 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Hrishikesh S. Saodekar1, Amogh S. Bubna1, Yogesh Salphale2* , Ganesh N. Pundkar1, Rajendra W. Baitule1, Sanjeev V. Jaiswal1, Aman S. Rathod1
, Ganesh N. Pundkar1, Rajendra W. Baitule1, Sanjeev V. Jaiswal1, Aman S. Rathod1
1Department of Orthopaeedics and Traumatology, Dr. P.D.M. Medical College, Shivaji Nagar, Amravati, Maharashtra, India.
2Consultant Trauma and Orthopaedic Surgeon, Shushrusha Hospital, Lane Opp. Z.P, Chandrapur Maharashtra, India.
Correspondence to: Yogesh Salphale, Consultant Trauma and Orthopaedic Surgeon, Shushrusha Hospital, Lane Opp. Z.P, Chandrapur Maharashtra, India.
Received date: September 7, 2024; Accepted date: September 21, 2024; Published date: September 28, 2024
Citation: Saodekar HS, et al. Management of Complex Pelvic Fractures Associated With Acetabulum Injury: Case Series. J Med Res Surg. 2024;5(5):110-115. doi: 10.52916/jmrs244148
Copyright: ©2024 Saodekar HS, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Comprehensive emergency management and early stabilization are pivotal in treating complex pelvic and acetabular fractures. Surgical treatment of displaced Pelvi-acetabular fractures has evolved from conservative to operative treatment. In the current study, we presented a series of thirty cases involving complex pelvic fractures as well as acetabular injuries, emphasizing the significance of comprehensive emergency management and appropriate intervention. As a result of the present case series, we highlight, the crucial role of a comprehensive operative plan that differentiates among patients based on their general condition, the available resources and the surgeon's preference. Central to our approach was the utilization of the Stoppa and Kocher-Langenbach techniques for internal fixation, demonstrating their efficacy in addressing these challenging fractures. The findings of the current series, reveal that, the functional outcome correlated well with the quality of reduction. Also, we recommended that the Stoppa and Kocher-Langenbach techniques be used as an effective treatment approach to address these complex fracture’s.
Pelvic fracture, Stoppa and Kocher-Langenbach techniques, Harris Hip Score (HHS), Reduction and internal fixation, Acetabulum injury.
Orthopedic surgeons face significant hurdles when it comes to dealing with acetabular and pelvic ring fractures. Due to the steep learning curve involved, only well-established reference centers with ample resources and expertise may have the equipment to effectively handle and treat these complex fractures [1]. As high-energy injuries become more prevalent, acetabular and pelvic ring fractures are frequently encountered in polytrauma patients. It is worth noting that up to 61.7% of individuals with pelvic ring injuries are victims of multiple injuries, and among these cases, 12.2% also exhibit concurrent soft tissue injuries [2]. The mortality rates associated with pelvic ring fractures vary considerably, ranging from 7% for isolated injuries to as high as 31.1% when severe soft tissue damage is involved. Furthermore, the mortality rate rises to 13% when a pelvic ring fracture is coupled with an acetabular fracture. Consequently, the decision-making process regarding prompt and suitable management, particularly in the case of polytrauma patients, carries significant weight. Even though achieving success during the acute phase of treatment is crucial, it is an even more formidable challenge to predict the long-term functional of the preserved limb and hip joint.
Current trends in the treatment of acetabular fractures involve open reduction and internal fixation [3], following principles applicable to all intra-articular injuries. Judet et al. [4], established the classification and operative management principles in the 1960s. Similarly, pelvic ring injuries are mainly based on Marvin Tile’s classification system from 1980[5]. These both classification systems are still widely used in the 21st century for decision-making and guidance of therapeutic protocols in the acute management of patients with pelvic ring disruptions. Long-term follow-up studies by Kebaish et al. [6], suggest superior results with surgical treatment (80% satisfactory) compared to non-operative treatment (30% satisfactory) for displaced acetabular fractures. In the current case series, we extended this understanding by presenting oneyear results (February 2022 to February 2023) and followed up for atleast a year and functional outcomes following surgical treatment across varied presentations of displaced acetabular fractures.
