 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Imtiaz Ali* , Rida Zainab, Khubab Khalid, Syeda Baneen Fatima, Muhammad Ayub Mansoor, Khansa Abro
, Rida Zainab, Khubab Khalid, Syeda Baneen Fatima, Muhammad Ayub Mansoor, Khansa Abro
Department of Radiology, Liaquat National Hospital, and Medical College, Karachi, Sindh, Pakistan
Correspondence to: Imtiaz Ali, Department of Radiology, Liaquat National Hospital, and Medical College, Karachi, Sindh, Pakistan
Received date: August 28, 2022; Accepted date: September 22, 2022; Published date: September 29, 2022
Citation: Ali I, Zainab R, Khalid K, et al. Post-Cholecystectomy Gossypiboma Mimicking the Liver Hydatid Cyst. J Med Res Surg. 2022; 3(5): 96-98. doi: 10.52916/jmrs224087
Copyright: ©2022 Dumanli A, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted
use, distribution and reproduction in any medium, provided the original author and source are credited.
Gossypiboma is also called as retained foreign body or surgical sponge a rare and serious complication following the major surgical intervention. It is commonly occurred after major abdomino-pelvic surgery and can cause significant morbidity and mortality. We present a case of large gossypiboma within the liver parenchyma in post-operative patient radiologically mimicking the hydatid cyst and its surgical findings.
Gossypiboma, Surgical sponge, Retained, Hydatid cyst, Textiloma
Gossypiboma is defined as retained surgical sponge or mass of cotton matrix in peritoneal cavity, organs or in other body compartments after major surgeries [1-3]. Retained foreign body is a rare complication after surgical intervention frequently after abdomino-pelvic surgery however, it can also occur rarely after thoracic, orthopedic, urological and neurosurgical procedures [1,3,4]. Most common retained foreign body is surgical sponge [1]. It may lead to medico-legal implications and diagnostic dilemma due to diagnostic procedures and therapeutic operation [1,2]. Most frequent risk factor for gossypiboma or retained foreign body is unplanned or emergency surgery, high body mass index or multiple surgical teams involved [1,5,6]. Clinically it is more important and frequently occurred than reported cases [3]. It can be discovered few days after surgery or remains undetected for years if asymptomatic [2,3,7]. Clinical symptoms are nonspecific and variable may be early or late depends on the location, inflammatory reaction, involved organs, and complication [1-3,5]. Most common clinical presentation of patient is intestinal obstruction [5,8]. It is difficult to diagnose because of asymptomatic and nonspecific symptoms [2,3]. History of surgery, physical examination, laboratory investigation, and radiological imaging can help to reach the correct diagnosis [2,3]. It can mimic the soft tissue tumor, abscesses, or ecchinococcal lesions on Computed Tomography (CT) scan [3].
A-65 years old male patient was presented in Emergency Department with complaints of nausea, vomiting, abdominal pain and shortness of breath for few days. He had past history of open cholecystectomy and appendectomy 2 years back.
On physical examination there was oblique incision scar on right hypochondriac region and right iliac fossa. Large mass was palpable in right hypochondriac region. The initial baseline laboratory investigations turned out to be negative and noncontributory to any diagnosis. He underwent the ultrasound scan which showed large heterogeneous mass within the right lobe of liver with no definite internal vascularity. This was reported as neoplastic lesion (Not shown here). Patient underwent contrast enhanced CT scan abdomen for characterization of liver mass. CT scan showed large hypodense non enhancing mass in right lobe of liver. It showed few hyperdense areas, which were considered as calcification and internal membrane like structures. It measured 13.2 × 12.3 × 10.0 (AP × TS × CC) (Figure 1). This was reported as hepatic hydatid cyst. On the basis of CT scan imaging findings, the ecchinococcus titer was sent and turned out to be negative. The CT scan again was reviewed by Radiologist on request of surgeon and following negative workup for ecchinococcal lesion. The diagnosis of gossypiboma was raised in presence of previous history of open cholecystectomy and thin hyperdense thread of gauze piece which is imaging diagnosis of gossypiboma (Figure 2).
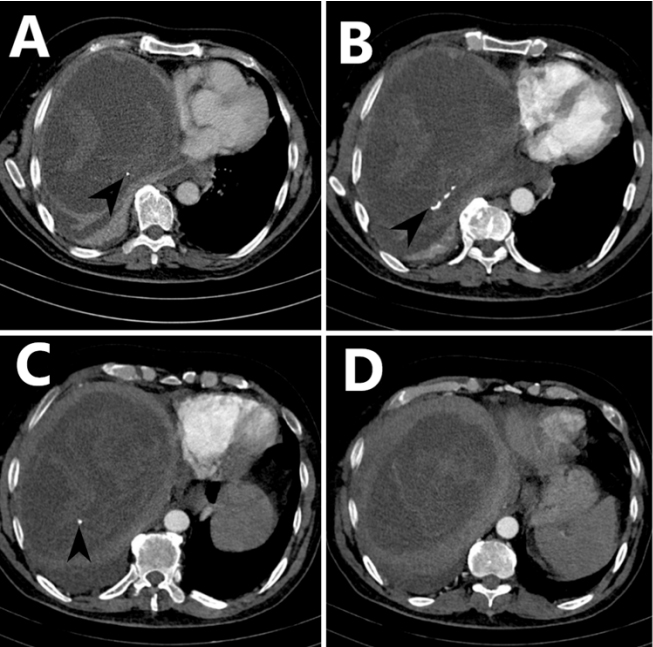 Figure 1: : Contrast enhanced CT scan liver axial images show large hypodense
non-enhancing mass in right lobe of liver. Few hyper-densities are seen
within the mass consistent with metallic density thin thread of gauze sponge
(black arrow heads in A, B, C).
