 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Ahmet Dumanli1* , Suphi Aydin1, Gülcan Gencer2
, Suphi Aydin1, Gülcan Gencer2
1Department of Chest Surgery, Afyonkarahisar Health Sciences University Faculty of Medicine, 03200, Afyonkarahisar, Turkey
2Department of Biostatistics and Medical Informatics, Afyonkarahisar Health Sciences University Faculty of Medicine, 03200, Afyonkarahisar, Turkey
Correspondence to: Ahmet Dumanli, Department of Chest Surgery, Afyonkarahisar Health Sciences University Faculty of Medicine, 03200, Afyonkarahisar, Turkey
Received date: September 09, 2022;; Accepted date: September 21, 2022; Published date: September 29, 2022
Citation: Dumanli A, Aydin S, Gencer G. Evaluation of Traumatic Vertebra and Rib Fractures. J Med Res Surg. 2022; 3(5): 86-95. doi: 10.52916/jmrs224086
Copyright: ©2022 Dumanli A, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted
use, distribution and reproduction in any medium, provided the original author and source are credited.
Background: In our study, we aimed to examine the relationship between trauma-related thoracic
vertebral fractures and/or rib fractures location, age and gender.
Methods: Between January 1, 2020 and December 31, 2020, 100 patients with trauma-related thoracic
vertebral fracture and/or rib fracture were included in the study. Rib fractures and thoracic vertebral
fractures were analyzed according to age, gender, level and fracture type. The correlation between rib
and vertebral fractures was investigated.
Results: 72% of the patients were male and 28% were female, mean age was 48.49 ± 18.83. Thoracic
vertebral corpus fractures were detected most frequently in T8 in 22 patients and in T1 in at least 1
patient. Spinous process fracture was found to be highest in T2 with 9 patients, and 1 patient each in T5,
T6, and T12. Transverse processes fracture was seen in T9 with a maximum of 5 patients. Rib fractures
were observed more frequently on the right. Displaced rib fractures were most common in the 6th and 7th
ribs, and non-displaced rib fractures were observed in the 5th ribs with 9 patients. Left rib fractures were
most common in the 5th rib, with 6 displaced patients and 8 non-displaced patients. When the thoracic
vertebral fractures and rib fractures were examined depending on the age variable, it was determined
that the fractures in the T2 spinous, T3 spinous, T5 corpus and T8 vertebral corpus, and rib fractures in
the right 4,6,8,10 and left 2 and 4 differ depending on the age variable (p<0.05). When thoracic vertebral
fractures and rib fractures were analyzed depending on gender, a correlation was found between T7
vertebral body fractures and left 6th rib fractures (p<0.05).
Conclusion: The coexistence of vertebral and rib fractures should be kept in mind in trauma patients,
and plans for diagnosis and treatment should be made accordingly.
Thorax, Rib, Vertebra, Fracture, Trauma
Trauma is a condition that occurs as a result of external factors and disrupts the structure of the body [1]. It is the most common cause of death after cancer and heart diseases among all age groups [2,3].
The first known definition of thoracic trauma was made in 1600 BC [3]. Thoracic trauma is the third most common trauma among all trauma cases, present in 40% of trauma cases [4] and [5,6]. Thoracic traumas constitute one third of emergencies and hospitalizations due to trauma among all trauma cases [5,7]. It is responsible for approximately 20-25% of all trauma-related deaths [2,4,7]. Although traffic accidents are the most common cause of blunt thoracic trauma, it can also be seen due to situations such as beating, falling, and crushing [8].
The most common finding in thoracic traumas is rib fractures and the most common 4-9. It is seen in the ribs [5,7,9-11]. Fractures of the ribs are very common in clinical practice and although most of them have limited clinical significance [12], respiratory functions can sometimes be adversely affected [13]. More than half of rib fractures caused by blunt trauma are uncomplicated and only healed with analgesic therapy [14]. In rib fractures that cause complications, treatment is performed for the cause. While the overall mortality is reported as 9% in thoracic traumas, this rate increases to 13-15% if there is a co-system injury, and up to 30-35% if there is more system injury [11]. The most common finding in thoracic traumas is rib fractures and is most commonly seen in the 4th-9th ribs [5,7,9- 11]. Fractures of the ribs are very common in clinical practice and although most of them have limited clinical significance [12], respiratory functions can sometimes be adversely affected [13]. More than half of rib fractures caused by blunt trauma are uncomplicated and only healed with analgesic therapy [14]. In rib fractures that cause complications, treatment is performed for the cause. While the overall mortality is reported as 9% in thoracic traumas, this rate increases to 13-15% if there is a cosystem injury, and up to 30-35% if there is more system injury [11].
