 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Mariam Konso* , Ikram Errabih, Salma Mechhor, Manal Cherkaoui Malki, Nadia Benzzoubeir, Hicham El Bacha
, Ikram Errabih, Salma Mechhor, Manal Cherkaoui Malki, Nadia Benzzoubeir, Hicham El Bacha
Department of Gastroentero-Hepatology and Proctology “Medicine B”, Ibn Sina Hospital, University Mohamed V, Rabat, Morocco.
Correspondence to: Mariam Konso, Department of Gastroentero-Hepatology and Proctology “Medicine B”, Ibn Sina Hospital, University Mohamed V, Rabat, Morocco.
Received date: April 04, 2024; Accepted date: May 05, 2024; Published date: May 12, 2024
Citation: Konso M, Errabih I, Mechhor S, et al. Caecal Adenocarcinoma Revealed by Ileo-Caecal Intussusception in Adult: A Case Report. J Med Res Surg. 2024;5(2):52-54. doi: 10.52916/jmrs244136
Copyright: ©2024 Konso M, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted
use, distribution and reproduction in any medium, provided the original author and source are credited.
Acute Intestinal Intussusception (AII) in Adult, unlike in children, is a rare event, most often occurring in the setting of a small bowel tumor of malignant origin. It accounts for 1 to 5% of intestinal obstruction etiologies in Adult. Invaginations have been classified into four categories according to their location: entero- enteric, colo-colic, ileo-colic and ileo-cecal. In Adult, an organic cause is found in 70-90% of cases, whereas in children, intestinal obstruction is most often idiopathic. Treatment is always surgical in Adult. We report a case of acute ileo-caecal intussusception revealing caecal adenocarcinoma in a 40-year-old woman.
Acute Intestinal Intussusception (AII), Organic cause, Adenocarcinoma, Invagination, Surgery.
Acute intestinal intussusception (AII) in adults, unlike in children, is a rare event, most often occurring in the setting of a small bowel tumor of malignant origin. It accounts for 1 to 5% of intestinal obstruction etiologies in adults [1]. In adults, an organic cause is found in 70-90% of cases, whereas in children, intestinal obstruction is most often idiopathic [2,3]. Intestinal Intussusception is defined as the telescoping of a proximal segment of the intestinal tract within the lumen of the adjacent distal segment. It was initially described in 1674 by Barbette from Amsterdam and presented by John Hunter in 1789 as “introssusception,” a rare form of bowel obstruction. Treatment for intussusception varies largely among children and adults due to the different etiologies. Treatment is always surgical in adults and frequently requires an urgent surgical solution. We report a case of acute ileo-caecal intussusception revealing caecal adenocarcinoma in a 40-year-old woman.
A 40-year-old woman with no previous history, presented to the emergency department after five days of intermittent diffuse abdominal pain originating in the right iliac fossa, associated with nausea, evolving in a context of altered general condition and apyrexia. Initially, pain was infrequent, but progressed to become more severe and regular, accompanied by rectal bleeding. Her Intestinal transit were altered, with a tendency to constipation. Vital signs were within normal limits. Clinical examination revealed distension in the right iliac fossa, with a tympanum on percussion, slightly tender, with no palpable mass. The rectal exam was bloodstained. The patient was apyretic. The rest of the clinical examination was normal, but there was a recent alteration in general status. Standard laboratory tests revealed anemia, with no signs of inflammation. An unprepared abdominal X-ray showed a level in the right iliac fossa, then an abdominopelvic CT scan with contrast showed a complex-appearing, elongated, sausage-shaped mass at the ileo-caecal level, with wall thickening at this level. The indication for surgery was clear. Laparoscopy revealed a viable invaginated loop, with no locoregional adenopathy. Surgical laparoscopic exploration a viable invaginated loop, with no locoregional adenopathy; any peritoneal carcinoma nodule or liver metastasis, but an intussusception of the caecum in the ileum with a 3 cm diameter mass on the caecal fundus. A hard, irregular caecal process (Figure 1). The patient underwent a right colectomy with ileocolic anastomosis by mechanical clamp.
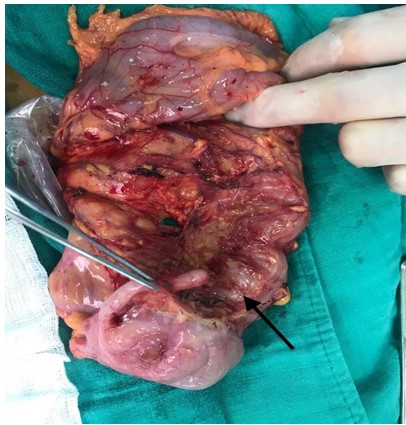 Figure 1: A tumour infiltrating the caecal wall discovered on opening the surgical specimen.
