 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Guzmán-Casta Jordi1,2*, Riera-Sala Rodrigo Fernando1, Martínez-Vega Rocío Pamela5, Rubio-Cordero Jairo Aaron2, Téllez-CamposcLucía2, Baltazar-Contreras Rocío del Carmen2, Carrasco-Cara Chards Sonia3, Guzmán-Huesca Jorge4, González-Araujo Andrea6, Hernández-Dehesa Itzel Ariadna7, Domínguez Ayala Adriana10, Correa-Cano Rafael9
, Elvira-Fabián Karina8, Escobar-Gómez Mario2, Lázaro-León Jesús Miguel2
1.Department of Clinical Oncology, Instituto Nacional de Enfermedades Respiratorias, Ciudad de México, México.
2.Department of Clinical Oncology, Hospital General de México “Dr. Eduardo Liceaga”, Ciudad de México, México.
3.Facultad de Medicina, Universidad Nacional Autónoma de México, Ciudad de México, México.
4.Bonita Community Health Center, Internal Medicine, Bonita Springs, Florida, United States
5.Nutritional Department, Hospital General de México “Dr. Eduardo Liceaga” Ciudad de México, México
6.Resident of Primary Care, Instituto del Seguro Social “IMSS”, Guanajuato, México
7.Department of Radiology, Hospital Ángeles Acoxpa, Ciudad de México
8.Centro Médico Hospital ABC Santa Fé, Ciudad de México, México.
9.Resident of Clinical Oncology, Centro Médico Nacional Siglo XXI “IMSS”, Ciudad de México, México.
10.Department of Radiooncology, Centro Médico Naxcional 20 de Noviembre “ISSSTE”, Ciudad de México, México
Correspondence to: Guzmán-Casta Jordi, Department of Clinical Oncology, Instituto Nacional de Enfermedades Respiratorias, Ciudad de México, México.
Received date: November 22, 2020; Accepted date: December 6, 2020; Published date: December 13, 2020
Citation: Jordi GC, Rodrigo FernandoRS, Rocío Pamela MV, et al. (2020) Microsatellite Instability Incidence in Recurrent Colon Cancer Stage II and III. J Med Res Surg 1(6): pp. 1-5. doi:10.52916/jmrs204034
Copyright: ©2020 Jordi GC, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Objective: To evaluate the incidence of Microsatellite Instability (MSI) in patients with Colon Cancer in stage II & III in the Mexican population.
Methods: This is a descriptive, retrospective and cross-sectional study performed through a review of 30 clinical charts of patients with the diagnosis of Colorectal Cancer and evaluation of Microsatellite Instability in surgical pathology specimens.
Results: Males with 53.3% had a higher incidence than females. The most frequent site was the left colon (53%), followed by the right colon (16.6%), higher rectum (10%), mid rectum (10%), and lower rectum (10%). The majority of the patient were classified as moderately differentiated (86.7%), with 6.7% being poorly differentiated and the rest 6.7% well differentiated. For the presence of MSI in repair genes (MLH1, MSH2, PMS2), this was positive in 33% of the population studied. The clinical-stage most frequently affected was IIA with 36.7% of the positive cases followed by stage IIB with 20%, stage IIIA 20%, and finally, stage IIC and IIIB with 13% and 10% respectively. Among histologic subtypes, adenocarcinoma was found in 90% of the cases, mucinous carcinoma in 6.7%, and signet ring cell carcinoma in 3.3%. In regards to treatment, 50 % of patients underwent only surgery while the other 50% were treated with surgery followed by adjuvant chemotherapy. Clean surgical margins were achieved in 93.7% after initial surgery and the rest were taken back to surgery for a wider resection. The predominant tumor size was T2 (50%), T3 (33%), and T4a (16.7%). The most commonly found lymph node involvement was N1a with 63.3% of the cases followed by N1b with 16.7%. In terms of recurrent metastatic disease, M1a was the most frequent, found in 73.3% of the cases.
Conclusion: In our study population in contrast with current literature from the rest of the world we found a higher presence of microsatellite instability (33% vs 15%) and a higher incidence in the left colon with a definitive impact in the survival of patients.