Along with rib fractures, vertebral fractures are usually seen as a result of high-energy blunt trauma [15]. Thoracic traumas are accompanied by vertebral fractures at a rate of 6%. The most affected area in vertebral column traumas is the thoracic vertebra. The most important reason is that the longest part of the vertebral column consists of thoracic vertebra [11]. Neurological damage and morbidity are higher in fractures of this region compared to vertebral fractures in other regions [15]. Its causes are narrow spinal canal in the thoracic region, less distance between the spinal cord and bone parts, and more limited blood flow to the spinal cord in this region [16]. Conservative treatment is preferred in cases where there is no neurological deficit and the spine is stable in vertebral fractures in the thoracic region [17]. However, there are indications for surgical treatment in fractures with severe loss of vertebral body height with canal compression, neurological deficit and kyphotic deformity [17,18]. The main purpose of surgical treatment is to protect or improve the neurological status, to provide stability, to correct the deformity, and to prepare the ground for early rehabilitation [17,19].
Approval was obtained from Afyonkarahisar Health Sciences University Clinical Research Ethics Committee with the date and number of 2022/3. The files of 250 patients who had trauma between January 1, 2020 and December 31, 2020 were reviewed retrospectively. Conditions that increase co-morbidity such as osteoporosis and malignancy were excluded from the study.
The patients with vertebral fractures and/or rib fractures were identified by examining the thoracic computed tomography scans of the patients. 100 patients with traumatic rib fracture and/or thoracic vertebral fracture were included in the study. The level of rib fractures, displaced or non-displaced conditions were detected in the thoracic computed tomography. The levels and types of fractures (corpus fracture, transverse and spinous process fractures) in patients with thoracic vertebral fractures were determined. The relationship between vertebral fractures and rib fractures was examined.
Chi-square analysis was used to determine whether the cases of complete fractures or cracks in the patients changed depending on the age and gender variable. Statistical analyzes were made using the "IBM SPSS Statistics 26" program. Descriptive statistics for all variables and chi-square analysis were used for evaluation. All results were considered statistically significant with p<0.05 values.
100 patients with rib fracture and/or thoracic vertebra fracture were included in this study. Of the patients, 72% were male and 28% were female. The mean age in men was 45.5 ± 17.92 years, in women the mean age was 56.18 ± 19.26, and the mean overall age was 48.49 ± 18.83 (Table 1).
| Variables | Frequency |
Mean |
Standard Deviation |
|
| Sex | Male |
72 |
45.5 |
17.92 |
Female |
28 |
56.18 |
19.26 |
|
| Age | 30 and below |
27 |
- |
- |
31-44 |
13 |
- |
18.83 |
|
45-56 |
19 |
48.49 |
- |
|
57-70 |
25 |
- |
- |
|
71 and above |
16 |
- |
- |
|
| Total | 100 |
- |
- |
|
When the fracture levels, corpus fracture, transverse and spinous fractures in patients with thoracic vertebral fractures were examined; the fracture rate in corpus was found to be high between T3 and T9. It was observed that the most corpus fractures were in T8 with 22 patients. Corpus fracture was detected in T1 with at least 1 patient. The fracture rate is generally low in spinous process. The highest fracture rate was in the T2 spinous process with 9 patients. Spinous fracture is the least common place in T5, T6 and T12 with 1 patient each. Transverse processes fracture was seen in T9 with a maximum of 5 patients. T1 and T2 transverse process fractures were not detected (Table 2).
