 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Imran Qureshi1*, Ghazala Hamid1, Jaweria Naqi2, Hamed Sultan Albusaidi Hamed1, Parmanand Nathani1, Fatema Mohammed Khamis Al Sadairi1, Sanobar Bughio3* , Tharaa Marhoon Almamari1, Darryl James Arguelles1, Fatima Said Albatashi1, Hooria Hafeez4, Mugilan saminathan1, Muath Salim Al Abri1, Rajkumar Johnwilliams1
, Tharaa Marhoon Almamari1, Darryl James Arguelles1, Fatima Said Albatashi1, Hooria Hafeez4, Mugilan saminathan1, Muath Salim Al Abri1, Rajkumar Johnwilliams1
1Department of Radiology, Royal Oman Police Hospital, Muscat, Oman.
2Shaheed Mohtrma Benazir Bhuto Medical College, Lyari, Karachi, Pakistan.
3Department of Radiology, Dr Ziauddin Hospital, Karachi, Pakistan.
4Macclesfield District General Hospital, Victoria Rd, Macclesfield SK10 3BL, UK.
Correspondence to: Imran Qureshi, Department of Radiology, Royal Oman Police Hospital, Muscat, Oman.
Received date: February 10, 2024; Accepted date: March 04, 2024; Published date: March 11, 2024
Citation: Qureshi I, Hamid G, Naqi J, et al. Cerebellar Tonsillar Herniation an Incidental Finding in Asymptomatic Patient. J Med Res Surg. 2024;5(1):10-12. doi: 10.52916/jmrs244128
Copyright: ©2024 Qureshi I, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted
use, distribution and reproduction in any medium, provided the original author and source are credited.
Cerebellar tonsillar herniation, often associated with Chiari malformation, involves the downward displacement of the cerebellar tonsils below the foramen magnum. This condition can lead to significant complications due to the limited intracranial space within the rigid skull. Timely diagnosis is crucial given its potentially fatal nature, with brain structural displacement evident on imaging studies. We present a case of a 27-year-old female with continuous headaches and dizziness, diagnosed with tonsillar herniation through MRI revealing 16 mm of tonsillar descent without associated hydrocephalus or syrinx. Tonsillar herniation, characterized by inferior descent of the cerebellar tonsils, may be congenital or acquired, with measurements typically referenced from the McRae line to the displaced tonsil tip. Complications include brainstem compression, obstruction of cerebrospinal fluid flow, syringomyelia, impaired blood flow, and various neurological and psychological symptoms. Management options vary based on symptom severity and may involve observation, medication, or surgical intervention to alleviate compression and improve cerebrospinal fluid flow. Consultation with a neurologist or neurosurgeon is essential for comprehensive evaluation and tailored management plans aiming to relieve pressure on the brainstem and spinal cord in tonsillar herniation cases.
Tonsillar, Herniation, Cerebellum, Chiari malformation, Hydrocephalus, Syringomyelia.
Cerebellar tonsillar herniation, precisely referring to the downward displacement of the cerebellar tonsils below the foramen magnum, tonsillar herniation can be categorized into congenital and acquired forms [1]. The McRae line is used as a reference for this measurement. It is obtained by drawing a line from the basion to the opisthio Assessment, attention was given to the cerebellar tonsils with a focus on two aspects first degree of herniation, this refers to the extent to which the cerebellar tonsils extend below the level of the foramen magnum, which is the opening at the base of the skull. Herniation of the cerebellar tonsils beyond their normal position can be associated with conditions like Chiari malformation second morphological Configuration this involves studying the shape and structure of the cerebellar tonsils. Variations in the morphological configuration may be indicative of certain medical conditions or abnormalities [2].
Cerebrospinal Fluid (CSF), blood, and the brain constitute the three main components placed in hard, vault-shaped skull. Bony landmarks and inelastic dural reflections serve as its partitioning elements [3]. Given the inflexible nature of the skull, the intracranial volume is set and has little space for expansion because of the rigid architecture of the skull [4].
A timely diagnosis of cerebral herniation is imperative due to its potentially fatal nature. Brain structural displacement can be clearly shown on imaging, which are characteristics of the various brain herniation subtypes should be recognized by the radiologist Radiological findings should be interpreted in the context of clinical signs and symptoms. The correlation between imaging findings and the patient's neurological status is crucial for an accurate diagnosis [5].
This case report describes as a 27 years old female came to the emergency department of our hospital with complaining of continuous headache for two months and dizziness, she was well oriented with time place and person no other comorbid . She was referred to the radiology department for a MRI brain. The sagittal and axial images of an MRI revealing 16 mm of tonsillar descent with posterior fossa crowding without associated hydrocephalus or syrinx as described in figure 1-4.
 Figure 1: Axial T1W shows tonsillar descend with anterior brainstem displacement and effacement of CSF in the foramen magnum.
Figure 1: Axial T1W shows tonsillar descend with anterior brainstem displacement and effacement of CSF in the foramen magnum.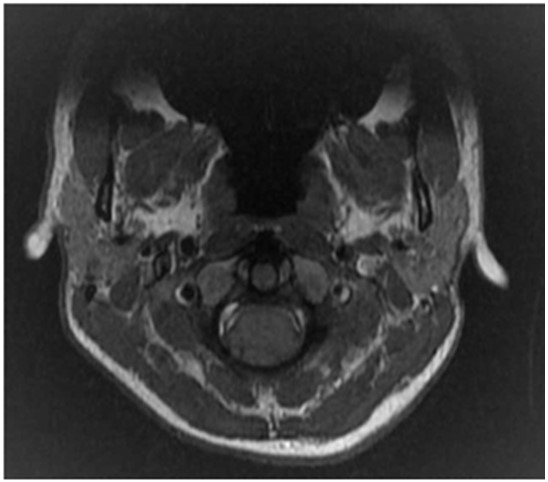 Figure 2: Axial T2W shows tonsillar descend with anterior brainstem displacement and Effacement of CSF in the foramen magnum.
