 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Addajou Tarik* , Rokhsi Soukaina, Mrabti Samir, Benhamdane Ahlame, Sair Asmae, Berrida Reda, Elkoti Ilham, Rouibaa Fedoua, Benkirane Ahmed, Seddik Hassan
, Rokhsi Soukaina, Mrabti Samir, Benhamdane Ahlame, Sair Asmae, Berrida Reda, Elkoti Ilham, Rouibaa Fedoua, Benkirane Ahmed, Seddik Hassan
Department of Gastroenterology, Military Hospital Mohammed V, Rabat, Morocco
Correspondence to: Addajou Tarik, Department of Gastroenterology, Military Hospital Mohammed V, Rabat, Morocco
Received date: May 28, 2022; Accepted date: June 13, 2022; Published date: June 20, 2022
Citation: Tarik A, Soukaina R, Samir M, et al. (2022) Endoscopic Biliary Drainage in the Palliative Treatment of Klatskin Tumours: Outcomes and Factors Associated
with Success or Failure. J Med Res Surg 3(3): pp. 47-49. doi: 10.52916/jmrs224078
Copyright: ©2022 Tarik A, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted
use, distribution and reproduction in any medium, provided the original author and source are credited
Background: Klatskin's tumour is a cholangiocarcinoma that develops from the right or left bile ducts and the upper part of the main bile duct. They are usually diagnosed at an advanced, inoperable stage, and have an extremely poor prognosis. Biliary drainage is proposed in palliative situation and carries a high risk of infectious complications. The aim of our work is to report the results of endoscopic biliary drainage as well as the factors associated with its success or failure.
Methods: This is a retrospective and analytical study of 75 patients, conducted between July 2009 and August 2021, including all patients admitted with Klatskin's tumour and for whom endoscopic drainage was indicated. Factors associated with the success or failure of endoscopic treatment were studied by logistic regression analysis.
Results: The average age of our patients was 62.67 years with a male predominance of 68%. Cholangiocarcinoma was classified as bismuth IV in 50.6% of patients, bismuth IIIa in 30% of patients, bismuth IIIb in 13% of patients and bismuth II in 6% of patients. Sixteen percent of patients had liver metastases. Endoscopic drainage was successfully performed in 81.3% of patients by plastic prosthesis in 32% of cases, by a metal prosthesis in 45.2% and by nasobiliary drain in 4.1% . Forty-seven percent of patients had dilatation of the stenosis prior to prosthesis placement. Causes of stenting failure were primarily related to failure of papilla catheterisation, failure to pass the guidewire through the stenosis, or duodenal invasion by the tumour. In multivariate analysis and by adjusting the studied parameters, namely the age, gender, bismuth tumour type, presence of metastases and endoscopic dilatation of the stenosis, only the presence of metastases, endoscopic dilatation of the stenosis and the bismuth tumour classification affect the success rate. Indeed, endoscopic dilatation of the stenosis prior to stenting increases the success rate fourfold. Prosthesis increases the success rate by a factor of 4 [OR=4; p=0.01], whereas the presence of metastases decreases this rate by 65% [OR=0.35; p<0.001]. However, tumours classified as bismuth IV [OR=8; p<0.001] or bismuth IIIa [OR=5; p=0.004] were associated with a risk of endoscopic treatment failure.
Conclusion: Our study suggests that the presence of metastatic hilar cholangiocarcinoma classified as bismuth IV or bismuth IIIa appear to be associated with failure of endoscopic biliary drainage, whereas endoscopic dilatation prior to prosthesis placement appears to be associated with success.
Endoscopic biliary drainage, Klatskin tumours, Palliative treatment
Klatskin's tumour is a cholangiocarcinoma that develops from the right or left bile ducts and the upper part of the main bile duct. They are usually diagnosed at an advanced, inoperable stage, and have an extremely poor prognosis. Biliary drainage is proposed in palliative situation and carries a high risk of infectious complications.
Endoscopic Retrograde Cholangiopancreatography (ERCP) is frequently used in the management of patients with malignant hilar biliary obstruction that includes Klatskin tumor.
