 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Cemal Aydın Gündoğmuş1* , Ruslan Asadov2, Tural Mammadov3, Efe Soydemir4, Mine Sorkun6, Feyyaz Baltacıoğlu5
, Ruslan Asadov2, Tural Mammadov3, Efe Soydemir4, Mine Sorkun6, Feyyaz Baltacıoğlu5
1Department of Radiology, Lokman Hekim University Akay Hospital, Ankara, Turkey.
2Department of Radiology, Azerbaijan Medical University, Baku, Azerbaijan.
3Department of Radiology, Istanbul Florance Nightingale Hospital, Istanbul, Turkey.
4Department of Neurosurgery, Marmara University, School of Medicine, Istanbul, Turkey.
5Department of Radiology, VKV Amerikan Hospital, Istanbul, Turkey.
6Department of Radiology, Koc University Hospital, Istanbul, Turkey.
Correspondence to: Cemal Aydın Gündoğmuş, Department of Radiology, Lokman Hekim University Akay Hospital, Ankara, Turkey.
Received date: July 25, 2024; Accepted date: August 13, 2024; Published date: August 20, 2024
Citation: Gündoğmuş CA, Asadov R, Mammadov T, et al. CT-Guided Core and Fine Needle Aspiration Transthoracic Lung Biopsies: Multivariate Analysis of Risk Factors Associated with Pneumothorax and Effect of Dwell Time in Core Biopsies. J Med Res Surg. 2024;5(4):88-94. doi: 10.52916/jmrs244143
Copyright: ©2024 Gündoğmuş CA, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted
use, distribution and reproduction in any medium, provided the original author and source are credited.
Purpose: To compare CT-guided core and fine-needle aspiration TTLBs in terms of complication rates, diagnostic adequacy, and dwell time and to investigate the independent risk factors associated with pneumothorax.
Material and Methods: 247 consecutive biopsies (125 core and 122 FNA) were evaluated retrospectively. 17-18 G co-axial system was used in the core, and 19-22 G co-axial system was used in FNA biopsies. Lesions less than 10 mm were excluded since all were performed with FNA. The dwell time of each biopsy was noted.
Results: The median age of the study group was 63 (183 males, 64 females). There was no significant difference between the core and FNA biopsy groups regarding age, gender, other parenchymal diseases, lesion localization, and traversed lung. Median dwell time was significantly shorter in the core biopsy. PX rate was 19.4%. Nineteen patients (7.7%) had PX requiring treatment. PX was not found to be related to the biopsy needle (core or FNA), even though its rate was significantly higher in the FNA. 5.5 minutes was the threshold dwell time for the occurrence of PX in the core biopsies. Dwell time more than this increased the risk by 4.9 times.
Conclusion: Diagnostic adequacy and major complication rates of core biopsies are similar to FNAB. Although PX rates were higher in FNA biopsies, the biopsy type did not affect the risk. The threshold time for the safe procedure in core biopsies has been 5.5 minutes.
Transthoracic lung biopsy, Pneumothorax, Multivariate analysis, CT scan, Pneumothorax.
CT-guided Transthoracic Lung Biopsies (TTLB) are frequently performed in interventional radiology clinics. With the widespread use of lung cancer screening, it is expected that there will be an increase in the number of detected lesions and biopsies to be performed [1]. CT-guided TTLB can be performed as a core and Fine-Needle Aspiration (FNA) biopsy. Most of the time, access to the lesion is provided with the co-axial technique in both methods [2]. Although the procedure is widely accepted, the reported complication rate varies greatly. Pneumothorax is the most common complication of transthoracic lung biopsy in the literature, with rates ranging between 10-40% in different studies [3]. Other complications of TTLB are hemoptysis, parenchymal hemorrhage, hemothorax, air embolism, infection, and seeding metastasis [4]. Generally acknowledged common risk factors of pneumothorax are emphysema, small lesion size, no contact between the lesion and pleura, multiple pleural punctures, prone or lateral decubitus body position, larger needle gauge, higher patient age, and longer traversed lung [3,5]. Since most patients have more than one risk factor, a multiple logistic regression analysis is mandatory to assess which independent variables contribute to pneumothorax, and studies including a multivariate analysis are limited. There is still very limited data on how dwell time affects pneumothorax risk, and there is one paper showing dwell time as an independent risk factor and one, not recently [6-8].