Figure 2: Axial T2W shows tonsillar descend with anterior brainstem displacement and Effacement of CSF in the foramen magnum. Figure 3: Sagittal T1W shows downward displacement of cerebellar tonsils approximately 16 mm relative to the McRae line. There is obliteration of the cisterna magna with mild anterior displacement of medulla oblongata.
Figure 3: Sagittal T1W shows downward displacement of cerebellar tonsils approximately 16 mm relative to the McRae line. There is obliteration of the cisterna magna with mild anterior displacement of medulla oblongata.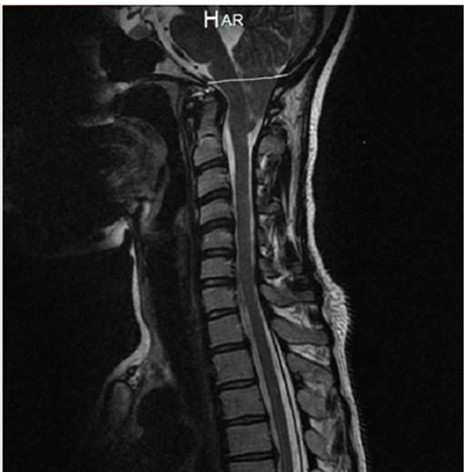 Figure 4: Sagittal T2W shows downward displacement of cerebellar tonsils approximately 16 mm relative to the McRae line. There is obliteration of the cisterna magna with mild anterior displacement of medulla oblongata.
Figure 4: Sagittal T2W shows downward displacement of cerebellar tonsils approximately 16 mm relative to the McRae line. There is obliteration of the cisterna magna with mild anterior displacement of medulla oblongata.Tonsillar herniation refers to the displacement of the cerebellar tonsils below the level of the foramen magnum, which is the opening at the base of the skull. This condition is measured by the extent of descent, and it is generally considered abnormal if the cerebellar tonsils descend more than 5 millimeters below the foramen magnum. Cerebral tonsillar herniation can be categorized into congenital and acquired forms [6,7]. Congenital tonsillar herniation (Chiari Malformation) Acquired tonsillar herniation can be associated with conditions that cause increased intracranial pressure. This may include situations such as brain tumors, hydrocephalus (excess cerebrospinal fluid), or certain types of traumatic brain injuries [6].
The McRae line is used as a reference for this measurement. It is obtained by drawing a line from the basion to the opisthio [7] The degree of tonsillar herniation is the perpendicular length from the McRae line to the tip of the displaced tonsil Main Document Tonsillar herniation, the brainstem is compressed against the clivus, thereby altering the vital life-sustaining functions of the pons and medulla, such as the respiratory and cardiac centers [8,3].
Complications arising from cerebellar tonsillar herniation, particularly in conditions like Chiari Malformation, can indeed have a profound impact on overall health. The cerebellar tonsils, when displaced below the foramen magnum, can compress vital structures in the brainstem, leading to a range of neurological and systemic effects. Some of the multifaceted complications associated with cerebellar tonsillar herniation include Neurological symptoms, respiratory disturbances, cardiac complications, swallowing and speech issues, hydrocephalus, syringomyelia, central nervous system dysfunction [4].
The compression of surrounding structures can lead to Brainstem Compression, hindrance of Cerebrospinal Fluid (CSF) Flow, development of Syringomyelia, impairment of blood flow, emergence of various neurological symptoms, and even psychological consequences. Chronic pain, stemming from the compression and altered neural signaling, can contribute to a significant psychological burden, affecting the individual's emotional well-being and daily life functionality [5].
The intricate interplay of these complications underscores the complex nature of tonsillar herniation and its far-reaching consequences.
Understanding the intricate relationship between the anatomical changes, clinical manifestations, and potential complications associated with tonsillar herniation is pivotal for healthcare professionals managing patients with this condition. A comprehensive approach that considers both the physical and psychological aspects of tonsillar herniation is essential for providing effective care and improving the overall quality of life for affected individuals [6,8,9].
Cerebellar tonsillar herniation, often associated with Chiari malformation, involves the downward displacement of the cerebellar tonsils below the foramen magnum. This condition can lead to significant complications due to the limited intracranial space within the rigid skull.
Management and treatment options would depend on the severity of symptoms and may include observation, medication, or surgical intervention (brainstem compression, obstruction of cerebrospinal fluid flow, syringomyelia, impaired blood flow, and various neurological and psychological symptoms) to relieve the compression and improve CSF flow. It's important for individuals with these findings to consult with a neurologist or neurosurgeon for a comprehensive evaluation and appropriate management plan. When addressing tonsillar herniation, the primary goal is often to relieve pressure on the brainstem and spinal cord. This can be achieved through various means, and the choice of treatment depends on the specific circumstances of each case.
The authors of the paper you are referring to have declared no conflicts of interest or financial gain.

