 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Maram Alkhatieb1,2 , Rahaf Alrayiqi2, Omar A. Alsulami2*, Ziyad M. Albassam2, Sahal M. Wali2, Haifa Alnahdi2,3
, Rahaf Alrayiqi2, Omar A. Alsulami2*, Ziyad M. Albassam2, Sahal M. Wali2, Haifa Alnahdi2,3
1Division of General Surgery, Faculty of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia
2Faculty of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia
3Division of Endocrinology, Department of Internal Medicine, King Abdulaziz University Hospital, Jeddah, Saudi Arabia
Correspondence to: Omar A. Alsulami, Faculty of Medicine, King Abdulaziz University, Jeddah, Saudi Arabia
Received date: August 01, 2022; Accepted date: August 11, 2022; Published date: August 18, 2022
Citation: Alkhatieb M, Alrayiqi R, Alsulami OA, et al. Common Pathogens Isolated from Infected Diabetic Foot Ulcers at King Abdulaziz University Hospital, Saudi Arabia: A Retrospective Study. J Med Res Surg. 2022; 3(4): 71-78. doi: 10.52916/jmrs224084
Copyright: ©2022 Alkhatib M, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Objectives: To determine the common pathogens isolated from DFI to administer appropriate antibiotic treatment, followed by surgical interventions. Methods: A retrospective study was performed on 260 patients who presented with diabetic foot at King Abdulaziz University Hospital, Jeddah, Saudi Arabia, from October 2014 to September 2020. All patients underwent swabs and tissue culture for microbiological evaluation. Patient medical records were reviewed to collect demographic and clinical data, including Glycated Hemoglobin (HgA1C), Diabetes Mellitus (DM) type, duration of diabetes, swab, tissue culture, type of surgery, and type of isolated organism. Results: Escherichia coli was the most common organism isolated from the feet of diabetic patients, followed by Staphylococcus aureus, Klebsiella pneumoniae, Streptococcus agalactiae, and Pseudomonas aeruginosa. Amputations were significantly higher in patients who did not have Staphylococcus aureus or Pseudomonas aeruginosa infection, with no significant relationship between amputation and any other isolated organisms. A significant negative correlation between patient age and HgA1C level was discovered, as well as a significant positive correlation between HgA1C and the number of minor amputations. Patients with major and minor amputations had a significantly higher percentage of non-Multidrug Resistance (MDR), whereas patients with MDR had a significantly higher rate of infection with Klebsiella pneumoniae, Escherichia coli, Pseudomonas aeruginosa, or Staphylococcus aureus. Conclusion: DM is a metabolic syndrome that affects all the body systems and impacts both morbidity and mortality. The most common organism isolated from the feet of diabetic patients was Escherichia coli, followed by Staphylococcus aureus. Ulcer specimens should be collected for culture and identification of causative organisms. Preventive measures such as good glycemic control, appropriate foot care, targeted antibiotic therapy, and patient education can reduce the incidence of amputation.
Pathogen, Isolated, Diabetic, Foot, Ulcers, Diabetic foot
BMI: Body Mass Index; DFI: Diabetic Foot Infections; DFU: Diabetic Foot Ulcers; DM: Diabetes Mellitus; MDR: Multidrug Resistance.
Diabetes Mellitus (DM) is a metabolic syndrome characterized by hyperglycemia, which can be caused by a decrease in insulin secretion, a defect in insulin activity, or both, causing serious damage to the heart, kidneys, eyes, blood vessels, nerves, and causing diabetic foot ulcers [1]. Diabetes is more prevalent in developing countries than in developed countries [2].
Saudi Arabia is ranked fifth worldwide for the prevalence of type 1 diabetes in children aged 0-14 years, with an estimated incidence of 31 per 100,000. Diabetes is estimated to affect 18% of adults in Saudi Arabia [3]. Neuropathy affects approximately 15.8% of Saudi patients with diabetes [1]. The World Health Organization defines Diabetic Foot Ulcers (DFUs) as foot ulcers associated with neuropathy, varying degrees of ischemia, and infection [4]. The proportion of people with diabetes with a history of foot ulceration is understandably higher than the proportion who have an active ulcer; 3.1-11.8% of people with diabetes, or 12.9-49.0 million people worldwide, have a history of foot ulceration [5-7].