Trauma |
Frequency |
Percent |
|
| T1 corpus | None |
99 |
99 |
Displaced |
1 |
1 |
|
| T1 spinous process | None |
97 |
97 |
Displaced |
3 |
3 |
|
| T1 tranverse process | None |
100 |
100 |
| T2 corpus | None |
98 |
98 |
Displaced |
2 |
2 |
|
| T2 spinous process | None |
91 |
91 |
Displaced |
9 |
9 |
|
| T2 tranverse process | None |
100 |
100 |
| T3 corpus | None |
90 |
90 |
Displaced |
10 |
10 |
|
| T3 spinous process | None |
93 |
93 |
Displaced |
7 |
7 |
|
| T3 tranverse process | None |
99 |
99 |
Displaced |
1 |
1 |
|
| T4 corpus | None |
79 |
79 |
Displaced |
21 |
21 |
|
| T4 spinous process | None |
98 |
98 |
Displaced |
2 |
2 |
|
| T4 tranverse process | None |
98 |
98 |
Displaced |
2 |
2 |
|
| T5 corpus | None |
84 |
84 |
Displaced |
16 |
16 |
|
| T5 spinous process | None |
99 |
99 |
Displaced |
1 |
1 |
|
| T5 tranverse process | None |
98 |
98 |
Displaced |
2 |
2 |
|
| T6 corpus | None |
88 |
88 |
Displaced |
12 |
12 |
|
| T6 spinous process | None |
99 |
99 |
Displaced |
1 |
1 |
|
| T6 tranverse process | None |
96 |
96 |
Displaced |
4 |
4 |
|
| T7 corpus | None |
83 |
83 |
Displaced |
17 |
17 |
|
| T7 spinous process | None |
98 |
98 |
Displaced |
2 |
2 |
|
| T7 tranverse process | None |
98 |
98 |
Displaced |
2 |
2 |
|
| T8 corpus | None |
78 |
78 |
Displaced |
22 |
22 |
|
| T8 spinous process | None |
98 |
98 |
Displaced |
2 |
2 |
|
| T8 tranverse process | None |
96 |
96 |
Displaced |
4 |
4 |
|
| T9 corpus | None |
84 |
84 |
Displaced |
16 |
16 |
|
| T9 spinous process | None |
97 |
97 |
Displaced |
3 |
3 |
|
| T9 tranverse process | None |
95 |
95 |
Displaced |
5 |
5 |
|
| T10 corpus | None |
90 |
90 |
Displaced |
10 |
10 |
|
| T10 spinous process | None |
95 |
95 |
Displaced |
5 |
5 |
|
| T10 tranverse process | None |
96 |
96 |
Displaced |
4 |
4 |
|
| T11 corpus | None |
87 |
87 |
Displaced |
13 |
13 |
|
| T11 spinous process | None |
97 |
97 |
Displaced |
3 |
3 |
|
| T11 tranverse process | None |
96 |
96 |
Displaced |
4 |
4 |
|
| T12 corpus | None |
81 |
81 |
Displaced |
19 |
19 |
|
| T12 spinous process | None |
99 |
99 |
Displaced |
1 |
1 |
|
| T12 tranverse process | None |
97 |
97 |
Displaced |
3 |
3 |
|
Total |
100 |
100 |
When the fracture levels in patients with right rib fracture were examined; it was observed that the rate of displaced fracture was higher in the right 6th and 7th ribs with 8 patients each. Non-displaced fractures were found to be higher between the 4-11 ribs on the right. 9 patients had the highest rate of non-displaced fracture in the right 5th rib, While non-displaced and displaced fractures were observed in at least the 1st rib in 6 patients, no fractures were found in the 12th ribs (Table 3) (Figure 1).
