 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Yulia Bogdanova Peeva*
Department of Social Medicine and Public Health, Faculty of Public Health, Medical University, Plovdiv, Bulgaria.
Correspondence to: Yulia Bogdanova Peeva, Department of Social Medicine and Public Health, Faculty of Public Health, Medical University, Plovdiv, Bulgaria.
Received date: November 22, 2024; Accepted date: December 06, 2024; Published date: December 13, 2024
Citation: Peeva YB. Patient Perceptions and Unique Requests in Orthodontic Treatment: Oral Health, Functionality, and Aesthetics. J Med Res Surg. 2024;5(6):124-129. doi: 10.52916/jmrs244151
Copyright: ©2024 Peeva YB. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Introduction: The question of human beauty depends on the canons in different cultures, but it also changes over time and place. So, if the beaty understanding in the worldwide differ how to be sure that something or especially the face and smile are beautiful? The answer to the question seems to be based on the proportions and personal perceptions of beauty. Scientists, artists and philosophers are increasingly aware of the central mathematical/geometrical application of beauty in nature. The dentist could “catch” the beauty in the simplicity of the smile.
The aim of the current study is to represent the boundaries in esthetics and harmonious perceptions of patient and doctor that can lead to successful orthodontic treatment.
Materials and methods: 872 patients were examined to assess the aesthetic needs for orthodontic treatment in children and adults during a sociological survey. They differ in their orthodontic needs and patients in their understanding of beauty. Some of them had unusual requests to the orthodontist. Children (n=260) participated in the study with an average age of 12.56 ± 3.14 years, respectively 12.38 ± 3.22 years for boys and 12.69 ± 3.07 years for girls, P>0.05. The number of adult patients who participated in the study was n=612. At the age of 36-40 years, the sex distribution was 32.39 ± 3.21% for women and 9.39 ± 2.0% for men, P<0.05 (u=14.60).
Results and Discussion: Two factors were extracted as significant for aesthetics according to the respondents. For this purpose, Principal Component Analysis – PCA was used, and the parents and children expectations at the first orthodontic consultation were analyzed. The results were compared with those achieved at the end of treatment. At baseline, the statements “I want to have straightened teeth”, “My parents want them, I don’t want to wear braces” and “I don’t like my teeth look” had the highest correlation coefficients, respectively rxy=0.90, rxy=0.87, rxy=0.83. In the final stage of treatment, the children’s opinions focused on the long-term benefits of orthodontic treatment. “I want to be more confident”, “I want to have a lot of success in the future because I can smile more now”, “My teeth will be healthier because they are straight and I know how to clean them”, respectively rxy=0.93, rxy=0.90, rxy=0.88. Factorial signs in the perception of function and aesthetics in the maxillofacial region were evaluated.
Conclusions: Social medicine is the unifying link between the patient's (subjective) and the doctor's (objective) understandings of disease or condition (beauty). Awareness is that stone "that can overturn a car on the road." Inappropriate (such as age, gender, social group) awareness can affect the psycho-social perception of the problem and create complexes in the patient's perception. This process is particularly noticeable when evaluating the aesthetics of the orofacial complex. In fact, one of society's expectations from the dentist is to educate. To educate in aesthetics and beauty through his work. And to manage patient’s perceptions of what is good or bad in facial esthetics.
Sacred geometry, Esthetics, Perceptions, Orthodontic treatment needs.
The beauty of smile - ethical and cultural considerations. The question of human beauty depends on the canons and understandings of aesthetics in different cultures. Perception also changes over time. From Leonardo da Vinci's "Vitruvian Man" (1490) to the present day, the search for harmonious proportions and physical perfection of the human body has accompanied the achievement of a functional and aesthetic optimum. The meaning of knowledge is in changing human consciousness for the better. It increases productivity and activity of the human personality [1-7]. The main answer to the question seems to be based on proportions. This approach is most often professional and requires accuracy and concentration on the part of the orthodontist to prepare a cephalometric analysis, treatment plan and implementation of the treatment. For the overall satisfaction of both parties - dentist and patient, it is necessary to clarify expectations from the beginning. Scientists, artists, and philosophers also have used the central mathematical/geometric application of beauty in nature for centuries to create masterpieces. For dentists, beauty lies in the attractiveness of the smile, straightened and healthy teeth and periodontium, and is perfect when it reveals the patient's satisfaction with the doctor's work well done. Dentistry is often compared to art, and this is no coincidence, because the dentist manages to sculpt the smile, to find the right proportions and harmony, in a way that nature (in this case, the parents) failed to do [8].
