 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Guzmán-Casta Jordi1,2*, Baltazar-Contreras Rocío del Carmen2, Martínez-Vega Rocío Pamela4, Rubio-Cordero Jairo Aarón2, TéllezCampos-Lucía2, Padilla-Reyes Nelson Enrique2, Carrasco-CaraChards Sonia3, Guzmán-Huesca Jorge5, Escobar-Gómez Mario2
1Clinic of Thoracic Oncology Department, Instituto Nacional de Enfermedades Respiratorias, Dr. Ismael Cosío Villegas, Ciudad de México, México
2Clinical Oncology Department, Hospital General de México, Dr. Eduardo Liceaga, Ciudad de México, México
3Facultad de Medicina, Universidad Nacional Autónoma de México, Ciudad de México, México
4Nutritional Department, Hospital General de México, Dr. Eduardo Liceaga, Ciudad de México, México
5Internal Medicine, Bonita Community Health Center, Florida, USA
Correspondence to: Guzmán-Casta Jordi, Clinic of Thoracic Oncology Department, Instituto Nacional de Enfermedades Respiratorias, Dr. Ismael Cosío Villegas, Ciudad de México, México, México; E-mail: jordioncomed@gmail.com
Received date: September 21, 2020; Accepted date: October 2, 2020; Published date: October 10, 2020
Citation: Jordi GC, Rocío del Carmen BC, Rocío Pamela MV, et al. (2020)Extragonadal Germ Cell Tumors in the Mexican Population. J Med Res Surg 1(6): pp. 1-5.
doi:10.52916/jmrs204029
Copyright: ©2020 Jordi GC, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Aim: Extragonadal Germ Cell Tumors (EGGCT) are rare malignancies which represent a unique entity because their biology and behavior is substantially different from the tumors whose source is the gonads.
Methods: All cases of Extragonadal Germ Cell Tumors diagnosed and treated at the Department of Oncology of the General Hospital in Mexico City between 2015 and 2020 were retrospectively evaluated to determine the clinical and pathological characteristics of the tumors as well as the different treatments utilized and follow-up.
Results: Among a total of 50 patients, the mediastinum was the most frequent location, being found in 46 patients followed by 2 in the retroperitoneal space, 1 in the ethmoidal air cells, and 1 in the pineal gland. The predominant histopathology was a mixed germinal tumor in 82% of the cases with the rest being pure seminomas. All patients received first-line systemic treatment followed by surgery or second-line treatment according to their initial response to therapy. Conclusions: Extragonadal Germ Cell Tumors require a multidisciplinary approach to achieve an adequate diagnosis and treatment. The clinical and pathological differences like tumor site, histopathological type, and tumor stage influence the progression-free survival and the global overall survival.
Extragonadal tumors, Germ cell, Global overall survival, Progression-free survival
Extragonadal Germ Cell Tumors (EGGCT) are rare malignancies arising from anatomical locations different from the gonads. They represent a unique entity because their biology and behavior is substantially different from the tumors whose source is the gonads [1-2].
Approximately between 3% to 5% of all Germ Cell Tumors arise from non-gonadal sources, particularly from the mediastinum (Figure 1), the retroperitoneal space (Figure 2), the pineal gland (Figure 3), ethmoidal air cells (Figure 4), affecting mainly young adults in the third decade of life [1]
The cytogenetic, histologic and serologic characteristics of the Extragonadal Germ Cell Tumors are similar to those of the gonadal tumors but important differences exist suggesting that these tumors may be biologically different and as such the Extragonadal Germ Cell Tumors are considered a unique and independent entity requiring a different multimodal approach. Combined management based on multiple agent chemotherapy, surgery and radiotherapy is a pivotal part of the treatment [3-4].
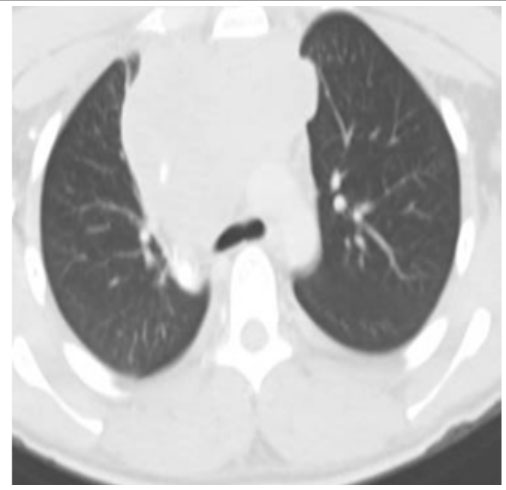 Figure 1: Non-seminoma mediastinal mixed germ cell tumor.
