 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
FJ Buils Vilalta1,2*, JJ Sánchez Cano1,2, R Prieto Butillé1, J Menéndez1, MA García1, G Renau1, N Lobo1, S Haupt1, A Sánchez Marín1,2
1Department of General and Digestive Surgery, Sant Joan University Hospital, Reus, Tarragona, Spain
2Rovira I Virgili University, Faculty of Medicine and Health Sciences, Surgery Unit, Tarragona, Spain
Correspondence to: Vilalta FJB, Department of General and Digestive Surgery, Sant Joan University Hospital, Reus, Tarragona, Spain
Received date: October 11, 2022; Accepted date: October 23, 2022; Published date: October 30, 2022
Citation: Vilalta FJB, Cano JJS, Butillé RP, et al. Laparoscopic Approach to Pancreatic Pseudocyst: A Case Report. J Med Res Surg. 2022;3(5): 109-111. doi: 10.52916/jmrs224090
Copyright: ©2022 Vilalta FJB, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted
use, distribution and reproduction in any medium, provided the original author and source are credited.
Pancreatic Pseudocyst (PP) is a local complication due to rupture of the pancreatic duct in acute or chronic pancreatitis, trauma or obstruction of the pancreatic duct. Acute forms usually resolve spontaneously in more than 40% of cases and chronic forms usually do not disappear and are at higher risk of complications. They can be drained by surgical, laparoscopic, percutaneous and endoscopic methods. Percutaneous drainage may lead to an external pancreatic fistula and is not preferred Endoscopic internal drainage of pseudocysts has been shown to be effective and is less invasive compared to open surgery . We present a 70 year old male with a history of several episodes of acute pancreatitis with subsequent residual pseudocyst. Initially, an EUS-FNA/ERCP is performed with aspiration of the pseudocyst. Due to the subsequent recurrence months later, it was decided to consider a laparoscopic approach, to solve the recurrence, performing a laparoscopic cystogastrostomy. Postoperative period was uneventful and was discharged on the seventh post-intervention day.
Gossypiboma, Surgical sponge, Retained, Hydatid cyst, Textiloma
Pancreatic pseudocysts (PPs), common sequelae of acute or chronic pancreatitis and trauma. It is the most common cystic lesion of the pancreas. It is more prevalent in males, between the fourth and fifth decade. It is estimated that their maturation period is approximately 2 to 6 weeks [1,2]. Most resolve spontaneously, although size is the most influential factor (those <5 cm have a lower rate of complications and a higher probability of spontaneous resolution), other factors associated with low resolution can be highlighted, such as; extrapancreatic location, presence of multiple cysts, location in the pancreatic tail, absence of communication with the main pancreatic duct and wall thickness [3]. They generally present as single, however when there is an association with alcohol they are multiple. Its size is variable, being able to measure up to 30 cm. With the advent of minimally invasive techniques such as cystograstostomy, cystojejunostomy and cystoduodenostomy [4], Laparoscopy plays a great role in the management of PPs. Moreover, laparoscopic cystogastrostomy has been described as a safe and efficacious alternative to open drainage of PPs in adults [1,2]. We report a patient with multiple comorbidities with symptoms of pancreatitis of biliary origin with subsequent development of a pancreatic pseudocyst in whom surgical resolution was decided with a laparoscopic approach.
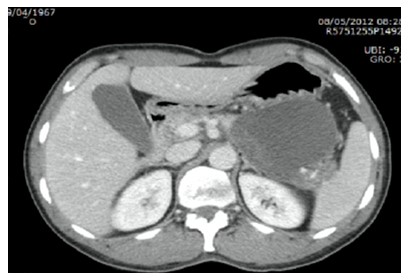
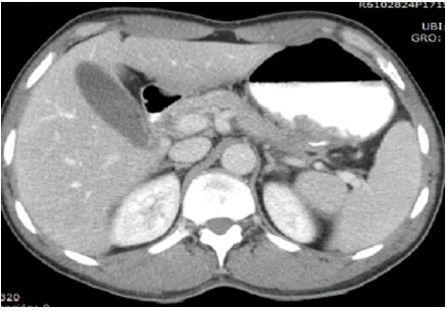
A 70-year-old male patient, with performance of EUS/ERCP with aspiration of the pseudocyst and placement of a pancreatic prosthesis one year earlier, with subsequent recurrence of the pseudocyst. A CT scan (Figure 1) demonstrated a 7.7 cm × 6.5 cm mass with its anterior wall closely contacted with the posterior wall of the stomach.