Diabetic Foot Infections (DFIs) account for up to 20% of all diabetes-related hospitalizations in both Europe and the US, making it the single most common cause of DM-related hospital admissions and one of the leading causes of amputation. Diabetes is the most common cause of non-traumatic amputation and is usually precipitated by the development of a chronic wound, which is clinically defined as a wound that does not heal within 30 days. According to previous studies, the presence of DFI increases the risk of lower extremity amputation by 50% compared to DFU without infection [8-12].
The etiology of DFU is multifactorial, with diabetic peripheral neuropathy, peripheral arterial disease, and foot deformity being the most common. DFI, which has been found to be present in 40-60% of all DFU patients, is another major contributor to DFU outcomes [13,14]. DFI is clinically diagnosed as the presence of two or more cardinal signs of inflammation (pain, erythema, fever, induration, and purulent discharge) and is regarded as a major health problem [9].
DFI is classified as mild, moderate, or severe and are commonly polymicrobial [9,15]. A wide variety of microbiological organisms found in DFI have been reported in the literature. Aerobic grampositive cocci, primarily Staphylococcus aureus, are the most commonly isolated organisms in North America and Europe, whereas aerobic gram-negative organisms are more common in Asia and Africa [16].
An appropriate treatment strategy for moderate-to-severe DFIs includes empirical broad-spectrum antibiotics tailored to the local bacterial profile. Previous studies have demonstrated that treatment success depends on the severity of infection, patients’ comorbidities, early surgical drainage, and debridement [15,16].
Few studies have been conducted to identify the most common pathogens isolated from DFI in Saudi Arabia. Therefore, this study aimed to identify the common pathogens isolated from DFI to apply proper targeted antibiotic treatment followed by surgical interventions.
Study design, setting, and duration
This retrospective study was conducted from September 2021
to October 2021 at King Abdulaziz University Hospital, Jeddah,
Saudi Arabia.
Study participants
Data were collected retrospectively from 260 patients
who presented with diabetic foot in the study setting from
October 2014 to September 2020. All patients who presented
with diabetic foot, which was confirmed using swabs and
tissue culture for microbiological evaluation, were included.
Nondiabetic patients with foot ulcers were excluded.
Study instrument
A checklist was prepared to collect patients’ demographic
and clinical data, such as Body Mass Index (BMI), Glycated
Hemoglobin (HgA1C), DM type, duration of diabetes, swab,
tissue culture, type of surgery, and type of isolated organism.
All data were obtained from patients’ medical records.
Ethical considerations
Ethical approval for this study was obtained as a signed paper
from the Institutional Review Board of King Abdulaziz University
Hospital (Approval No. 1-21). Written informed consent was
obtained from each participant.
Statistical analysis
Data were analyzed using the SPSS version 26 (IBM® SPSS® Statistics, Chicago, USA). Qualitative data were expressed as
numbers and percentages, and the chi-square test (χ2) was applied to test the relationship between variables. Quantitative
data are expressed as mean and standard deviation (mean ±
SD). Statistical significance was set at p <0.05.
This study included 260 patients whose mean age was 63.04 ±13 years; 69.2% were males, 36.2% had a Saudi nationality, and 71.5% had DM type 2 (Table 1). Among the study population, 30.4%, 26.5%, and 10.4% had dry, wet, and gas gangrene, respectively. Almost half of the patients (51.2%) had chronic ulcers, 79.6% were admitted through the ER, 64.6% were receiving insulin on a treat to target titration schedule, and 81.9% had foot infection. Most patients (83.8%) had comorbid chronic diseases, including hypertension (74.2%) and cardiovascular disease (30.8%). The mean number of chronic diseases was 1.39 ± 1.03.