Figure 1: A tumour infiltrating the caecal wall discovered on opening the surgical specimen.Histopathological findings were consistent with a well-differentiated adenocarcinoma infiltrating the caecal wall. The post-operative course was straightforward, and after a few weeks, the patient was put on adjuvant chemotherapy, with good tolerance and control of the neoplastic pathology.
Intestinal intussusception accounts for 1 to 5% of the etiologies of intestinal obstructions in adults, and 0.003 to 0.02% of hospitalizations. An organic cause is found in 70 to 90% of cases, and idiopathic in 8 to 20%, whereas in children intestinal intussusception is primary in 90% of cases [2,3]. Intussusception is defined as the telescoping of a proximal segment of the intestinal tract within the lumen of the adjacent distal segment. It was initially described in 1674 by Barbette from Amsterdam and presented by John Hunter in 1789 as “introssusception,” a rare form of bowel obstruction [4]. Intussusception occurs most frequently between the fourth and seventh decades of life; the mean age for intussusception due to secondary malignancy is in the 6th decade, whereas for intussusception associated due to benign tumors usually occurs in the 4th decade. Incidence is similar between men and women [5]. They usually evolve subacutely or chronically. intussusceptions have been classified into four categories depending on their location: colo-colic, entero-enteric, ileo-colic and ileo-cecal [6]. Clinical symptoms are polymorphous and often misleading: acute occlusive picture, sub-occlusive picture of progressive onset lasting from a few days to a few weeks, non-specific abdominal syndromes (altered transit, diffuse abdominal pain, digestive bleeding), sometimes evolving over several months, with or without alteration of general condition [7,8]. In adults, the most frequent symptoms of intussusception are abdominal pain, nausea, and vomiting [9,10]. Physical exam rarely discloses an abdominal mass. An organic lesion is found at the point of weakness of the intussusception in 80% of adult cases. Malignant tumors represent the primary etiology of intussusception in adults, especially in the colon, whereas they are secondary to a benign lesion (especially in the small bowel) in 25% of cases, and 10% are idiopathic [11]. These organic lesions include stromal tumors, lipomas, polyps, adenopathies and digestive thickening, especially ileocaecal thickening. Melanoma, adenocarcinoma and metastases are found in around 15% of invaginations [12]. Ileo-colic intussusception in adults is rarely caused by adenocarcinoma, with only a few cases described in the recent literature. The most sensitive diagnostic tool is the CT scan, due to the pathognomonic target sign and sausage-shaped appearance [13,14]. Even if the CT scan diagnoses the intussusception, the etiology remains unidentified [14]. Sonography can also be useful in diagnosing intussusception by revealing in transverse view a target or doughnut sign but this can be limited by obesity or the presence of distended bowel loops [15].
The treatment for intussusception varies largely between children and adults due to the different etiologies. Treatment is always surgical in adults, and leaves no place for reduction by radiological control hyperpressure. Intussusception associated with bowel obstruction frequently requires an urgent surgical solution; if there are signs of intestinal ischemia, a resection of the affected segment should be performed [16] although if there is absence of vascular impairment, the surgeon should try to reduce the invagination, then performing the selective resection of the causal element in order to avoid a larger intestinal resection. It is necessary when the primary pathology requires resection, as in the case of malignant tumors. Intestinal excision according to carcinological rules is essential when an obviously malignant tumor is discovered. Our patient benefited from a right hemicolectomy performed according to carcinological rules. The prognosis depends on the duration of evolution, the extent of lesions and the nature of the cause [17].
In adults, intestinal intussusception is often secondary to an organic lesion: inflammation or tumor. It is a rare condition and should be considered in the differential diagnosis of bowel obstruction also in an adult patient. It is characterized by its clinical polymorphism. It is essentially a recurrent sub-occlusive phenomenon. Ultrasound and, above all, CT scans play an essential role in diagnosing intussusception and its cause. In the case of ileocolic intussusception due to a colonic process, carcinological resection is essential, as the majority of colonic tumors are malignant. Intraoperative manual reduction of intussusception in selected cases can reduce the length of resection, thereby decreasing the frequency of short bowel syndrome.
None.