The Lancet in 1836 offered its readers Lectures on Materia medica and therapeutics, now in course of delivery to Windmill Street Medical School by George G. Sigmond: “The Great and the wise physician, Sydenham, just said, “The art of medicine, if it be a real art, and not barely a name, is the best of all in the world gifts, and so much preferable to all others, as life surpasses all the enjoyments it brings with it.” The investigation of the causes, the progress and termination of disease, - The inquiry into the powers which nature has placed in the hands of man to remedy the deviations from health, form the most interesting occupations of an intellectual being and are objects worthy of the highest degree of mental cultivation” [9-11].
Philosophers and psychologists can confirm with facts that a person's inner beauty, whether he is good and how he treats other human beings, can reflect on the physical (external). That is, physical beauty is a result of our behavior and thoughts. My father often tells my mother that she is very beautiful. She politely tells him that it isn't exactly like that. He is 82 years old, and she is 78. Both have no mental problems, are healthy and have loved each other since childhood. Apparently there is something that makes a person beautiful even as they age. The author admits personal retrospection, but it has been confirmed on a broader, general human level by a number of researchers. The philosopher David Hume (1741) said: “The beauty in things is in the mind that beholds them,” and the writer Margaret Wolfe Hungerford (1878) famously said: “Beauty is in the eye of the beholder” [12-15].
According to the most known and accepted definition for health from the Constitution of the WHO: “Health is a complete state of physical, mental and social well-being, and not merely the absence of disease or infirmity”. Well-being is accepted by scientists as a positive goal or better health in Medicine which follow to higher life-expectancy. Medicine is the science that seeks not only positive health but also aesthetics and harmony in symmetry through numbers. Because the beauty of Medicine is in health. Even with a surgical operation, the seam should be small, symmetrical, in the fold of the body - imperceptible.
In Kenneth Clark's book "Civilization", in addition to the specific tracing of fine arts and detailing of historical features, the development of spiritual culture is also traced. The external world and inner peace are in unity, and fine arts are what manage to recreate harmony and aesthetics. This does not mean, however, that the history of civilization is the history of fine arts and the search for beauty only. Great works of art can be created in barbarian societies. This is the result of the primary limitations of primitive society and this gives a special intensity and vitality to its decorative art. One of the most striking works of art is the sculptural work representing Apollo Belvedere, which to this day arouses the most natural admiration in the world [13].
The modern concept of beauty is very different from Renaissance culture. It offers unified models - perhaps a prelude to clones or a test for society. In fact, dictatorial regimes require students, workers, people, almost everyone to wear uniforms - to be the same and unrecognizable. It is what makes the identity of the person gray and depersonalizes the individual. It is what belittles the power and ability of the person to create, to look for beauty and to be creative for the society.
According to T. Tasevski's monography "Psychology of the Smile in Aesthetic Dentistry", until the 18th century, intellectual notions of the human being were dominated by the dogma that beautiful people are good and ugly people are bad (the main cultural consequences of morphopsychology) and part of the philosophical understanding of ethics [13]. Patients today are extremely concerned about improving their smile and are showing a strong interest in the field of aesthetic dentistry and especially orthodontics. In recent decades, smile design has moved from a two-dimensional approach to a three-dimensional one through computer-aided digitization [8,16-18].
It is debatable whether the mouth or the eyes are the first most expressive feature that each personality carries. The aesthetics of the face achieves its full perfection with the beautiful, pearly smile, which is inherently synonymous with beauty. Of course, the perception of the smile as a universal image requires balanced proportions, and at the same time arouses pleasant feelings [2,3,9,19,20].