| Variable | No. (%) |
| Age (years) | 63.04 ± 13 |
| Sex | |
| Female | 80 (30.8) |
| Male | 180 (69.2) |
| Nationality | |
| None-Saudi | 166 (63.8) |
| Saudi | 94 (36.2) |
| Diabetes type | |
| NA | 23 (8.8) |
| Type 1 | 51 (19.6) |
| Type 2 | 186 (71.5) |
| Dry gangrene | |
| No | 181 (69.6) |
| Yes | 79 (30.4) |
| Wet gangrene | |
| No | 191 (73.5) |
| Yes | 69 (26.5) |
| Gas gangrene | |
| No | 233 (89.6) |
| Yes | 27 (10.4) |
| Chronic ulcer | |
| No | 127 (48.8) |
| Yes | 133 (51.2) |
| Site of admission | |
| ER | 207 (79.6) |
| NA | 12 (4.6) |
| Outpatient | 41 (15.8) |
| Chronic diseases | |
| Yes | 218 (83.8) |
| No | 42 (16.2) |
| If yes: what type? (No.: 218) | |
| CVD | 80 (30.8) |
| DM | 26 (10) |
| CKD | 52 (20) |
| HTN | 193 (74.2) |
| Number of chronic diseases | 1.39 ± 1.03 |
| Insulin ttt | |
| NA | 27 (10.4) |
| No | 65 (25) |
| Yes | 168 (64.6) |
| Foot infection | |
| NA | 22 (8.5) |
| No | 25 (9.6) |
| Yes | 213 (81.9) |
| CVD: Cardiovascular Disease; DM: Diabetes Mellitus; CKD: Chronic Kidney Disease; HTN: Hypertension | |
Approximately 25.8% of patients had osteomyelitis, and 54.2% had a surgical history, with a mean number of surgeries of 1.31 ± 1.3 (Table 2). Overall, 21.2% (one-fifth) of the patients had co-infection, while 58.1% had a single infection. Of the 260 patients, 25.8% had Multidrug Resistance (MDR) and 86.9% had amputations, with a mean number of amputations of 1.38 ± 0.87. More than half of the patients (55.8%) had minor amputation, with a mean number of amputations of 0.74 ± 0.8 and with 16.2% of amputations through the metatarsal bones.
Overall, 50% of the patients underwent major amputation, with a mean number of amputations of 0.67 ± 0.76 and with 30.8% of amputations above the knee. Fewer patients (24.6%) underwent debridement, and the mean hospital stay was 21.16 ± 32.53 days.
The mean values of BMI and laboratory results are shown in (Table 2). The most commonly isolated organisms were Escherichia coli (16.9%), Staphylococcus aureus (10.8%), Klebsiella pneumoniae (9.6%), Streptococcus agalactiae (8.5%), Pseudomonas aeruginosa (7.3%), Morganella morganii (5.8%), and Proteus mirabilis (5%) (Figure 1). There was no significant relationship between amputation and the isolated organisms listed in (Tables 3 and 4) (p> 0.05), except for Staphylococcus aureus (p< 0.001), as shown in (Figure 2) (Table 3). Patients who had no Staphylococcus aureus infection had a significantly higher incidence of amputation (major and minor) (p< 0.001) (Figure 2). There was no significant relationship between minor amputations and the isolated organisms (p> 0.05), and the same applies to major amputations, except for Pseudomonas aeruginosa and Staphylococcus aureus infection (p< 0.05) (Table 4). Patients who had no Pseudomonas aeruginosa or Staphylococcus aureus infection had a significantly higher incidence of amputation (p> 0.05) (Figures 3 and 4).
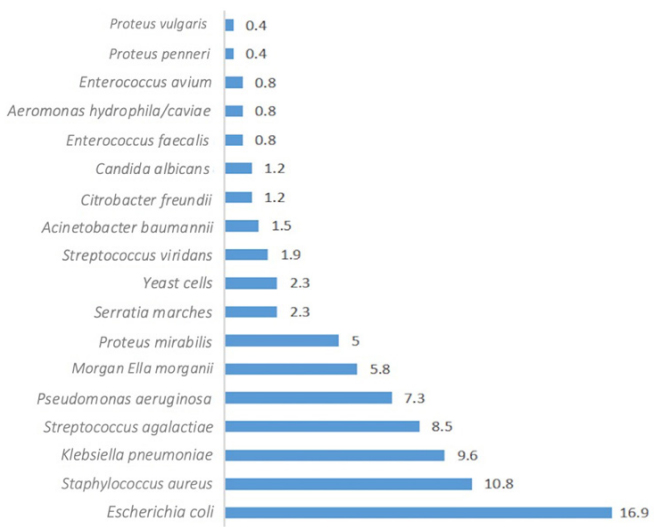 Figure 1: Percentage distribution of isolated organisms from diabetic foot
ulcers.