Figure 1: Non-seminoma mediastinal mixed germ cell tumor. Figure 2: Mixed retroperitoneal germ cell tumor.
Figure 2: Mixed retroperitoneal germ cell tumor.
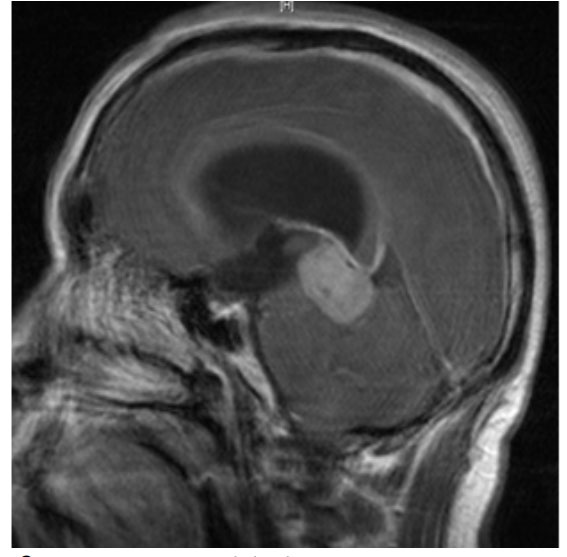 Figure 3: Pure seminoma pineal gland.
Figure 3: Pure seminoma pineal gland.
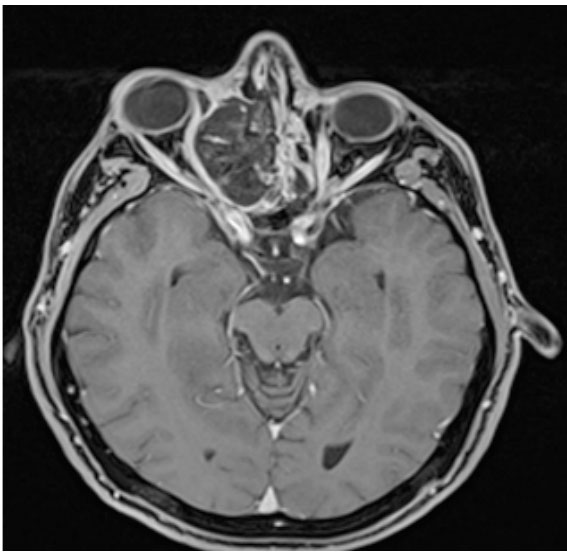 Figure 4: : Pure primary seminoma of the ethmoidal air cells..
Figure 4: : Pure primary seminoma of the ethmoidal air cells..
The clinical manifestations are mainly related to the localization of the tumor, patients with mediastinal masses complain of dyspnea (25%), precordial pain (23%), and cough (17%) as the initial presentation followed by fever (13%), loss of weight (11%), superior vena cava syndrome and tiredness and fatigue (6%). Less common symptoms reported were hoarseness, hemoptysis, and dysphagia (1%). Patients with retroperitoneal tumors experienced abdominal pain (29%), back pain (14%), other symptoms are loss of weight (9%), fever (8%), inferior vena cava thrombosis (9%), palpable abdominal mass (6%), cervical lymph node enlargement (4%), scrotal edema (5%), gynecomastia and dysphagia (3%) [5-8].
Metastasis is less frequent with Seminomatous Extragonadal Germ Cell Tumors (40%) compared to Non-Seminomatous (50% and 76% mediastinal and retroperitoneal tumors respectively). The pattern of metastasis varies according to the tumor location and its histology; mediastinal seminomas have mainly metastatic deposits in the cervical lymph nodes while non-seminomatous tumors have lung metastasis in 27% of the cases. The retroperitoneal seminoma produces metastasis to retroperitoneal lymph nodes (26%), mediastinal lymph nodes (12%), and cervical lymph nodes (6%) while the nonseminomatous retroperitoneal tumor causes lung metastasis (49%), the involvement of the abdominal and cervical lymph nodes (34% and 18% respectively), and hepatic metastasis (25%) [8-10]
Because Extragonadal Germ Cell Tumors are not as clinically evident as the Primary Gonadal Tumors the diagnosis is most of the time suspected when symptoms are related to the growth of the tumor in the mediastinum or the retroperitoneal cavity appear. A percutaneous fine needle biopsy or a diagnostic mediastinoscopy can reveal seminomatous or non-seminomatous elements but sometimes the term “undifferentiated carcinoma” is reported by pathology, in that case, it’s very important to obtain serum tumor markers and to request germ specific immunopathology that should result in a more precise diagnosis in almost all the cases [11-14].