The smile is one of the most specific features of the face and the most complex expression of the personality. It is an attribute with universal meaning and power in all civilizational cultures. A beautiful smile can brighten the human face, while an unattractive one can divert the gaze from it. A bright and beautiful smile gives a more youthful appearance, but more importantly, it affects a person's personal self-esteem and self-confidence. A smile leaves the desired impression. Initial perceptions of someone are formed in the first seconds and are based mainly on the emotions experienced [21-25]. In fact, it is not only a beautiful smile that is associated with laughter. Beautiful and attractive teeth are those attributes that make people laugh. They are a particularly characteristic component of the face and cannot go unnoticed.
The orthodontic deviations of world-famous artists such as Julia Roberts, Tom Cruise, Billie Eilish, Miley Cyrus and Zac Efron, etc. do not make them less attractive to people all over the world, on the contrary. They are easily recognizable and liked, and one of the reasons, besides their fame, is the smile "on duty" on their faces.
Aesthetics is one of the greatest achievements of modern dentistry. Achieving its goals requires knowledge from the field of several specialties - therapeutic dentistry; oral surgery; orthodontics; orthopedic dentistry; periodontology and implantology [3,7,8,10,12,16,21,24]. Aesthetic dentistry is based on psychological knowledge, as it is defined as a set of procedures to create harmony between facial features and the mouth, the structure and shape of the gums, the color of the teeth, the angles that form between the cutting edges of the teeth and those of the gingiva, the inclinations, shape and size of the teeth. In this process, the dentist should have the knowledge, skills and attitude to effectively listen and interpret the needs of the patients, and seek a solution for optimal aesthetics [4,6,7,10,15,26-28].
The aim of the current study is to represent the boundaries in esthetics and harmonious perceptions of patient and doctor that can lead to successful orthodontic treatment.
A 12-year-old patient (she is coming alone in the practice) asks the dentist if she can have her permanent upper canines filed down to look more like a vampire. This was very popular among her classmates and she wants to be modern. She has demands on the dentist because the availability of dentists in the area is very high and if he does not fulfill her request, she will go to another dentist.
The doctor is put in a situation where he violates the Hippocratic oath because he damages two permanent teeth by filing them, but he gains the patient's trust and keeps it for his practice or loses it due to refusal.
Which ethical principles are violated and should the patients' demands be met at all costs?
Discussion: Every patient has the right to be informed. Every patient has the right to be treated. Part of the problem in communication is that the information that the doctor has to be shared with the patient within 15-20 minutes, which is considered an effective consultation. Even if it is longer, it will not be essential and the doctor will take the necessary time to make sure that the patient has understood the information provided. The point is that the information that the doctor possesses as knowledge is built during his studies, specialization, courses, seminars, scientific literature and everything else and it must not only be shared, but also understood by the patient to end with informed consent. This casuistry exists when the patient has adequate questions.
When the patient does not have adequate questions, but unusual demands on the doctor, the best solution is to refuse the patient and increase his health culture with additional information, such as that these are irreversible dental damage. When the patient is under 18 y.old,, contact is sought with the parents and the issue is discussed with them. In such cases, children do not discuss their understanding of a beautiful smile with parents and it is entirely possible that they will have legal claims against the doctor if he has allowed himself to file the teeth. The dentist will be subject to legal liability for causing average bodily harm.
The most common advice to young doctors who cannot make an ethical decision is to accept the patient as a very close person whom they would not harm under any circumstances. The other option is to discuss the case with a colleague who is more experienced.
The second ethical case consider the role of the dentist and and although the agreement to fulfil the patient lips with more than 1ml of hyalluronic acid. It follows to the disturbance of the harmony in the society.
Discussion: Although, the dentist is an individual who educate patients in health culture and harmony. In this case the doctor shouldn’t accept the patient request.