| Ribs | Trauma |
Frequency |
Percent |
| Right 1 | None |
94 |
94 |
Non-Displaced |
2 |
2 |
|
Displaced |
4 |
4 |
|
| Right 2 | None |
97 |
97 |
Non-Displaced |
1 |
1 |
|
Displaced |
2 |
2 |
|
| Right 3 | None |
96 |
96 |
Non-Displaced |
1 |
1 |
|
Displaced |
3 |
3 |
|
| Right 4 | None |
93 |
93 |
Non-Displaced |
4 |
4 |
|
Displaced |
3 |
3 |
|
| Right 5 | None |
84 |
84 |
Non-Displaced |
9 |
9 |
|
Displaced |
7 |
7 |
|
| Right 6 | None |
86 |
86 |
Non-Displaced |
6 |
6 |
|
Displaced |
8 |
8 |
|
| Right 7 | None |
86 |
86 |
Non-Displaced |
6 |
6 |
|
Displaced |
8 |
8 |
|
| Right 8 | None |
91 |
91 |
Non-Displaced |
3 |
3 |
|
Displaced |
6 |
6 |
|
| Right 9 | None |
92 |
92 |
Non-Displaced |
6 |
6 |
|
Displaced |
2 |
2 |
|
| Right 10 | None |
92 |
92 |
Non-Displaced |
6 |
6 |
|
Displaced |
2 |
2 |
|
| Right 11 | None |
93 |
93 |
Non-Displaced |
5 |
5 |
|
Displaced |
2 |
2 |
|
| Right 12 | None |
98 |
98 |
Displaced |
2 |
2 |
|
| Left 1 | None |
95 |
95 |
Non-Displaced |
4 |
4 |
|
Displaced |
1 |
1 |
|
| Left 2 | None |
92 |
92 |
Non-Displaced |
7 |
7 |
|
Displaced |
1 |
1 |
|
| Left 3 | None |
94 |
94 |
Non-Displaced |
5 |
5 |
|
Displaced |
5 |
5 |
|
| Left 4 | None |
92 |
92 |
Non-Displaced |
5 |
5 |
|
Displaced |
3 |
3 |
|
| Left 5 | None |
86 |
86 |
Non-Displaced |
8 |
8 |
|
Displaced |
6 |
6 |
|
| Left 6 | None |
91 |
91 |
Non-Displaced |
7 |
7 |
|
Displaced |
2 |
2 |
|
| Left 7 | None |
92 |
92 |
Non-Displaced |
6 |
6 |
|
Displaced |
2 |
2 |
|
| Left 8 | None |
91 |
91 |
Non-Displaced |
5 |
5 |
|
Displaced |
4 |
4 |
|
| Left 9 | None |
92 |
92 |
Non-Displaced |
6 |
6 |
|
Displaced |
2 |
2 |
|
| Left 10 | None |
96 |
96 |
Non-Displaced |
3 |
3 |
|
Displaced |
1 |
1 |
|
| Left 11 | None |
97 |
97 |
Non-Displaced |
3 |
3 |
|
| Left 12 | None |
100 |
100 |
Total |
100 |
100 |
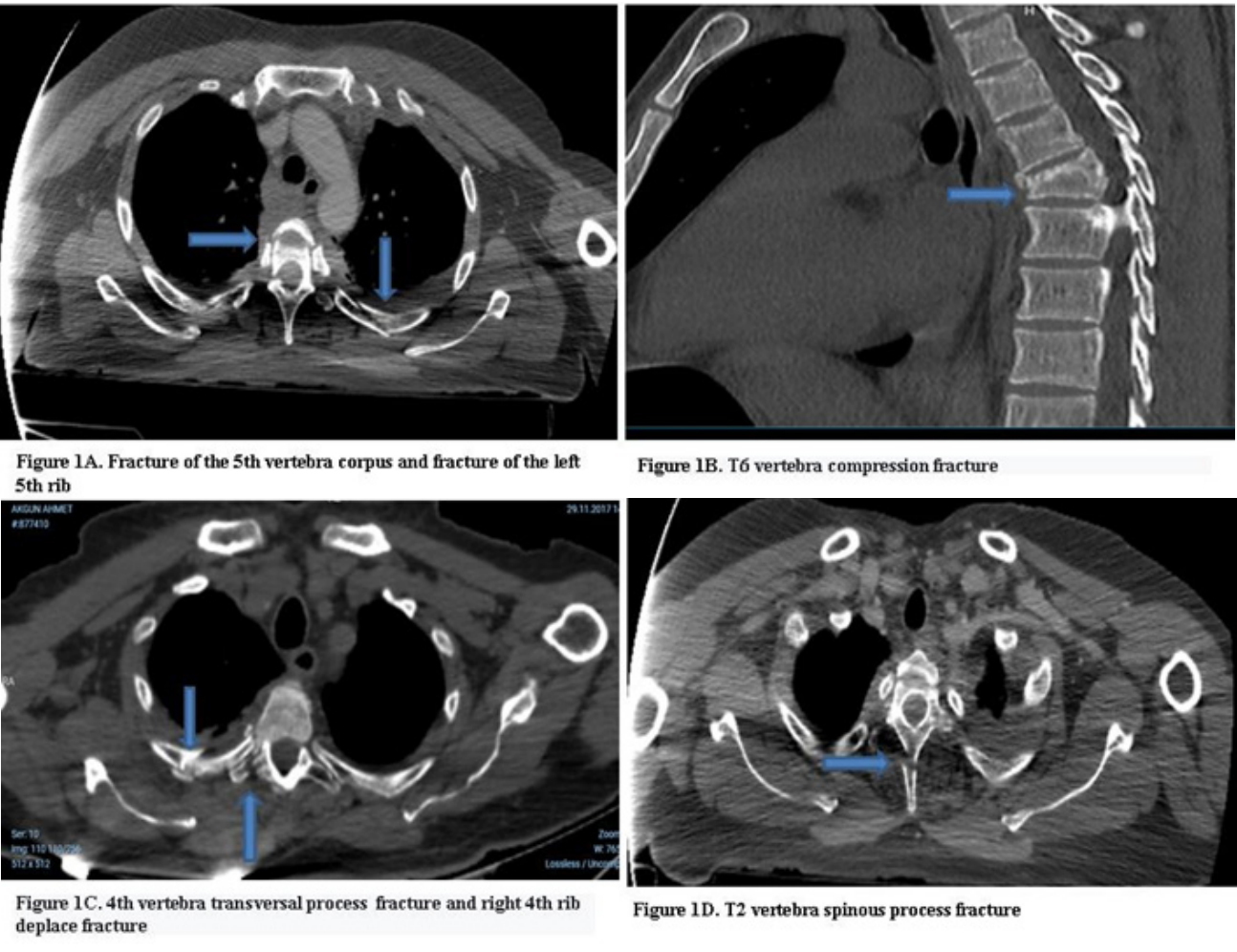 Figure 1: Computed tomography images of vertebra and rib fractures.