Seminomatous Extragonadal Germ Cell Tumors of the mediastinum and retroperitoneal space carry the same prognosis as their counterpart gonadal tumors, with a 5 years survival of 88%. The prognostic markers used in the gonadal tumors like HGC and LDH levels, the presence of non-pulmonary visceral metastasis, or primary tumor in the mediastinum are equally effective to predict good or intermediate prognosis in primary tumors of the extragonadal source.
Non-seminomatous Germ Cell Tumors have a worse prognosis than the Seminomatous tumors with a 5 years survival rate of 62% for the retroperitoneal and 45% for the mediastinal location. The rate of Complete Response with normalization of the tumor markers is 68% and 64% respectively for retroperitoneal and mediastinal tumors and the relapse rate is 50 % for the retroperitoneal tumors and 52% for the mediastinal location [15].
The principles of therapy for Seminomatous and NonSeminomatous Extragonadal Tumors run parallel to those described in the NCCN (National Comprehensive Cancer Network) guidelines for Gonadal Germ Cell Tumors. The emergent role of chemotherapy in patients with advanced seminomas has led many researchers to use Cisplatin-based therapy as primary treatment. Based on this, patients with good prognosis should be treated with 3 cycles of Cisplatin, Etoposide, and Bleomycin (BEP) and those with intermediate prognosis should receive 4 cycles [16]. Patients with large volume seminomas regardless of its location frequently have residual radiographic abnormalities following chemotherapy. The ideal management for patients with residual tumor after chemotherapy remains controversial.
Patients with seminoma and a residual tumor after chemotherapy of more than 3 cm carry the risk to harbor a viable tumor. In these patients, surgical resection is recommended to determine the nature of the mass and the need for further therapy.
In the case of Non-Seminomatous mediastinal tumors, the consensus is for chemotherapy as the primary line of treatment and because they carry a worse prognosis, a 4 cycles therapy with Cisplatin, Etoposide, and Bleomycin (BEP) is recommended. If posterior to therapy the serum levels of tumoral markers return to normal, a complete resection of the persistent radiographic abnormalities by an experienced thoracic surgeon is crucial to eliminate any residual tumor. However, and given the rarity of this subgroup of tumors, there is a lack of consensus for treatment strategies. In this study, we retrospectively reviewed our experience with Extragonadal Germ Cell Tumors emphasizing the clinical and pathological characteristics as well as the multimodal therapeutic approach.
We conducted a retrospective and descriptive analysis in patients diagnosed with Mixed Extragonadal Germ Cell Tumors between January of 2014 and December of 2019 at General Hospital in Mexico City. During this period a total of 50 patients were recruited and each one of them was diagnosed through histopathology obtained by biopsy of the tumoral mass. Patients with Primary Gonadal Germ Cell Tumors were excluded from the study. All clinical and pathological details, age, sex, primary location, serum tumoral marker levels, radiographic and surgical reports were obtained through the Hospital Patient Registry. The most frequent primary location was the mediastinum in 46 cases followed by the retroperitoneal cavity in 2 and the ethmoidal air cells and the pineal gland with 1 case respectively.
After analyzing the clinical data and pathology reports, we observed that the predominant histology was the Mixed Germ Cell Tumor in 82% of the cases with the rest of the cases being Pure Seminomas. All patients received first-line systemic therapy with Bleomycin, Etoposide and Cisplatin (BEP) with posterior clinical, biochemical, and radiological evaluation. Seven patients were referred for surgical treatment due to persisting residual tumor after chemotherapy and 15 patients underwent a second line of therapy with Paclitaxel, Ifosfamide, MESNA, and Cisplatin (TIP) due to persistence or progression of the disease. 10 of these patients initiated active surveillance as their disease reached a stable status but the other 5 with evidence of progression were treated with GemcitabiThe total of patients with progression of the disease represent 28% of the total mortality.ne and Oxaliplatin (GemOx) as a third-line therapy.