Figure 1: Percentage distribution of isolated organisms from diabetic foot
ulcers.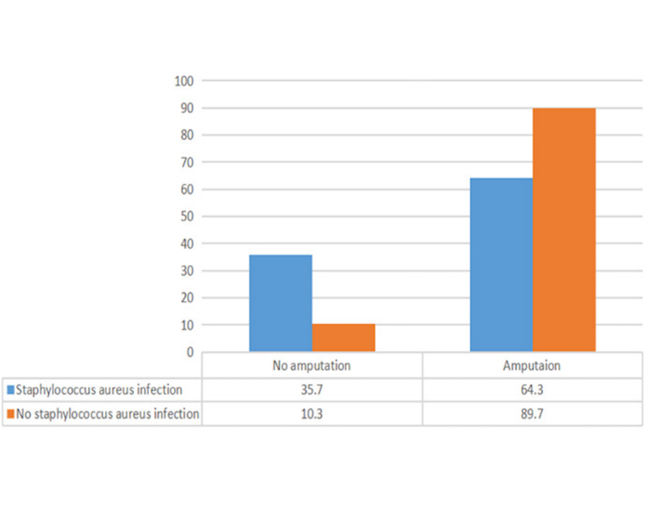 Figure 2: Relationship between amputation and Staphylococcus aureus
infection.
Figure 2: Relationship between amputation and Staphylococcus aureus
infection.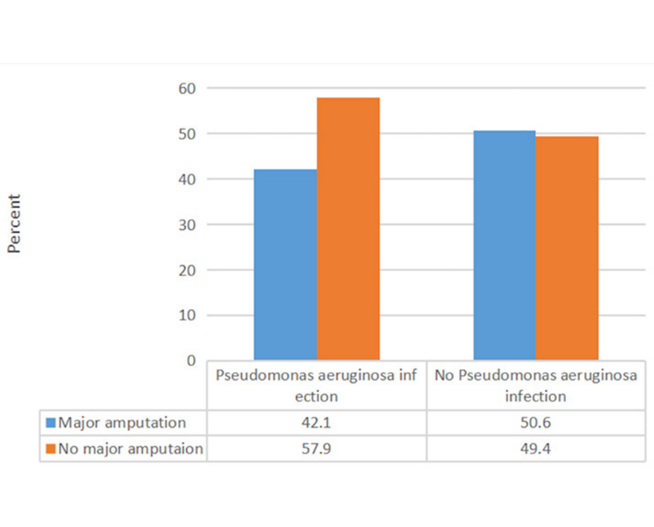 Figure 3: Relationship between major amputations and Pseudomonas aeruginosa infection.
Figure 3: Relationship between major amputations and Pseudomonas aeruginosa infection.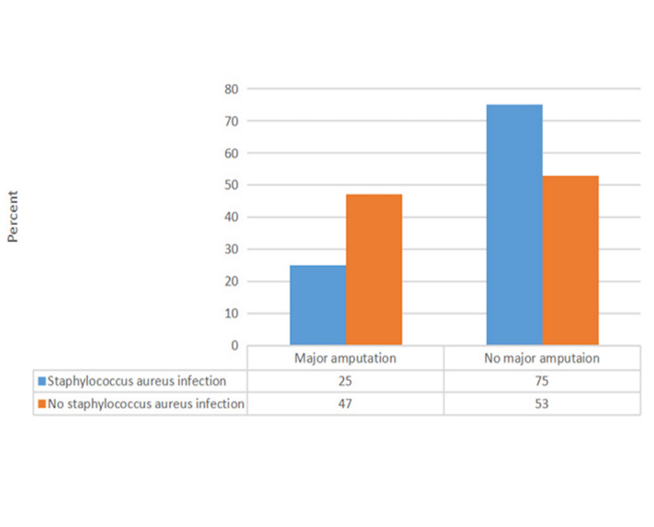 Figure 4: Relationship between major amputation and Staphylococcus aureus infection.