Figure 1: Computed tomography images of vertebra and rib fractures.When the fracture levels in patients with left rib fracture were examined; it was observed that the rate of displacement fracture was highest in the left 5th rib with 6 patients. It was determined that the rate of non-displaced fractures between the left 3 and 9 was high. The most common rib fractures were observed in the 5th rib with 6 displaced patients and 8 nondisplaced patients, while the least were detected in the 10th rib in 4 patients. While no displaced or non-displaced fracture was observed in the 12th rib, no displaced fracture was observed in the 11th rib (Table 3) (Figure 1).
When examining whether the fracture levels, corpus fracture, transverse and spinous fracture status of patients with thoracic vertebral fractures change depending on the age variable; A correlation was found between the fractures in T2 spinous, T3 spinous, T5 corpus and T8 vertebral corpus and the age variable (p<0.05). No significant correlation was found between the fracture levels and the age variable in patients with other thoracic vertebral fractures (p>0.05) (Table 4).
T2 spinous process |
Total | Chi-Square Tests | |||
None |
Displaced |
0.038* | |||
| Age | 30 and below |
26 |
1 |
27 |
|
31-44 |
13 |
0 |
13 |
||
45-56 |
14 |
5 |
19 |
||
57-70 |
24 |
1 |
25 |
||
71 and above |
14 |
2 |
16 |
||
| Total | 91 |
9 |
100 |
||
T5 corpus |
Total |
Chi-Square Tests | |||
None |
Displaced |
||||
| Age | 30 and below |
20 |
7 |
27 |
0.039* |
31-44 |
11 |
1 |
12 |
||
45-56 |
13 |
6 |
19 |
||
57-70 |
23 |
2 |
25 |
||
71 and above |
16 |
0 |
16 |
||
| Total | 83 |
16 |
99 |
||
T8 corpus |
Total | Chi-Square Tests | |||
None |
Displaced |
||||
| Age | 30 and below |
24 |
3 |
27 | 0.011* |
31-44 |
7 |
6 |
13 | ||
45-56 |
11 |
8 |
19 | ||
57-70 |
22 |
3 |
25 | ||
71 and above |
14 |
2 |
16 | ||
| Total | 78 |
22 |
100 | ||
When examining whether the cases of fractures or cracks in the right and left ribs change depending on the age variable; It was understood that the fractures in the right 4,6,8 and 10 and left 2 and 4 differed depending on the age variable (p<0.05). No significant relationship was found between the other ribs and the age variable (p>0.05) (Table 5).