Colon cancer recurrent, Microsatellite instability, Stage II, Stage III.
Colorectal Cancer (CRC) is the third most common malignancy in the western world and the second most common cause of cancer death in North America. It presents as a heterogeneous disease at the molecular level. Several studies have evaluated the different molecular subtypes, histopathology classification and clinical characteristics of CRC, finding the Microsatellite Instability (MSI) as a biological factor determining prognosis and treatment. Four Consensus Molecular Subtypes (CMS) in Colorectal Cancer (CRC) were identified in a study by Justin Guinney. MSI was the main characteristic for CMS1 (Immune Hypermethylation and an important activation of the immune system) [1-3].
The most common presentation is sporadic (85%) or associated with Lynch Syndrome (Hereditary Non-Polyposis Colon Cancer). The majority of cases occur as a consequence of sporadic methylation of hMLH1 (95%-97%). The MSI-H phenotype is an identity seal of CRC associated with Lynch Syndrome and it is diagnostic of it [4-6].
Microsatellites are small repetitive Deoxyribonucleic Acid (DNA) sequences from 1 to 6 bases distributed along the genome in both coding and non-coding regions. Microsatellite Instability (MSI) is a molecular change particularly distinctive in approximately 15% of the case of Colorectal Cancer [7,8].
Since 1998, we have learned that patients with high Microsatellite Instability (MSI-H) show a different clinical behavior, less aggressive course and a more favorable prognosis compared to the rest of the patients. It was Ribic et al. who initially described how patients with MSI-H tumors had a modestly better prognosis than those with tumors showing low microsatellite instability [9,10].
The molecular cause in Colorectal Cancer with MSI-H is a deficiency in the DNA Mismatch Repair (MMR). MLH1 and MSH2 genes are inactivated in 90% of Colorectal tumors with MSI. In the sporadic tumors, the inactivated gene is MLH1 and in more than 80% of the cases, this inactivation is produced by methylation of the promoter [11,12].
The MSI-H phenotype shows an association with a more proximal localization of the tumor, an important infiltration of lymphocytes, and a low incidence of distant metastasis. These MSI-H sporadic tumors typically develop in the proximal colon and have a female preponderance. In young patients presenting with Colorectal Cancer, the MSI-H phenotype is closely associated with Lynch Syndrome [13,14]. One of the histopathologic characteristics of MSI-H colorectal cancer is a high density of lymphocyte infiltration of the tumor. They generally have a mixed differentiation encompassing subtypes like signet ring cells, mucinous and medullary carcinoma. The evidence has shown that mutations in the Beta-2-Microglobulin (B2M) are associated with an absence of distant metastasis in patients with MSI-H Colorectal Cancer [15-17].
Recent independent studies have demonstrated that patients with a mutated B2M gene in MSI-H CRC have a remission free survival significantly longer compared to patients with a nonmutated B2M MSI-H Colorectal Cancer [18]. In recent years, the hypothesis that patients with MSI-H CRC show a decreased sensitivity to 5-Fluorouracil chemotherapy has been supported by various studies, including in vitro studies, experimental studies in mice and other clinical assays. MSH-1 Colorectal Cancer has a better prognosis than CRC with microsatellite stability. It’s been suggested that such prognosis has to do with malignancies associated with Lynch Syndrome and therefore a higher antitumor immune response [19,20].
The hypothetical predictive role of MSI with the response to 5-Fluorouracil based adjuvant chemotherapy has proven to be a rather more difficult topic to sort out. Adjuvant chemotherapy in patients with Stage II CRC is still a controversial topic. In a 2011 article by Sinicrope et al. about 2141 patients with CRC they found a benefit with 5-Fluorouracil in patients with MSI in Stage II cancers compared to other studies reported in the literature [5,21,22].
In Clinical Stage II tumors are highly heterogeneous with 5-year overall survival rates ranging from 58.4% to 87.5%. The European Society of Medical Oncology recommends that MSI should be evaluated in Stage II CRC to help with treatment and make decisions with regards to the administration of adjuvant chemotherapy [23-24].