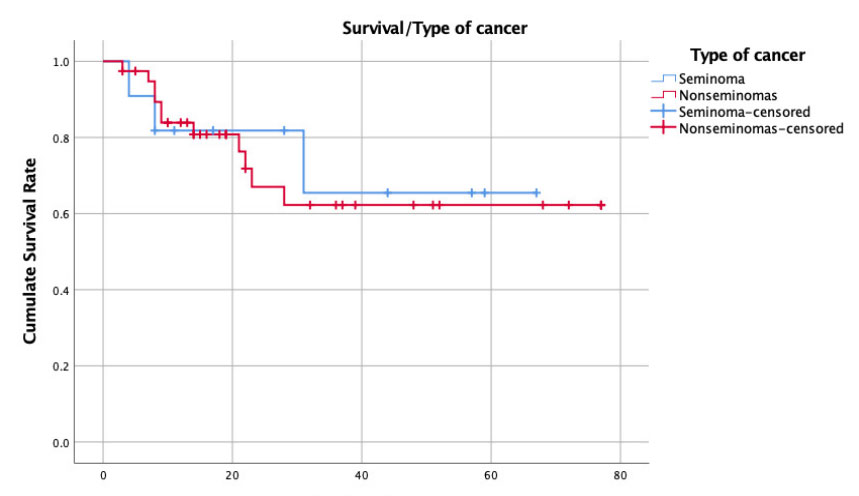 Figure 5: Table of response to treatment
Figure 5: Table of response to treatmentEleven patients of the total of 39 with Non-Seminomatous Tumors died compared to 3 out of 11 in the Seminoma Tumor group
For mortality, these were the results: 1 out of 7 patients treated with BEP+TIP died as well as 3 out of 5 patients treated with BEP+TIP +GemOx. 3 out of 6 patients treated with BEP+RT also died and the 2 patients treated with BEP+TIP+RT succumbed to the disease. Of the total of 27 patients who received BEP as therapy 4 of them died. We observed an overall mortality rate of 28%. Acknowledging that Extragonadal Germ Cell Tumors are rare, to be able to observe 50 patients in a Tertiary Care Hospital is important to gather experience about the disease and although we know the biology of the gonadal and extragonadal tumors and that the latter particularly have a midline presentation, it was interesting to see that up to 82% of the cases in our series were Non-Seminomatous Mixed Germ Cell tumors. These tumors usually require a more intense multimodal management and our patients observed a lower overall survival rate compared to the pure seminomas that accounted for only 18% of the total tumors. Being Bleomycin, Etoposide and Cisplatin (BEP) the mainstay of therapy for Germ Cell Tumors, those who had at least a partial response to it plus consolidation with Radiotherapy had better survival than those who required second-line therapy with TIP, VIP, or GemOx and with that we conclude that the best outlook for a patient with an extragonadal tumor is for this tumor to be a pure seminoma that responds completely or at least partially to first-line chemotherapy and radiation consolidation to increase the free of disease progression and overall survival.
Figure 6: Partial data diagram.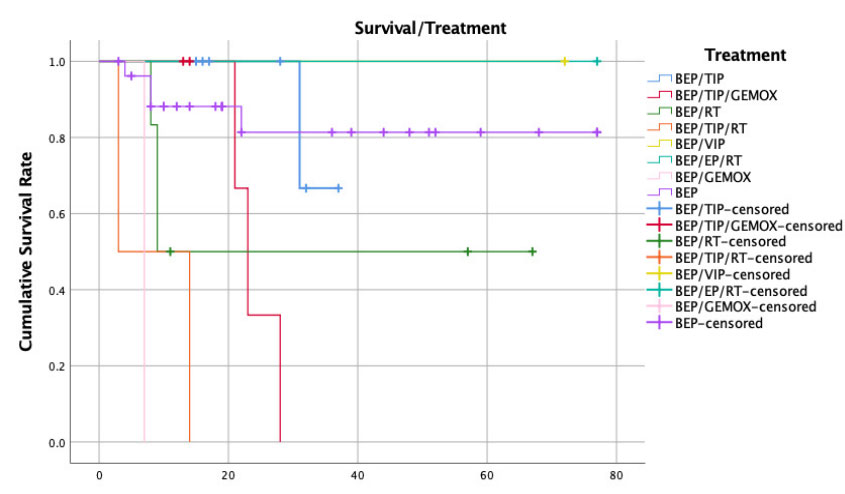 Figure 7: Chemotherapy treatment different modalities
Figure 7: Chemotherapy treatment different modalities