Figure 4: Relationship between major amputation and Staphylococcus aureus infection.| Variable | No. (%) |
| Osteomyelitis | |
| N/A | 95 (36.5) |
| No | 98 (37.7) |
| Yes | 67 (25.8) |
| Surgical history | |
| NA | 47 (18.1) |
| No | 72 (27.7) |
| Yes | 141 (54.2) |
| Number of surgeries | 1.31 ±1.3 |
| Co-infection | |
| Single infection | 151 (58.1) |
| Co-infection | 55 (21.2) |
| No organism or NA | 54 (20.8) |
| MDR | |
| NA | 46 (17.7) |
| No | 147 (56.5) |
| Yes | 67 (25.8) |
| Amputation | |
| No | 34 (13.1) |
| Yes | 226 (86.9) |
| Number of amputations | 1.38 ± 0.87 |
| Minor amputation | |
| No | 115 (44.2) |
| Yes | 145 (55.8) |
| Number of minor amputations | 0.74 ± 0.8 |
| Level of minor amputation | |
| Above_knee | 2 (0.8) |
| Below_Knee | 13 (5) |
| Great_toes_or_first_ray | 36 (13.8) |
| N/A | 115 (44.2) |
| Other_toes | 41 (15.8) |
| Through_ankle_or_Taurus | 2 (0.8) |
| Through_metatarsal_bones | 42 (16.2) |
| Through_tarsometatarsal_joints | 9 (3.5) |
| Major amputation | |
| NA | 0.4 |
| No | 129 (49.6) |
| Yes | 130 (50) |
| Number of major amputations | 0.67 ± 0.76 |
| Level of major amputation | |
| Above_knee | 80 (30.8) |
| Below_Knee | 56 (21.5) |
| Hip | 2 (0.8) |
| N/A | 121 (46.5) |
| Through_knee | 1 (0.4) |
| Debridement | |
| NA | 91 (35) |
| No | 105 (40.4) |
| Yes | 64 (24.6) |
| Hospital stay (days) | 21.16 ± 32.53 |
| Mean values | |
| BMI | 26.88 ± 7.4 |
| WBC | 16.4 ± 11.32 |
| Hg | 9.19 ± 3.08 |
| HgAIC | 6.95 ± 5.88 |
| CRP | 62.94 ± 95 |
| ESR | 61.53 ± 48.01 |
| Creatinine | 175.8 ± 201.42 |
| MDR: Multidrug Resistant Bacteria; N/A: Not Available; BMI: Body Mass Index; WBC: White Blood Cells; Hg: Hemoglobin; HgAIC: Glycated Hemoglobin; CRP: C-Reactive Protein; ESR: Erythrocyte Sedimentation rate. | |
| Variable | Amputation |
χ2 |
p-value |
|
No No. (%) |
Yes No. (%) |
|||
| Enterococcus faecalis | 0 (0.0) |
2 (100) |
0.3 |
0.582 |
| Acinetobacter baumannii | 1 (25) |
3 (75) |
0.5 |
0.476 |
| Streptococcus viridans | 1 (20) |
4 (80) |
0.21 |
0.643 |
| Klebsiella pneumonia | 3 (12 |
22 (88) |
0.02 |
90.867 |
| Morganella morganii | 0 (0.0) |
15 (100) |
2.39 |
0.122 |
| Escherichia coli | 7 (15.9) |
37 (84.1) |
0.36 |
0.549 |
| Streptococcus agalactiae | 3 (13.6) |
19 (86.4) |
0.007 |
0.935 |
| Pseudomonas aeruginosa | 1 (5.3) |
18 (94.7) |
1.1 |
0.294 |
| Citrobacter freundii | 0 (0.0) |