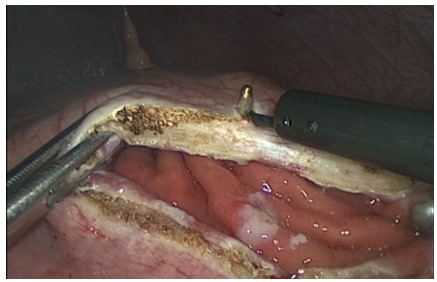
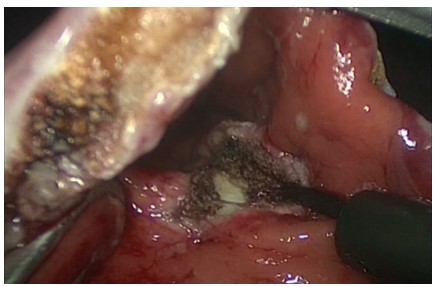
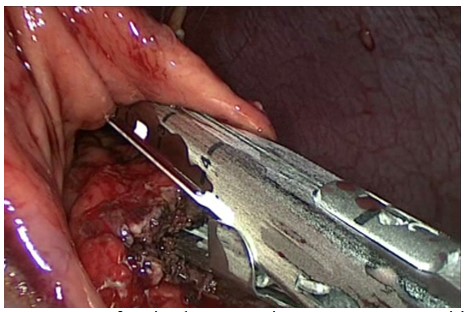
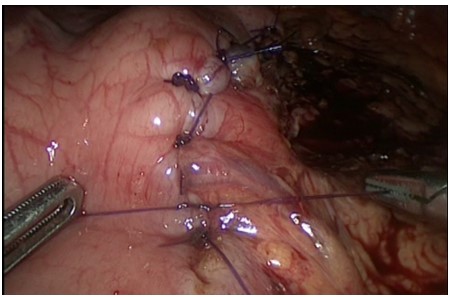
The patient underwent laparoscopic cystogastrostomy., The distribution of the trocars in the surgical field was as follows, a 10 mm port was placed subumbilically for laparoscopy, one 5-mm working ports was placed in the right subcostal area, a 12 mm port in left subcostal area and a 5-mm port was placed in the subxiphoid. Begin the laparoscopic approach performing an anterior and posterior gastrotomy using the monopolar scalpel in the area where the pseudocyst protrudes (Figures 2, 3).
There are several complications that can appear after an episode of pancreatitis; among them, the pancreatic pseudocyst is one of the most frequent. The pathophysiology, in most cases, is the result of injury or alteration of the normal anatomy of the pancreatic duct [5]. The etiology of the pseudocyst is directly related to the cause of pancreatitis; alcohol consumption is the cause in 65% of cases, followed by gallstones in 15%. Due to improvements in imaging techniques, the current prevalence is 10-20% in patients with acute pancreatitis and 20-40% in patients with chronic pancreatitis [6]. The prevalence of pancreatic pseudocyst is higher in males, between the fourth and fifth decades of life [7] and in terms of radiological studies, CT is the study of choice. Management strategies have changed and continue to evolve [8]. In the pancreatitis management guidelines written by the American College of Gastroenterology in 2013 [9], it is stated that the presence of an asymptomatic pancreatic pseudocyst can be managed conservatively regardless of size, location or extension to neighboring structures; Contrary to what was previously published, where drainage of the lesion was recommended if the size was greater than 6 cm or if it persisted beyond 6 weeks [10].
If clinically applicable, endoscopic drainage should be considered the first-line therapy for most of the pancreatic pseudocysts. Endoscopic drainage has become the first therapeutic option, it has the advantage that it is a minimally invasive procedure, it has lower cost, shorter hospital stay and offers better quality of life. This can be transpapillary with stent placement or transmural. This requires the protrusion of the pseudocyst into the lumen of the organ, the thickness of the cystic wall less than 1cm, and the absence of large vessels. To perform a transpapillary drainage, there must be communication between the pseudocyst and the pancreatic duct, for which it is extremely important to perform cholangioresonance. Among its complications we have bleeding, intestinal perforation, infection, migration of the stent and recurrence. According to published results, this procedure has an effectiveness of 90-95%, a complication rate of approximately 12%, a recurrence rate of 8% and a mortality rate of 1% [13]. Endoscopic drainage is the initial treatment of choice in most symptomatic and/or complicated pancreatic pseudocysts. Although there are no comparative controlled studies with other therapeutic alternatives, the endoscopic approach is a less invasive procedure, with a high response rate, less morbidity and recurrence comparable to other drainage techniques. After the failure of nonsurgical minimally invasive technique, the treatment chosen in our case was surgery, performing internal drainage through a communication between the pseudocyst and the stomach, all under a laparoscopic approach. The laparoscopic approach as a minimally invasive technique has been consolidated in many pathologies due to all the advantages and benefits it entails for the patient in terms of recovery, better pain control, less postoperative adhesions and a reduction in incisional hernias. Endoscopic treatment was also a good option, especially as a first option, reserving the laparoscopic approach for patients with failed endoscopic drainage. At the present time, as we have shown in our case, there are fewer and fewer arguments for performing an open surgical approach and opting for endoscopic/laparoscopic approach in these patients. Laparoscopic cystogastrostomy has been shown to be associated with shorter operating time, significantly lower postoperative morbidity and shorter hospital stay com- pared with open surgical cystogastrostomy [14].
The author declare no competing financial interest.
No.