Right 8 |
Total | Chi-Square Tests (p value) | ||||
| None | Non-Displaced | Displaced | ||||
| Age | 30 and below | 26 |
1 |
0 |
27 |
0.021* |
| 31-44 | 10 |
0 |
3 |
13 |
||
| 45-56 | 18 |
1 |
0 |
19 |
||
| 57-70 | 25 |
0 |
0 |
25 |
||
| 71 and above | 12 |
1 |
0 |
16 |
||
| Total | 91 |
3 |
6 |
100 |
||
Right 10 |
Total |
Chi-Square Tests (p value) | ||||
None |
Non-Displaced |
Displaced |
||||
| Age | 30 and below | 27 |
0 |
0 |
27 |
0.021* |
| 31-44 | 11 |
0 |
2 |
13 |
||
| 45-56 | 17 |
2 |
0 |
19 |
||
| 57-70 | 23 |
2 |
0 |
25 |
||
| 71 and above | 14 |
2 |
0 |
16 |
||
| Total | 92 |
6 |
2 |
100 |
||
Left 2 |
Total |
Chi-Square Tests (p value) |
||||
None |
Non-Displaced |
Displaced |
||||
| Age | 30 and below |
27 |
0 |
0 |
27 |
0.015* |
31-44 |
13 |
0 |
0 |
13 |
||
45-56 |
13 |
5 |
1 |
19 |
||
57-70 |
24 |
1 |
0 |
25 |
||
71 and above |
15 |
1 |
0 |
16 |
||
| Total | 92 |
7 |
1 |
100 |
||
Left 4 |
Total
|
Chi-Square Tests (p value) |
||||
None |
Non-Displaced |
Displaced |
||||
| Age | 30 and below |
27 |
0 |
0 |
27 |
0.008* |
31-44 |
13 |
0 |
0 |
13 |
||
45-56 |
13 |
4 |
2 |
19 |
||
57-70 |
25 |
0 |
0 |
25 |
||
71 and above |
14 |
1 |
1 |
16 |
||
| Total | 92 |
5 |
3 |
100 |
||
When the relationship between vertebral fracture and gender variable is examined; T7 only a significant relationship was found between the corpus vertebral and the gender variable (p<0.05). In this table 6, only 1 fracture in the T7 corpus was observed in women, while 16 fractures were detected in men. No significant relationship was found between other thoracic vertebral and gender variables (p>0.05) (Table 6).
| Left 6th Rib | None |
Non-Displaced |
Displaced |
Total |
Chi-Square Tests |
|
| Sex | Male | 68 |
2 |
2 |
72 |
0.022 |
| Female | 23 |
5 |
0 |
28 |
||
| Total | 91 |
7 |
2 |
100 |
||
| T7 vertebral corpus | None |
Displaced |
Chi-Square Tests |
|||
| Sex | Male | 56 |
16 |
72 |
72 |
0.019 |
| Female | 27 |
1 |
28 |
|||
83 |
17 |
100 |
||||
When the relationship between rib fracture and gender variable is examined; only a significant relationship was found between the left 6th rib and the gender variable (p<0.05). In this table, only cracks were observed in the left 6th rib in women, while both cracks and fractures were detected in men. No significant relationship was found between the other right and left ribs and the gender variable (p>0.05) (Table 6).
Cobanoglu, et al. in their study, they found that chest traumas were more common in males and between the 2nd and 5th decades [20]. Wang XR, et al. of 263 patients with vertebral fractures found that the mean age was 42.11 ± 9.82 years and it was more common in males [21]. Varlik M, et al. they found that 69.7% of the patients who had thoracic trauma were male and the mean age was 38 years [22]. Saricam M, et al. in their study of 195 patients, they found that 20% of the patients were women and 80% were men. They found the age range to be 3-93/year with an average of 40.2 years. They reported that the most common thoracic pathology was rib fractures [2].
Rakip U, et al. in their study of 148 men and 104 women, a total of 252 patients, they reported that thorax traumas were more common in men [17].
In our study, 72% of the patients were male and 28% were female, mean age in men was 45.5 ± 17.92, mean age in women was 56.18 ± 19.26, mean overall age was 48.49 ± 18.83.
In the study of İmamoğlu, et al. the incidence of rib fractures due to trauma was found to be 36.4% [23]. However, in different studies, the incidence of rib fractures due to general body trauma was reported to be between 7-40%, and rib fractures due to isolated thoracic trauma were reported to be between 6-12% [24].
In our study, different levels of vertebral fracture and/or rib fracture were detected in 100 (40%) of 250 patients who had general body trauma.