Figures 1-11 showing the results of the study (Stage II) was the most commonly found and where there was a higher recurrence rate, for that reason 50% of patients underwent surgery without adjuvant chemotherapy which has been demonstrated in the previous series and in the literature that the presence of risk factors including MSI is frequent in recurrent cases and sensitive to the use of Fluoroprymidine based chemotherapy, for that reason the group of non-adjuvant therapy was classified as of high risk for recurrence without taking into account other associated risk factors.
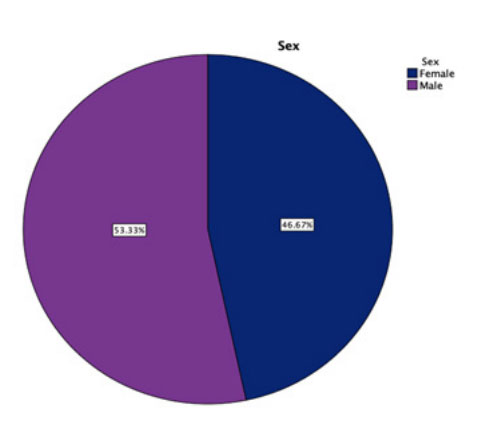 Figure 1: The incidence was minimally higher in men by 53.33% versus
46.67% in women.
Figure 1: The incidence was minimally higher in men by 53.33% versus
46.67% in women.
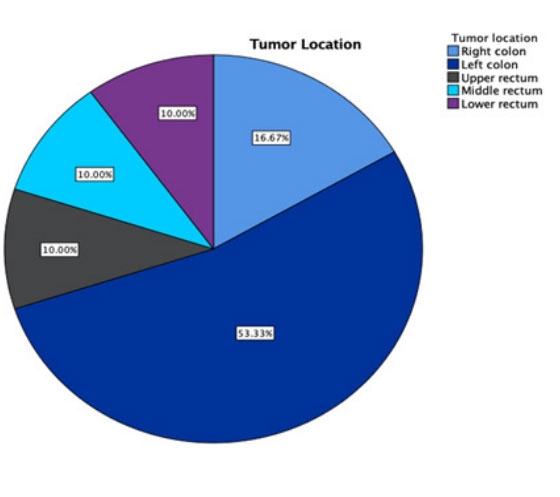 Figure 2: More than half of the patients evaluated had a tumor location in
the left colon 53.33%.
Figure 2: More than half of the patients evaluated had a tumor location in
the left colon 53.33%.
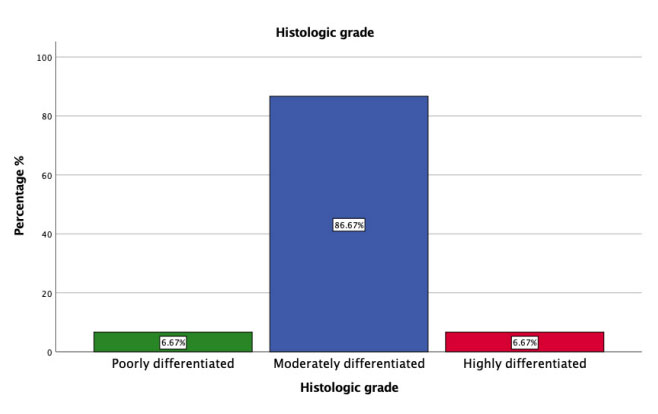 Figure 3: Up to 83% of tumors were moderately differentiated
adenocarcinomas.
Figure 3: Up to 83% of tumors were moderately differentiated
adenocarcinomas.