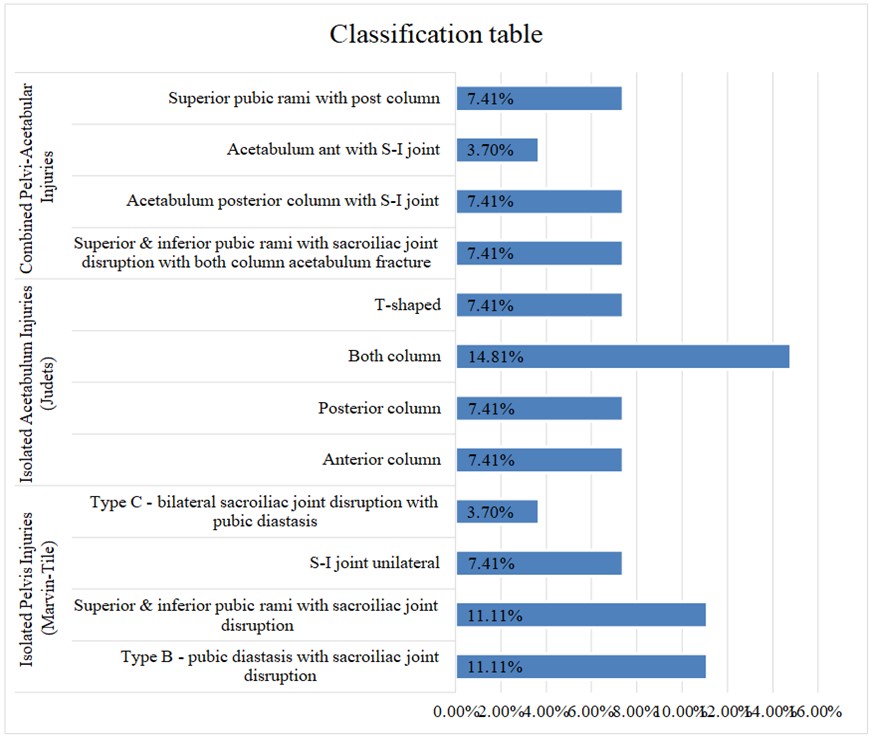 Figure 1: Showing the classification of injuries of the pelvis and acetabulum.
Figure 1: Showing the classification of injuries of the pelvis and acetabulum.The surgical procedure commenced with the administration of general anesthesia. Standard disinfection protocols were followed. For the Stoppa’s approach: Following successful anesthesia, patients were positioned supine, with slight hip and knee in flexion. Then, following the incision of skin and subcutaneous tissue, a longitudinal incision was made in the linea alba, allowing lateral displacement of the rectus abdominis while preserving its endpoint. Subsequently, lower abdominal wall muscles, external iliac blood vessels, femoral nerves, and iliac and lumbar muscles were anteriorly and laterally mobilized, shifting extraperitoneal pelvic organs posteromedially. This approach was primarily used for hernia repair since 1975 which was modified in 1994 to used by orthopaedic surgeons using the Pfannenstiel incision to approach the pubic symphysis and the anterior column along with a lateral window which allowed excellent visualization of the quadrilateral plate. Special attention was paid to the identification and management of anomalous vascular extraperitoneal communication branch, notably the "corona mortis" artery. The inferior epigastric or iliac vessels provide development to the surface of the superior branch of the pubis, where the corona mortis anastomoses with the obturator artery in close proximity to the obturator foramen.
For patients with double-column fractures, treatment involved a combination of the posterior K-L approach with the Stoppa’s approach.
In the present case series reduction of fractures was facilitated using instruments like Bucking Bars and pelvic fracture reduction forceps, sometimes accompanied by lower limb traction as and when required. Fracture fixation involved screws, Kirschner wires, and steel plates placed strategically in the true pelvis entrance and, when necessary, in the arcuate line. In cases of sacroiliac joint or ilium fractures, reduction and fixation was done using a lateral window, along with the stoppa’s approach (Figure 2). For double-column fractures, the posterior column was reduced and fixed using the K-L approach in the lateral position, following reduction of the anterior column through the extended Stoppa approach.
 Figure 2: Showing both column fracture.
Figure 2: Showing both column fracture.In this case series, functional outcomes were assessed using the Harris hip score. Among the cases, 6 (24%) achieved an excellent outcome, and 11 (44%) achieved a good outcome. Additionally, 5 (20%) cases were categorized as fair, while only three cases (12%) had a poor outcome attributed to incongruent reduction. Scores in the Merle d’Aubigne score range from a maximum of 11 (44.00%) to 1 for excellent, good, fair, and poor, which are represented as 6 (24%), 7 (28%) and 1 respectively, as shown in Table 1 and Figure 3.
Table 1: Showing functional outcome based on Merle d’Aubigné score.|
Pelvic outcome |
Patients (%) |
|
Excellent |
11 (44.00%) |
|
Good |
6 (24.00%) |
|
Fair |
7 (28.00%) |
|
Poor |
1 (4.00%) |
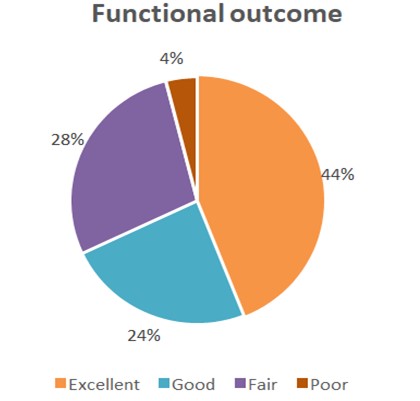 Figure 3: Showing functional outcome based on Merle d’Aubigné score.