Wang XR, et al. found the frequency order of trauma-related vertebral fractures to be L1, followed by T12 and L2 fractures [21]. In another study, Göya C, et al. stated that 6% of the thoracic traumas were accompanied by vertebral fractures, and they found that the most common fracture site was the thoracic vertebra [12]. Büyükkarabacak YB, et al. determined that 6% of thoracic traumas were accompanied by vertebral fractures. They found the most common thoracic fracture [11]. Ayaz UY, et al. found that 86.7% of the patients with vertebral fractures were in the lumbar vertebra and 13.3% were in the thoracic vertebra [25]. Varlik M, et al. In their study on 1338 patients who had thoracic trauma, they found rib fracture in 29 (2.2%) and vertebral fracture in 56 (4.2%) [22]. Wang XR, et al. L1 fracture in his study; found 25.3% in men and 36.5% in women. They found T12 fracture in 17.7% in men and 19.2% in women. L2 fracture; found 14.6% for men and 10.6% for women [21]. Ulrich J, et al. evaluated 35 articles on vertebral differences, and found that the most common fracture sites were T11/T12 thoracic vertebra and L1/L2 lumbar vertebra [26]. Dumanli A, et al. in their study on 201 cases, they found that rib fractures were more common on the right side, displaced fractures were seen more frequently, and most frequently between the ribs of 48.3% and 5-8%, nondisplaced fractures were the least and most common in 20.4% [9-12] reported that it was between the ribs [5].
In our study, vertebral fractures were most common at the T8 level in 22 patients in the corpus region. It was at least at T1 level and was present in 1 patient. Transverse process fracture was most common in T9 and was present in 5 patients. No transverse process fracture was observed in T1 and T2.
Spinous process fractures were observed most frequently at T2 level and were present in 9 patients, while they were observed at least at T5 and T6 levels and were observed in 1 patient each.
Displaced rib fractures were most common in the 6th and 7th ribs and were observed in 8 patients each. On the left, it was seen in the 5th rib and in 6 patients. Non-displaced rib fractures were most common in the 5th rib on the right and in 9 patients, and on the left in the 5th rib and in 8 patients. Displaced rib fractures were seen in at least 2,9,10,11 and 12 ribs on the right and were present in 2 patients each. 1,2,3,10 ribs, 1 patient each on the left. No fracture was observed in the 12th rib. At least non-displaced fractures were seen in the 1st rib and 1 patient on the right, and in the 10th and 11th ribs and 3 patients on the left, but no non-displaced fractures were observed in the left 12th rib. When evaluated in general, vertebral fractures were most common at T8 level, and rib fractures were most common in the right side and 5th rib.
According to Leblebici HI, et al. in their study on 302 cases (263 men, 39 women), they found the frequency of multiple rib fractures to be 21.5% [27].
In 100 patients included in the study, rib fractures were most common on the right side and in the 5th and 9th ribs.
T7 only in patients with vertebral fracture. A significant relationship was found between the corpus vertebral and the gender variable (p<0.05). In the T7 corpus, only 1 fracture was seen in women, while 16 fractures were detected in men. The difference appears to be due to men.
In rib fractures, only a significant correlation was found between left 6th rib fracture and gender (p<0.05). In the left 6th rib, only non-displaced fracture was observed in women, while both non-displaced and displacement fractures were detected in men.
T2 and T3 spinous, T5 and T8 corpus fractures in patients with vertebral fracture were found to differ depending on the age variable and were statistically significant (p<0.05). In general, it was understood that this relationship was most common in patients aged 45-56 years and patients aged 30 years and younger.
T2 and T3 spinous, T5 and T8 corpus fractures in patients with vertebral fractures were found to differ depending on the age variable and were statistically significant (p<0.05). In general, it was understood that this relationship was most common in patients aged 45-56 years and patients aged 30 years and younger. T2 and T3 spinous, T5 and T8 corpus fractures in patients with vertebral fractures were found to differ depending on the age variable and were statistically significant (p<0.05).
It was determined that right 4,6,8,10 and left 2nd and 4th rib fractures in patients with rib fractures differed depending on the age variable and were statistically significant (p<0.05).
It was understood that this difference was caused by patients
aged 71 years and older in the right 4th, 6th and 8
Rib and vertebral fractures are common conditions that can cause mortality and morbidity and are secondary to trauma. It should be remembered that vertebral fractures may be common in patients due to trauma and may be accompanied by rib fractures. This coexistence should be taken into consideration in the planning of the diagnosis and treatment of patients.
The study was performed under a protocol approved by the Afyon Kocatepe University Medical Ethic Committee (2022/3).
The autors declare that they have no conflict of interests.
None.
All authors contributed equally.