872 patients were examined to assess the aesthetic needs for orthodontic treatment in children and adults during a sociological survey. They differ in their orthodontic needs. The patients differ also in their understanding of beauty. Some of them had unusual requests to the orthodontist. Children (n=260) participated in the study with an average age of 12.56 ± 3.14 years, respectively 12.38 ± 3.22 years for boys and 12.69 ± 3.07 years for girls, P>0.05. The number of adult patients who participated in the study was n=612. At the age of 36-40 years, the sex distribution was 32.39 ± 3.21% for women and 9.39 ± 2.0% for men, P<0.05 (u=14.60). Data are presented at Figure 1:
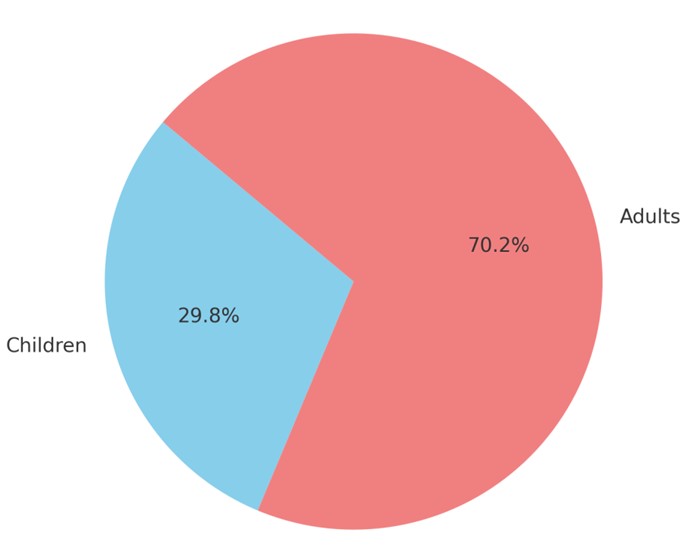 Figure 1: Distribution of patients examined (children vs adults are less, P<0.005).
Figure 1: Distribution of patients examined (children vs adults are less, P<0.005).The distribution of children and adults in the study shows that the number of adults studied (612 participants) significantly exceeds the number of children (260 participants), P<0.005. This distribution is adequate because a child has two parents.
According to literature, the age of the child's first orthodontic examination is essential, as jaw deviations, asymmetry, disorders in facial proportions and balance can be predicted very early. In addition, the history takes data that are relevant and allow the orthodontist to refer the patient to other specialists, for example, otolaryngologist, physiotherapists, neurologists, psychologists, speech therapists, etc [6,20,27,28].
By using a sociological method of straight-group questionnaire the subjects have been asked to consider socio-demographic characteristics, oral health culture, the necessity of prophylaxis and their attitudes for the improvement of function and esthetics during orthodontic treatment. In order to objectify the results, a numerical scale - Visual Analogue Scale (VAS) was introduced [12,14,19,23,29-31]. In the present study, professional and patient’s opinion were compared also and esthetic assessment was provided by using the Visual Analogue Scale.
The whole range 0-100 points has been divided into the following assessment groups:
Statistical data are discussed by means of variation and nonparametric analyses. Findings and graphics are presented by computer software programs SPSS ver. 23.
The gender distribution of the two groups, children and adults, is presented in Figure 2.
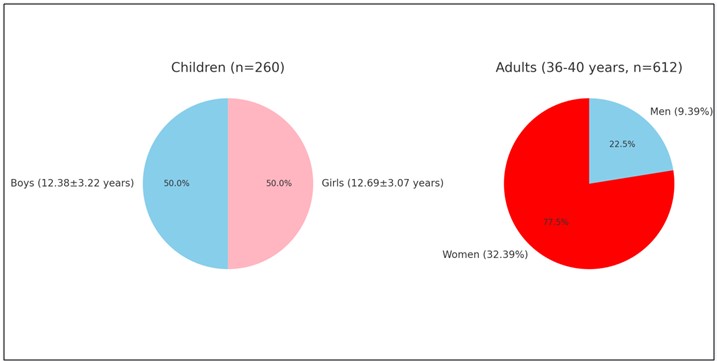 Figure 2: Even gender distribution in children, Females predominate in adults, P<0.05.
Figure 2: Even gender distribution in children, Females predominate in adults, P<0.05.The first pie chart presents the distribution of boys and girls among children (n=260), and the other shows the gender distribution among adults (n=612), P<0.05.