3 (100) |
0.45 |
0.499 |
| Aeromonas hydrophilic/caviae | 0 (0.0) |
2 (100) |
0.3 |
0.582 |
| Enterococcus avium | 0 (0.0) |
1 (100) |
0.15 |
0.698 |
| Candida albicans | 0 (0.0) |
3 (100) |
0.45 |
0.499 |
| Serratia marches | 0 (0.0) |
6 (100) |
0.92 |
0.336 |
| Proteus mirabilis | 1 (7.7) |
12 (92.3) |
0.34 |
0.555 |
| Proteus penneri | 0 (0.0) |
1 (100) |
0.15 |
0.698 |
| Proteus vulgaris | 0 (0.0) |
1 (100) |
0.15 |
0.698 |
| Yeast cells | 1 (16.7) |
5 (83.3) |
0.07 |
0.792 |
| Variable | Minor amputation No. (%) |
χ2 (p-value) |
Major amputation No. (%) |
χ2 (p-value) |
| Enterococcus faecalis | 2 (100) |
-0.206 |
1 (50) |
-0.996 |
| Acinetobacter baumannii | 3 (75) |
-0.435 |
1 (25) |
-0.591 |
| Streptococcus viridans | 3 (60) |
-0.847 |
1 (20) |
-0.389 |
| Klebsiella pneumonia | 15 (60) |
-0.654 |
11 (44) |
-0.766 |
| Morganella morganii | 11 (73.3) |
-0.158 |
9 (60) |
-0.713 |
| Escherichia coli | 25 (56.8) |
-0.903 |
21 (47.7) |
-0.854 |
| Streptococcus agalactiae | 14 (63.6) |
-0.437 |
6 (27.3) |
-0.076 |
| Pseudomonas aeruginosa | 12 (63.2) |
-0.501 |
8 (42.1) |
-0.002 |
| Staphylococcus aureus | 13 (46.4) |
-0.292 |
7 (25) |
-0.017 |
| Citrobacter freundii | 3 (100) |
-0.121 |
1 (33.3) |
-0.836 |
| Aeromonas hydrophila/caviae | 2 (100) |
-0.206 |
1 (50) |
-0.996 |
| Enterococcus avium | 0 (0.0) |
-0.261 |
1 (100) |
-0.605 |
| Candida albicans | 3 (100) |
-0.121 |
2 (66.7) |
-0.843 |
| Serratia marches | 3 (50) |
-0.773 |
3 (50) |
-0.988 |
| Proteus mirabilis | 10 (79.9) |
-0.115 |
6 (46.2) |
-0.931 |
| Proteus penneri | 0 (0.0) |
-0.261 |
1 (100) |
-0.605 |
| Proteus vulgaris | 0 (0.0) |
-0.261 |
1 (100) |
-0.605 |
| Yeast cells | 1 (16.7) |
-0.051 |
5 (83.3) |
-0.255 |
There was a significant weak negative correlation between patient age and HgA1C (r=- 0.16, p-value=0.015), while a significant positive correlation was found between HgA1C and the number of minor amputations (r=0.22, p=0.001) (Table 5). Patients with a HgA1C level < 7% had a significantly higher percentage of minor amputations (p< 0.05) (Table 6). However, a non-significant relationship was found between HgA1C levels and major amputations (p> 0.05). A significantly higher percentage of those who cultured drug-sensitive organisms underwent a minor amputation only (p<0.001) (Table 7). The details of the MDR status of the isolated organisms are shown in (Table 8).