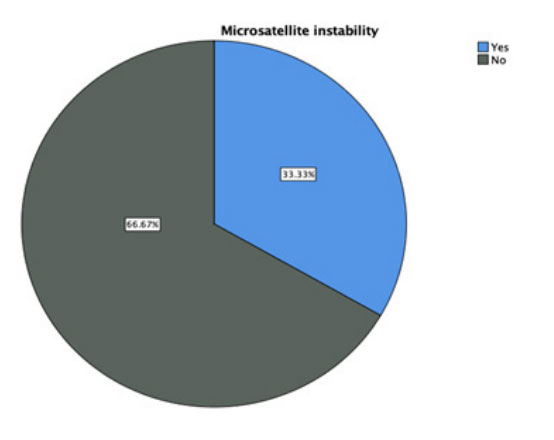 Figure 4: The incidence of microsatellite instability was 66.7% in recurrent
tumors.
Figure 4: The incidence of microsatellite instability was 66.7% in recurrent
tumors.
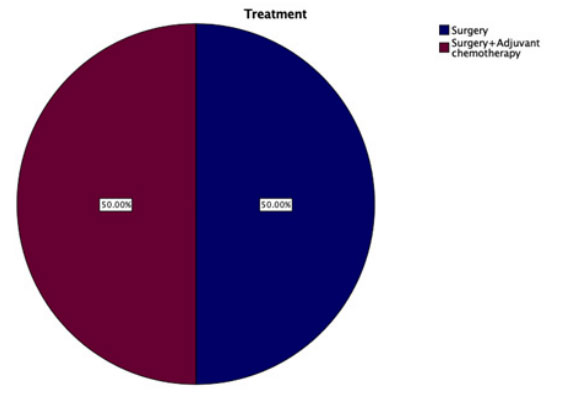 Figure 5: Half of the patients were only taken to surgery and the other half
was added adjuvant chemotherapy
Figure 5: Half of the patients were only taken to surgery and the other half
was added adjuvant chemotherapy
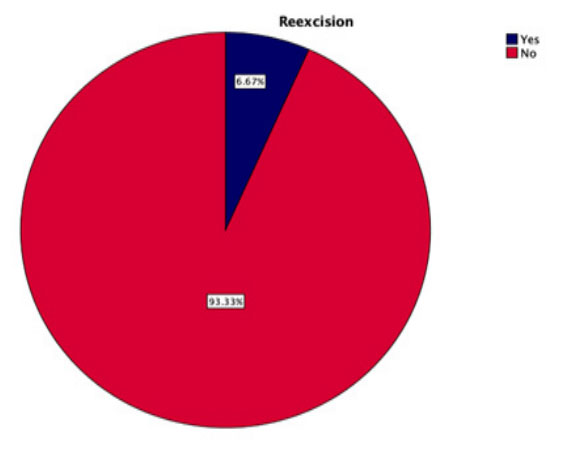 Figure 6: Because the initial surgery was not addressed by oncologist
surgeons, reoperation had to be performed in 6.67% of the patients.
Figure 7: The most prevalent clinical stage was IIA in our patients
Figure 6: Because the initial surgery was not addressed by oncologist
surgeons, reoperation had to be performed in 6.67% of the patients.
Figure 7: The most prevalent clinical stage was IIA in our patients
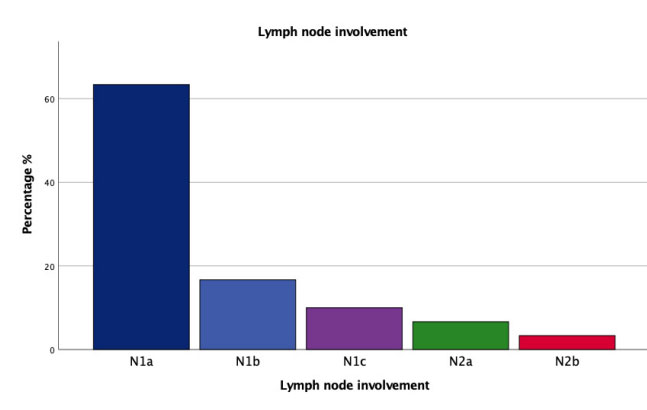 Figure 8: The incidence of lymph node involvement was greater than 60% in
the postsurgical evaluation.
Figure 8: The incidence of lymph node involvement was greater than 60% in
the postsurgical evaluation.