When discussing the strange requests and unusual questions from the patient, a shift in the boundaries of the patient's perceptions regarding aesthetics is observed, P<0.05. Aesthetics are educated. In the family, at school, by the dentist, by society. However, the process is not unambiguous. It goes both ways.
Will parents let their child bring them up? Will school administrators let children grow up unruly? Will a dentist give in to every whim of his patients? Will society be left to bullies?
Patient-dentist communication is often put to the test. The factors are many. They can be socio-economic, educational, behavioral, emotional, even a result of social media. Usually, the patients are proned to believe their friends, stories, FB, forums even thoughtoday they can ask chatgpt but not their dentist. Figure 3 presents the questions asked to the dentist, divided according to their unusualness:
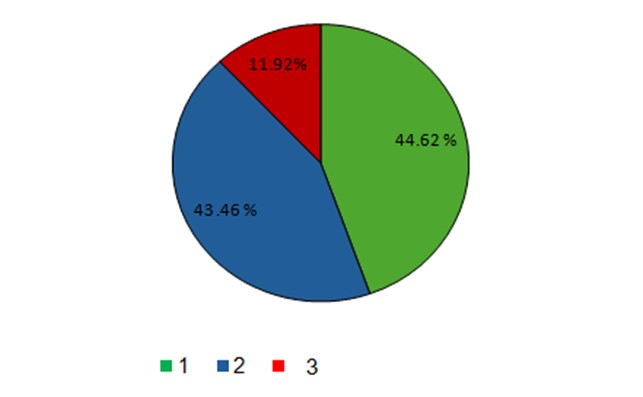 Figure 3: The correct questions that patients ask are marked with the number (1) and colored green; The strange questions of the patients are colored blue (2); and the unusual requests are colored red (3).
Figure 3: The correct questions that patients ask are marked with the number (1) and colored green; The strange questions of the patients are colored blue (2); and the unusual requests are colored red (3).The effective communication with the patient means that the doctor should be serious and calm when hears some strange or even though fanny questions from the patient. Table 1 and Figure 3 present the distribution of patients on these issues and unusual requests in the context of orthodontic examination:
Table 1: Relative parts of children, according to some questions and unusual requests they have.|
Relative parts of patients according to |
Number (n) |
% |
Sp |
|
Correct questions |
116 |
44.62 |
3.08 |
|
What did you say? |
113 |
43.46 |
3.07 |
|
Unusual request |
31 |
11.92 |
2.01 |
|
Total |
260 |
100.0 |
- |
The largest group is the group of patients asking the right questions (44.62%). This indicates good information and effective communication with the dentist. The group asking strange questions is very large also and approximately equal to the first (43.46%). This tendency to misunderstanding may be due to insufficient precision, lack of information or preparation, communication barriers or confusion following prior questioning of classmates or friends about orthodontic treatment [30].
Some of the strange questions are: "I want to have a dental unit like this at home. How much does it cost?", "My daughter's hair is dripping. Is it from the braces?", "Can you put braces on my dog?", "Can I keep the teeth you pulled out of my mouth? I would like to make a necklace out of them.", "Please, close my mouth to help me with diet.", etc. The estetics and harmony in orofacial complex is evaluated by the doctor and selfesteemed perceptions are presented in Table 2.