| Variable | HgA1C |
|
R |
P-value |
|
| Age | -0.16 |
0.015 |
| Diabetes duration | -0.15 |
0.317 |
| Number of chronic diseases | -0.05 |
0.388 |
| Number of surgeries | 0.07 |
0.322 |
| Number of all amputations | 0.09 |
0.179 |
| Number of minor amputations | 0.22 |
0.001 |
| Number of major amputations | -0.12 |
0.053 |
| Hospital stay (days) | 0.06 |
0.33 |
| Variable | HgAIC |
χ2 |
p-value |
||
< 7 |
7.1-10 |
> 10 |
|||
| Minor amputation | |||||
| No | 57 (57.6) |
22 (22.2) |
20 (20.2) |
9.31 |
0.009 |
| Yes | 48 (37.5) |
46 (35.9) |
34 (26.6) |
- |
- |
| Major amputation | |||||
| ND | 1 (100) |
0 (0.0) |
0 (0.0) |
8.55 |
0.073 |
| No | 44 (39.6) |
32 (28.8) |
35 (31.5) |
- |
- |
| Yes | 60 (52.2) |
36 (31.3) |
19 (16.5) |
- |
- |
| HgAIC: Hemoglobin A1C, ND: Not Detected | |||||
| Variable | MDR |
χ2 | p-value |
||
N/A |
No |
Yes |
|||
| Amputation | |||||
| No | 2 (5.9) |
26 (76.5) |
6 (17.6) |
6.83 |
0.033 |
| Yes | 44 (19.5) |
121 (53.5) |
61 (27) |
- |
- |
| Minor amputation | |||||
| No | 26 (22.6) |
62 (53.9) |
27 (23.5) |
- |
- |
| Yes | 20 (13.8) |
85 (58.6) |
40 (27.6) |
- |
- |
| Major amputation | |||||
| ND | 0 (0.0) |
0 (0.0) |
1 (100) |
21.31 |
< 0.001 |
| No | 10 (7.8) |
85 (65.9) |
34 (26.4) |
- |
- |
| Yes | 36 (27.7) |
62 (47.4) |
32 (24.6) |
- |
- |
MDR: Multidrug Resistant, ND: Not Detected, NA: Not Available |
|||||
| Variable | MDR |
χ2 |
p-value |
||
N/A |
No |
Yes |
|||
| Enterococcus faecalis | 0 (0.0) |
2 (100) |
0 (0.0) |
1.54 |
0.461 |
| Acinetobacter baumannii | 0 (0.0) |
4 (100) |
0 (0.0) |
3.12 |
0.21 |
| Streptococcus viridans | 0 (0.0) |
5 (100) |
0 (0.0) |
3.91 |
0.141 |
| Klebsiella pneumoniae | 0 (0.0) |
14 (56) |
11 (44) |
8.46 |
0.015 |
| Morgan Ella morganii | 0 (0.0) |
8 (53.3) |
7 (46.7) |
5.54 |
0.063 |
| Escherichia coli | 0 (0.0) |
24 (54.5) |
20 (45.5) |
17.75 |
< 0.001 |
| Streptococcus agalactiae | 0 (0.0) |
16 (72.7) |
6 (27.3) |
5.38 |
0.068 |
| Pseudomonas aeruginosa | 0 (0.0) |
9 (47.4) |
10 (52.6) |
9.67 |
0.008 |
| Staphylococcus aureus | 0 (0.0) |
17 (60.7) |
11 (39.3) |
7.87 |
0.02 |
| Citrobacter freundii | 0 (0.0) |
1 (33.3) |
2 (66.7) |
2.79 |
0.247 |
| Aeromonas hydrophila/caviae | 0 (0.0) |
2 (100) |
0 (0.0) |
1.54 |
0.461 |
| Enterococcus avium | 0 (0.0) |
1 (100) |
0 (0.0) |
0.77 |
0.68 |
| Candida albicans | 0 (0.0) |
3 (100) |
0 (0.0) |
2.33 |
0.311 |
| Serratia marches | 0 (0.0) |
3 (50) |
3 (50) |
2.53 |
0.282 |
| Proteus mirabilis | 0 (0.0) |
8 (61.5) |
5 (38.5) |
3.33 |
0.189 |
| Proteus penneri | 0 (0.0) |
0 (0.0) |
1 (100) |
2.89 |
0.236 |
| Proteus vulgaris | 0 (0.0) |
0 (0.0) |
1 (100) |
2.89 |
0.236 |
| Yeast cells | 0 (0.0) |
6 (100) |
0 (0.0) |
4.72 |
0.094 |
| MDR: Multidrug Resistance, N/A: Not Available | |||||
This retrospective study aimed to identify the common pathogens isolated from DFI to apply appropriate antibiotic treatment followed by surgical interventions, wherein data N.B.: (χ were collected retrospectively from 260 patients who presented with diabetic foot in the study setting from October 2014 to September 2020. We found that the most common isolated pathogen was the gram-negative Escherichia coli, which is in contrast with the finding that gram-positive bacteria are the most common pathogens isolated from diabetic foot ulcers [16].
The current study included a majority of male participants, which is consistent with the findings of other studies conducted locally and internationally [17,18]. Another finding from this study was that Escherichia coli was the most commonly isolated organism, followed by Staphylococcus aureus. This finding is consistent with the finding of a study conducted at King Khalid Hospital in Al Kharj city, Saudi Arabia, wherein Escherichia coli was the dominant anaerobic organism (22%), leading to the development of infectious processes and being distributed in a proximal direction along the synovial-tendon sheets of the foot [19]. Furthermore, our finding agrees with a previous Iranian study finding [20].