Figure 3: Showing functional outcome based on Merle d’Aubigné score.Pelvic ring injuries and acetabular fractures, or a combination of both, result from high- energy trauma, and are often displaced to such an extent that surgery is inevitable [7]. The patient's physiological condition serves as the primary determinant for the definitive management of pelvic fractures, although effectively timing the management of concomitant injuries presents a significant challenge. Timely fixation of fractures is widely acknowledged as a key factor in reducing complications and mal-union rates.
In our ongoing case series, we have seen that even though the perfect anatomical reduction may not be achieved a normal functional outcome for the patient is possible.
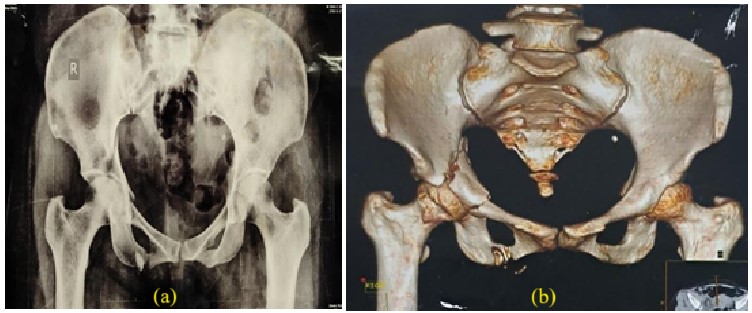 Figure 4(a,b): Showing the central hip dislocation with fracture of medial wall of acetabulum right side.
Figure 4(a,b): Showing the central hip dislocation with fracture of medial wall of acetabulum right side.One case with fracture acetabulum left, left hip central dislocation (Figure 4) and another case of pubic diastasis and sacro-iliac joint disruption with fracture acetabulum right (Figure 5). In these cases, surgery was performed using the Stoppa and Kocher- Lagenbach approaches and open reduction with plating. The choice of approach was based on pre decided protocol, which took into consideration which of the two columns was maximally displaced. We first fixed/stabilized the acetabular injury when indicated. The surmise being the restoration of the hip joint articulation and joint surface is supposedly better. However stability of the pelvic ring is more important than the anatomical reduction in helping the functional outcome.
As in the above mentioned case with central hip dislocation it was decided to provide the same patient with a 21-day course of lateral traction post fixation was done for added stability as there was a delay in fracture fixation due to the low general condition of the patient, so to attempt to obtain a normal functional outcome for the hip. After three months, the patient showed satisfactory recovery, with significant improvement in functional ability, as represented in Figures 5 and 6. Figure 5: Showing percutaneous cc screw with plating for the anterior column.
Figure 6(a,b): Showing immediate post-operative x-ray and with lateral traction.
Figure 5: Showing percutaneous cc screw with plating for the anterior column.
Figure 6(a,b): Showing immediate post-operative x-ray and with lateral traction. There have been multiple attempts in the past to use a single approach to tackle complex fractures of the acetabulum. Xue et al. [10], used a pubic symphysis approach (Pfannenstiel incision) to treat a series of 15 patients with acetabular fractures. Being minimally invasive, this approach had better outcomes in terms of approach-related morbidity.
In fractures involving the sacro-iliac joint or having sacro-iliac joint disruption resulting due to vertical shear forces, which caused a S-I joint disruption with pubic diastasis, percutaneous cc-screw was inserted into the sacrum and plating done for the pubic diastasis. Anatomical reduction was achieved with a single incision and a percutaneous screw into the sacrum. Here the fixation of the posterior segment i.e. the sacro-iliac joint is done first, which we observed aided in the stability of the pelvis for the fixation of the pubic diastasis, to help us achieve an anatomical reduction (Figure 7).
 Figure 7: Showing 3 months post-operative.
Figure 7: Showing 3 months post-operative.However, the requirement of an additional Kocher-Langenbeck approach in more than 50% of the study population again showed the inadequacy of any single approach.This showed that injuries are associated to occur together involving multiple columns which require different approaches for effective fixation In alignment with the findings of Suzuki et al. [11], who recommend employing the Stoppa’s approach for pelvic fractures, enabling reduction from within the pelvis by utilizing the remaining capsular attachment to facilitate anatomical reconstruction of the anterior column. Some cases required an anterior as well as a posterior incision for a single column fracture along with bilateral sacro-iliac joint disruption (Figure 8). Firstly the sacro-iliac joints were stabilized with plating and a cc-screw which helped in the stability of the pelvis, thereby making the fixation of the acetabular wall easier and to maintain an anatomical reduction.