Figure 1: : Contrast enhanced CT scan liver axial images show large hypodense
non-enhancing mass in right lobe of liver. Few hyper-densities are seen
within the mass consistent with metallic density thin thread of gauze sponge
(black arrow heads in A, B, C).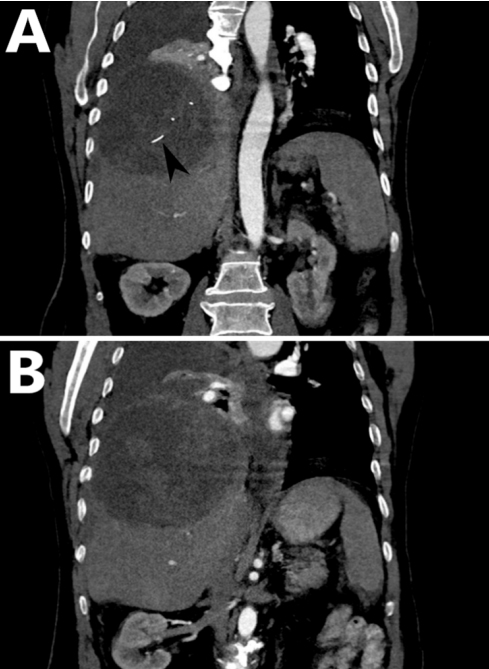 Figure 2: Contrast enhanced CT scan liver coronal images show large
hypodense non-enhancing mass in right lobe of liver. Few hyper-densities
are seen within the mass consistent with metallic density thin thread of
gauze sponge (black arrow head A).
Figure 2: Contrast enhanced CT scan liver coronal images show large
hypodense non-enhancing mass in right lobe of liver. Few hyper-densities
are seen within the mass consistent with metallic density thin thread of
gauze sponge (black arrow head A).After written and informed consent, baseline investigations, pre-operative workup and general anesthesia fitness, she was booked for elective intra-abdominal open surgery and shifted to operation theater. On opening the patient large gauze sponge with mass like structure was embedded within the liver parenchyma was removed successfully and hemostasis was secured (Figure 3). The patient went through the smooth recovery with no drastic or minor complication, and was kept on antibiotics and symptomatic treatment in hospital post-operative course and on follow up visit. Post-operative radiological imaging showed no evidence of mass in liver or collection (Not shown here).
 Figure 3: Shows post-surgical large gauze piece/sponge in surgical bowel
removed from liver parenchyma.
Figure 3: Shows post-surgical large gauze piece/sponge in surgical bowel
removed from liver parenchyma.The term gossypiboma was initially introduced by Wilson in 1884. These were made up of non-absorbable textile materials that are left within the abdominal cavities during major surgeries therefore the term “Textiloma” is also used [1]. Although very rare, textiloma can lead to serious medico-legal complications between doctor and patients and are thus considered significant. Gossypiboma or textiloma is most commonly seen after surgeries related to abdomino-pelvic cavities, but it can also follow thoracic, orthopedic, urological and neurosurgical procedures [1,2]. The estimated incidence of a textiloma has been reported to be 1 in 100 to 3,000 for all surgical procedures and 1 in 1,000 to 1,500 for abdominal surgery [2].
Generally surgical sponges have radiopaque markers as shown in our case (Figure 1) that facilitate detection through radiography however, sponges without these markers are still being used in some institutions, decreasing the chance of detection of gossypiboma by direct radiography and even by abdominal CT scan [3]. Thus raising the possibility of hydatid cyst as one of the initial differential diagnosis. Hydatid cyst appears as non-enhancing complex cystic mass with or without calcification. Gossypiboma can give similar appearances, however the presence of thin thread metallic density, negative ecchinococcal titer and recent surgical history are major key factors in excluding hydatid disease [1,2].
On plain X-rays, gossypiboma appears as soft tissue mass the most important finding is the metallic wire. With ultrasound, it appears as a complex hypoechoic or cystic mass with wavy internal hyperechoic material resembling a Hydatid cyst and posterior shadowing. On CT it appears as a well-defined mass of heterogeneous attenuation with or without foci of air, wall enhancement, calcification and metallic density object within it. There may be associated perilesional inflammatory changes and abscess formation [3-6].
Two types of foreign body reactions have been explained with sponges that are missed in patients. The frequently seen is an aseptic fibrous response resulting in adhesion, encapsulation, and granuloma formation. Patients usually remain asymptomatic and the retained sponges are detected incidentally. The other foreign body reaction in retained sponge cases involves an exudative inflammatory reaction with abscess formation or chronic internal or external fistula formation. This is believed to be associated with transmural migration of retained sponges [3,4]. Most clinical symptoms are dependent on the gossypiboma location, impact of the inflammatory reaction on adjacent organs; therefore, intestinal obstruction is a frequent clinical presentation. Other nonspecific symptoms like pain, fever, lump formation may also greatly vary from immediate postoperative period to several years later [5,6].
Gossypiboma is treated by surgical excision. Keeping count of surgical sponges and other material, proper training of nursing staff and surgical team co-ordination are some the factors to play role in future prevention of Textiloma [6].
Gossypiboma is rare complication after abdomino-pelvic surgeries and difficult to diagnose. Radiologist should be aware of imaging findings of gossypiboma and keep in mind the differential diagnosis of hydatid cyst in presence of previous surgical history even in country where Hydatid cysts are common lesions.
This case report was written and images of patient’s scans and post-operative images were added after taking consent from patient and patient’s identity is not shown here and will be kept confidential.
The authors declared, there is no conflict of interest.
No funding or grant support.

