 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Somerville-Caso Santiago Walter1* , Ramos-Garibay José Alberto2, Haces-Caso Alfonso3, Martínez-Berlanga Paulina4
, Ramos-Garibay José Alberto2, Haces-Caso Alfonso3, Martínez-Berlanga Paulina4
1Dermatologist, Member of the Medical Association at the ABC Medical Center, Mexico City, Mexico.
2Deputy Head at the Dermatopathology Department of Pacua Dermatological Center, Mexico City, Mexico.
3Dentist, Fixed Prosthetics, Mexico City, Mexico.
4General Physician, Member of the Medical Association at the ABC Medical Center, Mexico City, Mexico.
Correspondence to: Somerville-Caso Santiago Walter, Dermatologist, Member of the Medical Association at the ABC Medical Center, Mexico City, Mexico.
Received date: June 24, 2023; Accepted date: July 04, 2023; Published date: July 11, 2023
Citation: Somerville CSW, Ramos GJA, Haces CA, et al. Ginvival Plasma Cell Granuloma: A Case Report. J Med Res Surg. 2023;4(3):60-62. doi: 10.52916/jmrs234109
Copyright: ©2023 Somerville CSW, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted
use, distribution and reproduction in any medium, provided the original author and source are credited.
Gingival Plasma Cell Granuloma (GPCG) is a rare benign lesion, which is considered within the so-called pseudotumors. In other specialties it is known as plasma cell granuloma. Histologically characterized by dense inflammatory cells infiltrates, mainly plasma cells. This manuscript presents the case of a 75 year-old woman, with a tumor in the upper alveolar region of the oral cavity. The final diagnosis corresponds to GGCP. Successfully treated with surgery, without recurrences. It is important to know this pathological entity to differentiate it form other oral cavity tumors with malignant behavior.
Gingival granuloma, Plasma cell gingivitis, Diagnosis, Inflammatory cells, Surgery.
Plasma cell granuloma of the gingiva is a tumorous lesion characterized by a proliferation of inflammatory cells [1-3]. This places GPCG in the pseudotumors group, with the consequent benign behavior. However its appearance, the characteristics of growth and the site where it is found can simulate a malignant neoplasm. It is known by synonyms such as plasma cell gingivitis [1]; inflammatory microfibrobalstic tumor, inflammatory pseudotumor [2]; benign myofibroblastoma [3]. Plasma cell infiltration can occur in any tissue.
These lesions have no sex predilection and may occur at any age, mainly in adults. The incidence of plasma cell granuloma is unclear, as well as the etiopathogenesis, biological behavior, appropriate treatments and prognosis. It may occur due to periodontitis, periradicular inflammation or may be due to an idiopathic antigenic cue. The treatment for plasma cell granuloma is a complete resection [4].
A 75 year-old female presents an asymptomatic oral cavity tumor, for the last 6 months, with progressive growth, which makes chewing moderately difficult. Without specific previous management or relevant medical history. On physical examination, a well-circumscribed exophytic lesion, with a smooth surface and firm consistency in the right upper alveolar region, was observed. Pink color with whitish areas and increased vascularity (Figure 1). Pyogenic granuloma versus gingival fibroma was the clinical diagnosis; therefore complementary studies, radiology images and incisional biopsy were requested. The radiological examination showed a slightly opaque mass that separates the dental pieces, compatible with soft tissue tumor (Figure 2). The histopathological examination of the biopsy obtained, with Hemotoxylin and Eosin stain, revealed the interpapillary processes mucosal epithelium with irregular and considerable acanthosis. Superficial lamina propria shows no alterations. The reticular lamina propria is entirely occupied by dense infiltrates, plasmatic cells predominance, organized in lobules, separated by collagen thin fibrous bundles, without atypia. The diagnosis of gingival granuloma of plasma cells is conclusive (Figure 3,4). The patient underwent a surgical procedure for the total removal of the lesion. The surgical piece reveals the same histological changes. The lesion was remove completely. Currently, 18 months later, there is no recurrence of the lesion (Figure 5).
 Figure 1: Tumor appears as a limited gingival thickening, in the right upper posterior region, separating molars. Smooth surface and an increased vascularity.
Figure 1: Tumor appears as a limited gingival thickening, in the right upper posterior region, separating molars. Smooth surface and an increased vascularity.
 Figure 2: Intraoral radiography, reveals an interdental space with radiopaque and other radiolucent areas, which suggests soft tissue tumor. Showing no bone involvement.
Figure 2: Intraoral radiography, reveals an interdental space with radiopaque and other radiolucent areas, which suggests soft tissue tumor. Showing no bone involvement.
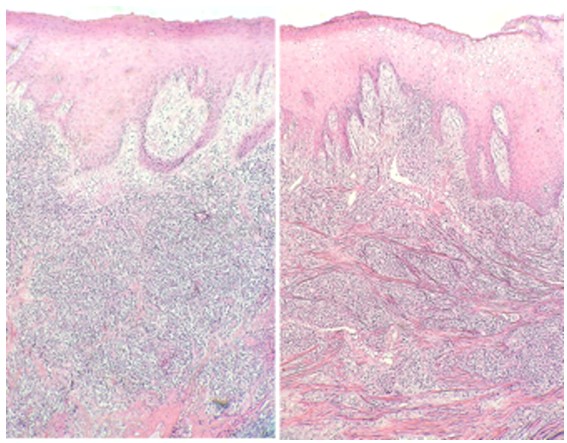 Figure 3: Histological image: epithelium with irregular acanthosis. The superficial and reticular lamina propria with dense inflammatory infiltrates. (Hemotoxylin and Eosin, 4X).
