 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Hooria Hafeez1, Huma Aslam2, Aneel Kumar3, Imran Qureshi4, Hamed Sultan Albusaidi4, Parmanand Nathani4, Fatema Mohammed Khamis Al Sadairi4, Sanobar Bughio5* , Omar Rashid Al Hatmi6, Jaweria Naqi7
, Omar Rashid Al Hatmi6, Jaweria Naqi7
1Macclesfield District General Hospital, Victoria Rd, Macclesfield SK10 3BL, UK.
2South Tynside and Sunderland NHS foundation Trust UK.
3Specialist Radiologist, King's College Hospital London, Dubai UAE.
4Department of Radiology, Royal Oman Police Hospital, Oman.
5Specialist Radiologist, Royal Oman Police Hospital, Oman.
6Senior Medical Officer, Royal Oman Police Hospital, Oman.
7Shaheed Mohtrma Benazir Bhuto Medical college, Lyari, Karachi, Pakistan.
Correspondence to: Sanobar Bughio, Specialist Radiologist, Royal Oman Police Hospital, Oman.
Received date: October 11, 2024; Accepted date: October 24, 2024; Published date: October 31, 2024
Citation: Hafeez H, Aslam H, Kumar A, et al. Epiploic Appendigitis – Presenting as Acute Abdomen: Diagnostic Pitfalls and Clinical Insights. J Med Res Surg. 2024;5(5):121-123. doi: 10.52916/jmrs244150
Copyright: ©2024 Hafeez H, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Introduction: Epiploic appendigitis is a rare, benign, self-limiting inflammatory process of the epiploic appendices. The epiploic appendices are small pouches of the peritoneum filled with fat and situated along the colon, mainly the transverse and sigmoid parts, but are absent in the rectum and have an unknown function. These appendages can become acutely inflamed as a result of torsion or venous thrombosis. Case Report: A young patient came to emergency department of our hospital with complain of pain in abdomen at left lumber region since five days. On Physical examination revealed lump at left lumber region at the site of pain. Further investigated by radiological. Discussion: Epiploic appendigitis is an uncommon condition first described by Lynn et al in 1956 and is one of the rare causes of acute abdomen secondary to the inflammation and necrosis of small finger like projections along the colon. These appendages refer to adipose structures that rise in the surface of the colon and project into the abdominal cavity. Conclusion: Given the rarity of this condition, its elusive nature and tendency to mimic acute appendicitis, diverticulitis or cholecystitis, which all may require surgical intervention, it is increasingly apparent that we should educate medical professionals on this important differential diagnosis, as early and accurate diagnosis can prevent unnecessary invasive treatments and misdiagnosis.
Epiploic appendigites, CT scan, Ultrasound, Treatment.
Epiploic appendigitis is a rare, benign, self-limiting and local inflammatory condition that involves appendages across the large bowel to become inflamed causing symptoms that mimic conditions of acute abdominal pain, such as acute appendicitis, diverticulitis and cholecystitis. This is also referred to as primary (spontaneous) epiploic appendigitis, along with the term omental infarction, and is grouped under the broader umbrella term intraperitoneal focal fat infarction [1,2].
They develop in the second trimester of fetal life and grow during adulthood, reaching a length of 0.5cm to 15cm and 2cm thick, located along the sigmoid colon 57%, ileocecal 26%, ascending colon 9%, transverse colon 6% and descending colon 2% respectively [3]. Torsion and inflammation are the most common causes of primary epiploic appendigitis [4].
Symptoms typically include acute onset of abdominal pain, commonly to the left lower quadrant and sometimes reports of nausea, vomiting, fever and diarrhea, though these are uncommon. The gold standard for diagnosis is using imaging studies such as Computed Tomography (CT) [5], though ultrasound and Magnetic Resonance Imaging (MRI) have also been reported to have been useful diagnostic modalities. Advancements in technology has contributed to the increase in the diagnosis of this disease.
Here, we present a case of epiploic appendigitis that highlights the importance of imaging and clinical suspicion in guiding appropriate management.
Case ReportA young 30-year-old male came to the ER for subacute left lower quadrant abdominal pain lasting since 5-days, partially relieved by paracetamol. It is mainly an isolated pain and not associated with fever. He was sent for ultrasound abdomen and it showed an ovoid fat density area with thin enhancing rim and surrounding inflammatory fat stranding noted. An abdominal CT scan with IV contrast was done that showed a normal urinary tract and a non specific extra-intestinal epiploic inflammatory collection just at the sigmoid colon junction suggested by Heterogeneous area predominately fat density with thin enhancing rim and surrounding fat stranding associated with adjacent few sub centimeter lymph nodes; the aspect was typical of an acute epiploic appendigitis (Figure 1 (a,b,c)).