Table 2: Malocclusion level and self-assessment by the child.|
Self-assessment Scale |
Malocclusion level |
|||||||||||
|
Mild |
Average |
Severe |
Total |
|||||||||
|
n |
% |
Sp |
n |
% |
Sp |
n |
% |
Sp |
n |
% |
Sp |
|
|
Poor |
2 |
1.52 |
1.06 |
7 |
7.22 |
2.63 |
3 |
4.17 |
4.08 |
12 |
3.95 |
1.22 |
|
Average |
43 |
32.58 |
4.08 |
34 |
35.05 |
4.84 |
12 |
45.83 |
10.17 |
89 |
34.78 |
2.99 |
|
Well accepted |
89 |
65.91 |
4.13 |
56 |
57.73 |
5.02 |
12 |
50.00 |
10.21 |
159 |
61.26 |
3.06 |
|
Total |
134 |
100.0 |
- |
97 |
100.0 |
- |
29 |
100.0 |
- |
260 |
100.0 |
- |
The clinical approach alone is insufficient and it is obvious that the need for orthodontic treatment should also be based on the patient's opinion. Identification of a malocclusion is a major factor in motivating an individual to seek orthodontic services. Nevertheless, it is important to discuss both the functional and aesthetic factors that determine the treatment. The subjective assessment of the patient at the beginning is very important for the treatment, because if the patient is not satisfied at the end, all the accompanying efforts remain unsuccessful. There are several subjective tools used in analysis that emphasize the patient's self-assessment and self-perceptions. These are IOTN (Index of Orthodontic Treatment Need), DAI (Dental Aesthetic Index), OASIS (Orthodontic Aesthetic Subjective Impact Scale), ICON (Index of Complexity Outcome and Need) and VAS (Visual Analogue Scale), Figure 4 [7,22,24,26].
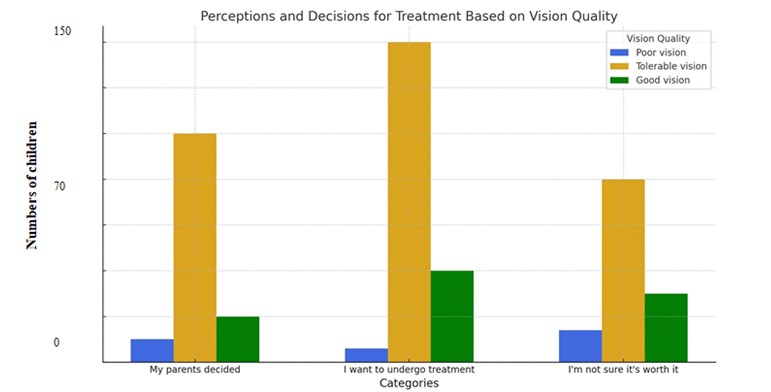 Figure 4: Perceptions and treatment Decision making capacity.
Figure 4: Perceptions and treatment Decision making capacity.Two factors were extracted as significant for aesthetics according to the respondents. For this purpose, Principal Component Analysis – PCA was used and the patient's expectations at the first orthodontic consultation were analyzed and compared with those achieved at the end of treatment when the braces were removed. At baseline, the statements “I want to have straightened teeth”, “My parents want them, I don’t want to wear braces” and “I don’t like my teeth look” had the highest correlation coefficients, respectively rxy=0.90, rxy=0.87, rxy=0.83. In the final stage of treatment, the children’s opinions focused on the long-term benefits of orthodontic treatment. “I want to be more confident”, “I want to have a lot of success in the future because I can smile more now”, “My teeth will be healthier because they are straight and I know how to clean them”, respectively rxy=0.93, rxy=0.90, rxy=0.88. Factorial signs in the perception of function and aesthetics in the maxillofacial region were evaluated. Data are presented in Table 3:
Table 3: Checking the adequacy (applicability) of factor analysis using KMO and Bartlett's Test in children.|
Adequacy Test - КМО (Kaiser-Meyer-Olkin Measure of Sampling Adequacy) |
0.553 |
|
|
Bartlett's Test of Sphericity |
Approx. Chi-Square |
1262.02 |
|
df |
406 |
|
|
Sig. |
0.001 |
|
Social medicine is the unifying link between the patient's (subjective) and the doctor's (objective) understandings of disease or condition (beauty). Awareness is that stone "that can overturn a car on the road." Inappropriate (such as age, gender, social group) awareness can affect the psycho-social perception of the problem and create complexes in the patient's perception. This process is particularly noticeable when evaluating the aesthetics of the orofacial complex. In fact, one of society's expectations from the dentist is to educate. To educate in aesthetics and beauty through his work. And to manage patient’s perceptions what is good or bad in facial esthetics. The role of the dentist and orthodontist today is very special. This is the bone between society’s expectations aand health culture of the patient. More than ever there is a need to be teached in harmony and esthetics.
We would like to thank all parents who participated in this sociological study. The author is grateful for the reviewer’s comment that improved the manuscript.
None declared.