In this retrospective study, we analyzed our experience of ERCP in patients with Klatskin tumors; the aim of our work is to report the results of endoscopic biliary drainage as well as the factors associated with its success or failure.
Study design, setting, and participants: This is a retrospective and analytical study of 75 patients, conducted between July 2009 and August 2021 in the endoscopic Department of Mohammed V Military Hospital, Rabat, Morocco. We included all patients admitted with Klatskin's tumour and for whom endoscopic drainage was indicated.
Variables: We extracted the epidemiological history, demographic data, comorbidities, as well as the radiological, operative and evolutionary data.
Statistical analysis: Descriptive data are presented as means (± Standard Deviation (SD)) for normally distributed continuous variables. Categorical variables were presented as counts and percentages.
We performed logistic regression with adjustment for potential confounders to calculate Odds Ratios (ORs) and 95% Confidence Intervals (CIs) to identify the factors associated with the success or failure for the endoscopic biliary drainage of Klatskin's tumour.
A two-tailed P-value of <0.05 was considered statistically significant. All statistical analyses were performed using Statistical Package for the Social Sciences (SPSS) version 22.0 program.
The average age of our patients was 62.67 +/- 12 years with extremes ranging from 31 years to 93 years. Our series was characterised by a male predominance of 68% with a sex ratio of 2.12.
Cholangiocarcinoma was classified as bismuth IV in 50.6% of patients, bismuth IIIa in 30% of patients, bismuth IIIb in 13% of patients and bismuth II in 6% of patients (Figure 1).
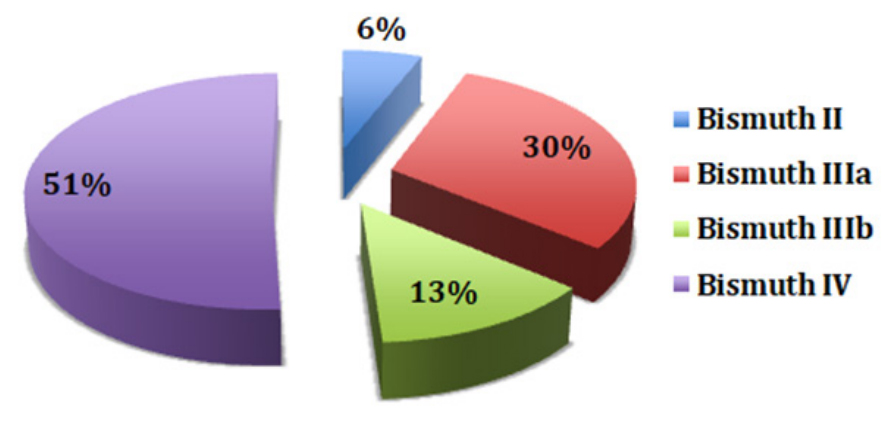 Figure 1:Repartition-according to Bismuth classification
Figure 1:Repartition-according to Bismuth classificationSixteen percent of patients had liver metastases.
Endoscopic drainage was successfully performed in 81.3% of patients by using plastic prosthesis in 32% of cases (n=24), a metal prosthesis in 45.2% (n=34) and by using nasobiliary drain in 4.1% (n=3) (Figure 2).
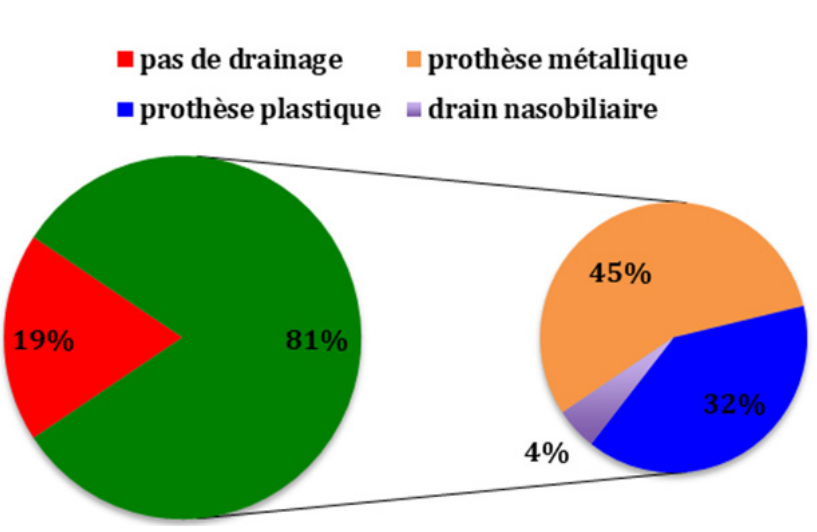 Figure 2:Results-of-biliary drainage and repartition according to the used method
Figure 2:Results-of-biliary drainage and repartition according to the used methodForty-seven percent of patients (n=35) had dilatation of the stenosis prior to prosthesis placement.