Our findings are also consistent with those of similar studies conducted in Kuwait and Lebanon, which found that gramnegative bacteria are more commonly isolated from DFIs, with Escherichia coli being the most common [21,22]. In contrast, Al Ayed et al. conducted a study in 2018 on 126 patients aged 40–70 years at the Prince Sultan Military Medical City in Riyadh, Saudi Arabia, using a swab culture method for microbiological testing and reported that Staphylococcus aureus was the most commonly isolated organism, followed by Pseudomonas aeruginosa [23]. The high incidence of gram-negative DFI in our region can be explained by multiple theories. The abuse of antibiotics could explain the predominance of gram-negative infections in our patients. Thus, initiating an appropriate empiric antibiotic treatment that covers gram-negative organisms in the Emergency Department for Patients presenting with diabetic foot infection is crucial and will improve the prognosis.
According to our study, 55% of the patients had minor metatarsal amputations, 50% had major above-knee amputations, and 24% had debridement. In comparison, a previous Saudi study reported minor toe amputation as the most common amputation [19]. According to the previously mentioned Iranian study [20], amputations were most frequently performed on the toes and below the knee. The higher number of aboveknee amputations in our data could be due to various factors, including later presentation because our hospital is a tertiary care center, type of diabetes, and the pathogen contributing to the infection.
According to a study conducted at Hebron Governmental Hospital between 2013 and 2020, the majority of the patients in the study had major amputations [24]. In our study, the majority of people who underwent amputation were infected with bacteria other than Staphylococcus aureus. A previous study found that gram-negative infections severely damage the tissue in diabetic feet and predispose patients to amputation [24].
This study observed a significant positive correlation between HgA1C and the number of minor amputations: patients with a HgA1C level of <7% were significantly more likely to require a minor amputation than patients with HgA1C level of >10%. This is in contrast with the findings of a previous study, which reported that patients who underwent amputation had poor glycemic control, were significantly older and less educated, and had longer hospital stays [25].
It was discovered that patients in the current study who had amputations (major or minor) and those who had minor amputations had a significantly lower percentage of MDR than those who did not. Infections of leg ulcers have a significant impact on patients and healthcare services; therefore, they must be detected early. DFIs can have a monomicrobial or polymicrobial etiology, and microorganisms could be resistant to one or more antibiotics [26-28]. In global comparisons, the most common causative organisms isolated in Western countries are gram-positive, particularly Methicillin-Sensitive Staphylococcus aureus (MSSA) [29].
The high incidence of gram-negative infections in our country has not yet been investigated, but it could be attributed to an era when antibiotics were available as over-the-counter medications. As a result, well-established guidelines for treating DFIs advocate empiric antibiotic regimens that cover these organisms.
This study has some limitations. The retrospective nature of the study design could have impacted the generalization of the study results. This study was conducted in a single center, and as such had a limited number of participants and some missing data, multicenter study design will overcome this limitation. There were insufficient studies on common pathogens isolated from infected diabetic foot ulcers in our nation, we recommend to do more studies.
DM is a metabolic syndrome that affects all the body systems and has an impact on both morbidity and mortality. One of the common complications in diabetic patients is diabetic foot ulcer, which is the single most common cause of DM-related hospital admissions and one of the leading causes of amputation. This study discovered that Escherichia coli was the most commonly isolated organism in the feet of diabetic patients, followed by Staphylococcus aureus. These results can serve as reference for local guidelines, aiming to improve patient outcomes and decrease and prevent bacterial resistance to antibiotics. Furthermore, preventive measures such as good glycemic control, appropriate foot care, well-adjusted antibiotic therapy, and patient education may significantly reduce the incidence of amputation among Saudi patients with diabetes. All treating physicians should collect appropriate specimens for culture and encourage clinical microbiology laboratories to report the genus of all organisms recovered from such specimens.
This research did not receive any specific grant from any funding agency in the public, commercial or not-for-profit sector.
The authors declare no competing financial interest.