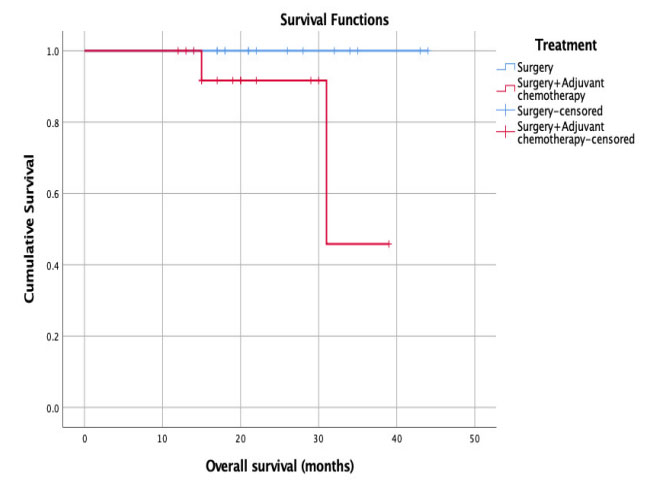 Figure 9: We observed that in the global survival follo w-up to more than 40
months, 100% of the patients who only underwent surgery were still alive.
Figure 9: We observed that in the global survival follo w-up to more than 40
months, 100% of the patients who only underwent surgery were still alive.
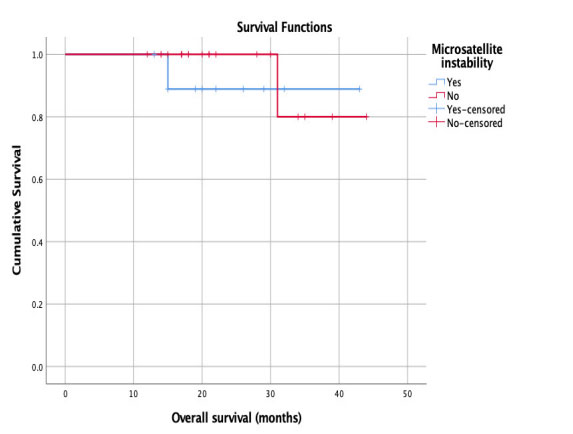 Figure 10: Patients who had microsatellite instability had higher overall
survival than those who did not present it.
Figure 10: Patients who had microsatellite instability had higher overall
survival than those who did not present it.
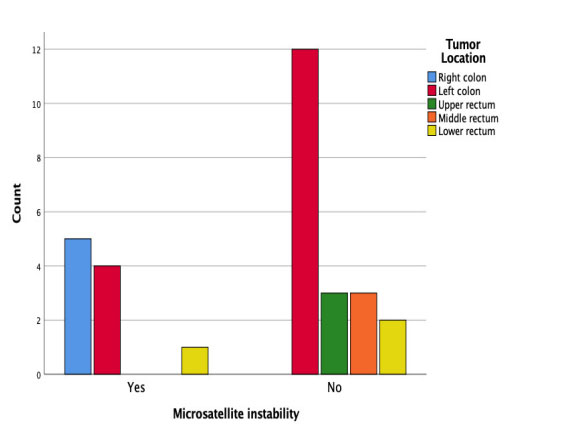 Figure 11: We found that the greatest presence of microsatellite instability
was in the left colon.
Figure 11: We found that the greatest presence of microsatellite instability
was in the left colon.
We can conclude that the population evaluated in our Hospital exhibited a different behavior than the one evaluated previously in the series reported worldwide in the literature. We observed a higher presence of microsatellite instability MSI and a higher prevalence of the tumor in the left colon as compared to the right colon with a higher risk as an independent factor for recurrence without taking into account the size of the tumor or the lymph node involvement that was reported in more than 60% in our series, the elevation of ACE levels and the fact that half of the patients did not receive adjuvant chemotherapy with Fluoropyrimidine which further increases the risk of recurrence, and finally the presence of Microsatellite Instability had better overall survival. The testing for the presence of satellite instability in tumor tissue should be a new standard to evaluate the prevalence and risk of recurrence.