Causes of stenting failure were primarily related to failure of papilla catheterisation, failure to pass the guidewire through the stenosis, or duodenal invasion by the tumour.
In multivariate analysis and by adjusting the studied parameters, namely age, gender, Bismuth tumour type, presence of metastases and endoscopic dilatation of the stenosis, only the presence of metastases, endoscopic dilatation of the stenosis and the bismuth tumour classification affect the success rate (Table 1).
| Study parameters | Odds Ratio (OR) | 95% Confidence Interval (CI) | p |
| Age | 0.855 | 0.782-1.004 | 0.85 |
| Gender (female) | 1.867 | 1.012-3.444 | 0.46 |
| Bismuth tumour type (Bismuth IV) | 8 | 6.429-12.578 | <0.001 |
| Bismuth tumour type (Bismuth IIIa) | 5 | 2.561-11.738 | 0.004 |
| Presence of metastases | 0.35 | 0.023-1.175 | <0.001 |
| Endoscopic dilatation of the stenosis | 4 | 2.193- 6.968 | 0.01 |
Indeed, endoscopic dilatation of the stenosis prior to stenting increases the success rate fourfold. Prosthesis increases the success rate by a factor of 4 [OR=4; p=0.01], whereas the presence of metastases decreases this rate by 65% [OR=0.35; p<0.001]. However, tumours classified as bismuth IV [OR=8; p<0.001] or bismuth IIIa [OR=5; p=0.004] were associated with a risk of endoscopic treatment failure.
Although Klatskin tumor, or hilar cholangiocarcinoma, is a relatively rare tumor of the hepatobiliary system, it presents a major management challenge to clinicians [1].
However, due to this carcinoma high predisposition to early local invasion of adjacent vital structures by neural, perineural, subepithelial, and lymphatic spread, the prognosis of these patients is usually guarded [2].
In about 90% of patients with Klatskin tumors who are considered unsuitable or unfit for curative resection at presentation because of advanced disease or concomitant illness, palliative treatment seems worthwhile because the quality of life can be improved considerably by relief of the pruritus and nausea of cholestasis [3].
Even in the best hands, surgical bypass procedures were reported to have a 33% operative mortality, while surgical intubation carried a 60-day postopera- tive morbidity of 26% and a mortality of 30% [4]. Non-operative drainage, either percutaneous or endoscopic, has been recommended as the treatment of choice for palliation in patients with malignant hilar biliary obstruction that includes Klatskin tumor [5], especially in patients with high operative risk and limited life expectancy [6].
A high (19%) morbidity rate for endoscopic stenting and a procedure-related mortality of 3% have been reported in patients with malignant hilar biliary obstruction [7].
In contrast to patients with distal bile duct obstruction who can usually be adequately palliated with a single endoscopic stent, patients with Klatskin tumors often have segmental bile duct involvement, and complete biliary drainage is often impossible despite the insertion of multiple stents. Ineffective drainage of segmental ducts including the caudate branch may result in sepsis, especially after opacification during endoscopic examination. In patients in whom initial satisfactory biliary drainage is achieved, progressive tumor growth can occur, producing segregation of segmental ducts and thus resulting in poor long-term palliation by endoscopic stenting [8].
Our study suggests that the presence of metastatic hilar cholangiocarcinoma classified as bismuth IV or bismuth IIIa appear to be associated with failure of endoscopic endoscopic biliary drainage of Klatskin's tumours, whereas endoscopic dilatation prior to prosthesis placement appears to be associated with success.
The patient has consented to the submission of the case report to the journal.
No.

