayo Clinic showed that surgical excision did not have any advantage over the simply performed surgical biopsy for diagnosis. Patients who underwent surgical biopsy and chemotherapy had better prognosis than those with surgical excision followed by adjuvant chemotherapy [11]. Therefore, chemotherapy and Radiation Therapy (RT) have replaced surgery as the main treatment measure [12]. Prognosis depends on the age, histological grade and stage of the disease. Tumor size, adherence to surrounding structures, extra-capsular extension, and retrosternal involvement are the main prognostic factors [13].
Prognosis is poor for diffuse-large B cell lymphoma when compared to localized primary Mucosa-Associated Lymphoid Tissue Lymphoma (MALTOMAS) being very poor stage IIIE and IVE with a 5-year survival rate of 15%–35%. Poorer prognosis is also attributable to Rapidly enlarging tumors with compressive symptoms and vascular involvement [14].
In our case the presentation and radiological findings were suggestive of neoplastic nature. FNAC however was not diagnostic but it did show lymphocytic thyroiditis and thyroid lymphomas do occur on background of lymphocytic thyroiditis. Incisional biopsy in our case diagnosed the condition but later on patient lost follow up.
Any rapidly enlarging mass should have high suspect of primary thyroid specially if associated with a back ground of lymphocytic/ hashimoto’s thyroiditis. Diagnostic confirmation needs histopathology with immunohistochemistry. Multidisciplinary team approach should be used for the management.
This case report was written and images of patient’s scans were added after taking consent from patient and patient’s identity is not shown here and will be kept confidential.
No.
The autors declare that they have no conflict of interests.