Figure 3: Histological image: epithelium with irregular acanthosis. The superficial and reticular lamina propria with dense inflammatory infiltrates. (Hemotoxylin and Eosin, 4X).
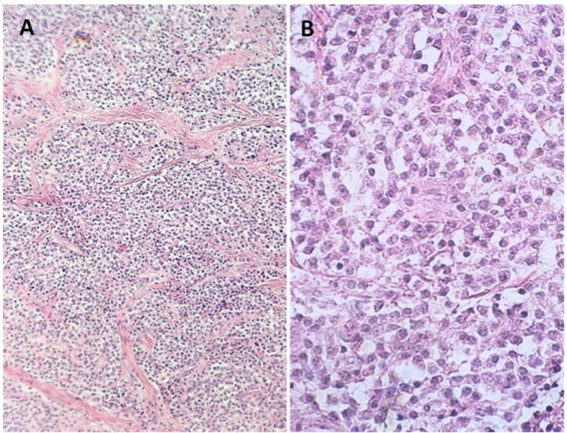 Figure 4: A): Infiltrate arrangement in foci or forming lobules (Hemotoxylin and Eosin, 10X) B): Abundant Plasma cells, with clear cytoplasm (Hemotoxylin and Eosin 40X).
Figure 4: A): Infiltrate arrangement in foci or forming lobules (Hemotoxylin and Eosin, 10X) B): Abundant Plasma cells, with clear cytoplasm (Hemotoxylin and Eosin 40X).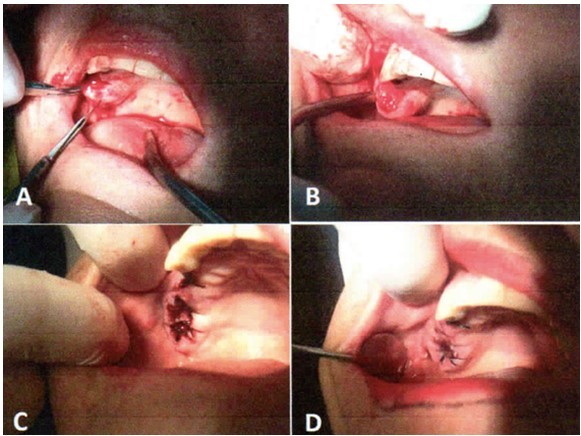 Figure 5: Surgical removal of the tumor. A, B): 3 days later; C): 8 days later; D): 14 days later.
Figure 5: Surgical removal of the tumor. A, B): 3 days later; C): 8 days later; D): 14 days later.
Zoon described the first cases published as plasmatic cell balanitis, in 1952 [5,6], an analogy is made with this type of lesions because they are benign in behavior and of unknown etiology. The vast majority of cases are described in publications related to the oral cavity and very few in dermatology journals [1,7].
Maymone and Cols 2017, published a review of benign lesions of the oral mucosa and did not consider this entity [8]. In 1973 Bahadory and Liebow reported the first cases of plasma cell granulomas present in lung, vaginal and laryngeal tissues. It can appear in other organs such as brain, heart and stomach, but the vast majorities are located in the oral cavity [6]. In 1968, Bhazkar et al, described the first cases located in the gingiva. Although the underlying cause is unknown, it is considered to be a reactive [5] and non-proliferative lesion. Kim and cols. detected the presence of IL-6 an phospholipase in the lesions. It is suggested that these substances induce the aggregation of plasma cells [2]. Other theories include the constant local trauma, the use of irritative toothpaste, the use of chewing gum, viral or bacterial infections [1,4].
The lesion ranges from reddish macule with precise limits, to a solitary exophytic tumor, sometimes hemispherical, with shades of red, smooth surfaces and sharp edges. It grows slowly and the lesion can be asymptomatic or may cause different degrees of pain [2,3,7]. The precise diagnosis is with the histopatholocgical images. The thickness of the epithelium can vary from atrophic to hyperplastic. In the thickness of the lamina propria, dense infiltrates of plasma cells, with some lymphocytes and histocytes are identified. No atypia is found. The infiltrate arrangement is in foci or forming lobules, it does no appear as a diffuse infiltrate, do not surround the blood vessels or annexes. The estroma presents different degrees of fibrosis. Immunohistochemistry reveals a polyclonal reaction with positive kappa and lambda chains [1-4,6,7].
The differential clinical diagnosis is broad, including solitary myeloma, extra medullar plasmocytoma, deep mycoses, sarcoidosis and a foreign body granulomas [5]. Histologically must be differentiated from plasma cell mucositis or gingivitis [10,11].
In the case presented, fibroma and pyogenic granuloma were ruled out. Carcinomas of various strains must also be ruled out, which is of vital importance [2,4,6,7].
The lesion´s appropriate treatment is unclear. The most commonly considered treatment for GPCG is a complete resection; however, in some cases , total surgical excision is not possible [2,4,6,7]. There are no cases reported with recurrence after surgical removal. A specialist with experience in this area, must perform the procedure. Other cases have been treated with a combination of oral prednisone 50 mg/day and azathioprine 150 mg/day [3] or with electrocoagulation with satisfactory results [1].
GPCG is an uncommon tumoral lesion, when it occurs, is generally in the gingival region. Although it’s a benign tumor, it is important to distinguish it, in order to differentiate it from a malignant neoplasm, which requires another approach. Surgical treatment is the chosen one, to avoid patient discomfort due to the effect of occupying mass.
We have no known conflict of interest to disclose.
No