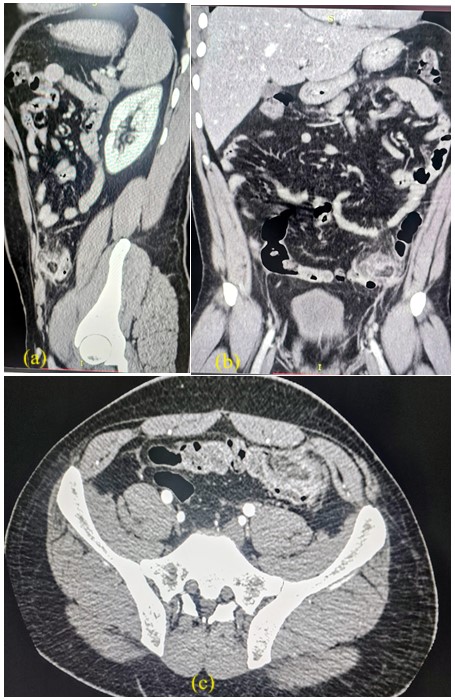 Figure 1: CT scan sagitale, coronal , and axial respectively shows typical of an acute epiploic appendigitis.
Figure 1: CT scan sagitale, coronal , and axial respectively shows typical of an acute epiploic appendigitis.The patient was discharged home on a symptomatic treatment composed by Non-Steroidal Anti-Inflammatory Drug (NSAID) and omeprazole for ten days; at the follow up visit, he was completely asymptomatic and the control abdominal CT scan done three weeks after the diagnosis showed that the collection has totally disappeared.
Epiploic appendigitis is an uncommon condition first described by Lynn et al in 1956 [6] and is one of the rare causes of acute abdomen secondary to the inflammation and necrosis of small fingerlike projections along the colon. These appendages refer to adipose structures that rise in the surface of the colon and project into the abdominal cavity [3]. They are found adjacent to the tenia coli of the colon from the caecum to the rectosigmoid in numbers of 50-100 distributed along the length of the large bowel.
Patients will typically present with acute onset severe abdominal pain commonly in the lower left quadrant, aggravated by coughing or stretching. The abdomen will be tender on palpation, they will describe pain getting progressively worse and there may be rebound tenderness present. Patients may also complain of nausea and very rarely vomiting. Clinical features will mimic acute appendicitis, diverticulitis, pelvic inflammatory disease and in women, ruptured ovarian cyst.
The incidence of cases where patients were initially suspected to have acute diverticulitis was reported to be 2-7% and 0.3- 1% patients were initially suspected to have acute appendicitis [7]. This only further highlights the importance of epiploic appendigitis being included in differential diagnosis for acute abdominal pain presentations.The condition usually affects patients in their 2nd-5th decades of life and studies report the presentation is slightly more common in males. The reported age range is between 12-82 years old [8]. It is usually associated with obesity, hernia and unaccustomed exercise.
The function of these is not completely clear but some suggest they act as a blood reservoir [7] providing cushioning, immunity and helping in colonic absorption. These appendages are pedunculated meaning they have arterial and venous supply and can become inflamed when there is limited blood flow, excessive mobility or pediculated morphology making them more susceptible to torsion with hemorrhage or ischemia [2]. They are visible on CT when inflamed or surrounded by fluid, seen as a central hyperdense dot and a fat-density ovoid structure adjacent to the colon, usually 1.5-3.5cm in diameter [1].
This particular case of epiploic appendigitis was first seen on ultrasound imaging performed over the patient’s area of maximal tenderness and then later confirmed on CT scan. On ultrasound we see a non-compressible, hyperechoic oval mass, surrounded by a hypoechoic peripheral ring, no central flow and increased echogenicity of the surrounding fat [1]. In earlier days, without radiological support diagnosis was made with exploratory laparotomy, however fortunately with technological advancements diagnosis has become easier and less invasive. Contrastenhanced CT remains the gold standard modality for diagnosing appendigitis and is often also performed to exclude other complications such as adherence to other viscera causing obstruction or abscess formation.
Laboratory findings and investigations are often unremarkable and within normal limits. They are often performed to exclude the possibility of infectious causes. The benefit of performing high quality imaging studies also serves as an important role in recognizing differential diagnoses of the disease avoiding unnecessary surgical procedures or antibiotic regimes. Though epiploic appendigitis is a self-limiting condition, symptomatic treatment with NSAIDs and painkillers is required. Most patients will often find symptoms resolve Most patients will often find symptoms resolve within 1-2 weeks of medical management at home and hospital admission is not typically required.
Given the rarity of this condition, its elusive nature and tendency to mimic acute appendicitis, diverticulitis or cholecystitis, which all may require surgical intervention, it is increasingly apparent that we should educate medical professionals on this important differential diagnosis, as early and accurate diagnosis can prevent unnecessary invasive treatments and misdiagnosis. The possibility of acute epiploic appendigitis should be considered in all patients clinically suspected to have acute appendicitis.