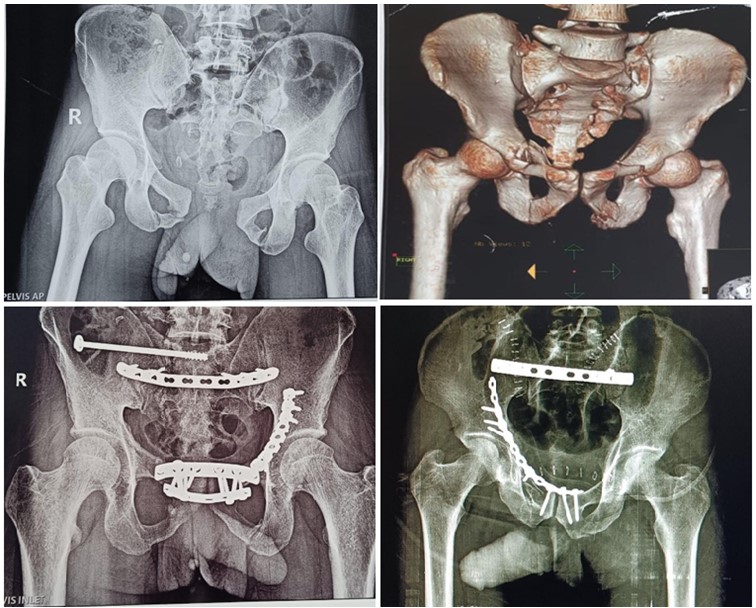 Figure 8: Showing posterior incision with plating of bilateral S-I joint.
Figure 8: Showing posterior incision with plating of bilateral S-I joint.This approach aligns with the insights of Hirvensalo and Lindahl [12], particularly in both column fractures, emphasizing that the reduction and fixation of the anterior column should commence from the most cranial area. Furthermore, the utilization of the anterior intrapelvic (modified Stoppa) approach with lateral window for treating acetabular fractures not only allows for excellent reduction in the majority of cases but also provides exceptional visualization and access to the quadrilateral plate, a technique supported by Sagi et al. [13].
This case series shows that radiographic congruency correlated well with functional scoring (p<0.05). Similarly, the assessment of functional outcomes using the Merle d’Aubigne score revealed 11 cases were having excellent, resulting in a high level of functional recovery and patient satisfaction. Six cases were rated as good, which represented satisfactory functional outcomes with minor limitations. Seven cases were categorized as fair, suggesting moderate success with some functional challenges remaining.
In 2021, a study conducted by Fakru NH et al. [14] evaluated 43 patients with isolated acetabular fractures and pelvis fractures was evaluated using the Merle d’Aubigne and Harris Hip Score (HHS), with an average mean of 15.77 and 86.6, respectively. A good correlation was found between the functional results and reduction quality in the current study.
Another standard protocol we used in the study at our institution was to do adequate imaging of the patient using 3D ct scans for a complete imaging of the the pelvis so as to not miss out fractures such as the sacro-iliac joint dissociation which are commonly missed in simple radiographs. We had a high index of suspicion that ,whenever a ring (pelvic ring) is fractured (broken) at one place the ring is bound to fracture at another place unless proven otherwise and most commonly the sacro-iliac joint is affected. Commonly vertical shear fractures were associated with the pelvic ring injuries, (sacro-iliac joint with the pubic rami).
In our case series we used a standard protocol for the fixation after thorough investigation using 3D CT scans to gauge the fracture columns and throughout the case series wherever we encountered multiple column fractures it was decided to fix the acetabular fractures first followed by fixation of the column which was maximally displaced causing. It was also observed that perfect anatomical reduction is not always possible due to various factors; like time to surgery which may result in soft tissue impalement at the fracture site and or fibrous union; osteoporosis, communition and also surgeon experience. A patient operated late (3 weeks after the trauma) had a satisfactory functional outcome after the 1 year follow-up even though anatomical reduction was not perfectly achieved.
Our case series highlights, the importance of a comprehensive evaluation and management approach for acetabulum and pelvic fractures. Early adequate evaluation with 3D CT-scan aids in determining the extent of the injury and guides appropriate treatment decisions which might get missed due to limitations of standard radiographs. The presented patients responded well to the reduction and fixation procedures, demonstrating the potential for functional recovery and ambulation within a reasonable timeframe. The cases operated early had a good functional outcome howsoever a delay to operate the patient due to contributory factors also did not cause a loss of satisfactory functional outcome.This case series contributes to the existing knowledge and emphasizes the significance of proper evaluation and time management in optimizing outcomes for patients with acetabulum and pelvic fractures.
None.
The authors declare no conflict of interest.