This study aims to compare CT-Guided core and fine-needle aspiration transthoracic lung biopsies in terms of complication rates, diagnostic adequacy, and dwell time and to investigate the independent risk factors associated with pneumothorax.
Ethical approval for this study was obtained from the Institutional Review Board (Document number: 02.09.2022.1187). Detailed informed consent was obtained from each patient. A total of 312 patients who underwent CT-guided transthoracic lung biopsy in the interventional radiology department of a tertiary hospital between March 2013 and April 2019 were included in this retrospective study. Forty patients with incomplete procedural images or for whom the dwell time could not be calculated, 12 patients with lesions invading the chest wall, ten patients with lesions with any diameter lower than 10 mm, and three patients with a mass located in the mediastinum were excluded.
The study population was 247 (125 core and 122 FNA biopsy patients). Since all the patients eligible for the study population were included, random selection was not performed.
Core and FNA biopsies are performed with the co-axial technique in our center. As a standard, 17 G co-axial and 18 G core (Bard Monopty Disposable Core Biopsy Device; Bard, Tempe, Ariz needles are used in core biopsies, and 19 G coaxial and 20-22 G aspiration needles are used in FNA biopsies.
Procedures were performed under CT guidance on a 64-section multidetector CT (Somatom Sensation; Siemens, Erlangen, Germany). All the procedures were applied by three operators under local anesthesia. Operators have 25, 9, and 5 years of interventional radiology experience. While a cytopathologist accompanied all fine needle biopsies, on-site cytology was never used in core biopsies. Standard 3 samples are taken in core biopsies, and a maximum of 5 samples are taken in FNA. As for the puncture planning, we avoid interlobar fissures to reduce the number of pleural punctures. We try to traverse the least amount of aerated lung without puncturing bullae or pneumatocele. All biopsies were technically successful. None of the procedures were stopped before retrieving a biopsy sample because of pneumothorax. Transfissural pass was a must in 6 patients. FNA biopsy is preferred for lesions smaller than 10 mm, in our institute. Therefore, these patients were excluded from the study. There are no criteria affecting the selection of FNA or core biopsy other than size. While FNA biopsy was used more frequently in previous years, core biopsy has been used more frequently in recent years. Core biopsy was chosen more often in larger lesions, naturally. Each practitioner is sufficiently experienced in both biopsy methods. Any breath-holding instructions are not used. The ‘’Biopsy side down’’ position was not used after biopsies. Oxygen through a nasal cannula was administered for all patients with minor pneumothorax. A CT scan is done immediately after the procedure for the pneumothorax control, and control chest radiographs are done at the 2nd and 6th hours post-intervention. If a pneumothorax greater than 20% or reaching the apex is seen on control CT images or patient SpO2 drops below 90%, a 6 F drainage catheter was inserted into the hemithorax with the Seldinger method, and aspiration was performed with the help of a stopcock. Evaluation of Procedure Images and Data Collection A radiologist retrospectively evaluated the images of the procedure and recorded the lesion localization, dimensions in two axes, the relationship of the lesion with the pleura and the fissures, the distance of lung tissue passed with the needle to reach the lesion, the duration and the complications of the procedure, and the patient's other lung disease, if any. Also, chest radiographs at the 2nd and 6th hours were also evaluated for pneumothorax.
The dwell time was recorded in minutes by calculating the difference between the time of the last CT images taken for complication control and the time of the first image when the coaxial needle passed the pleura. Traversed lung parenchyma to reach the lesion was measured on the needle trace between the lesion and the pleura and recorded in millimeters. Pneumothorax requiring treatment was determined as the need for a chest tube and hospitalization. Pneumothorax that was aspirated with a drainage catheter immediately after the procedure and did not require a chest tube was not classified as pneumothorax requiring treatment. The diagnostic adequacy of the biopsies and the patients’ demographic data were recorded blindly to the biopsy data from the hospital automation system.
Statistical Analysis Descriptive features were examined with n and % values in categorical data and median, minimum-maximum values in continuous data in the study. The Chi-square test and Fisher's exact test were used to compare categorical data. The distributions of continuous data were analyzed with the Kolmogorov-Smirnov test. The Mann-Whitney U test was used to compare continuous data. Receiver Operating Characteristic (ROC) curve was used to determine the threshold time value in the development of pneumothorax. Logistic regression analysis was used to calculate the effects of complication risk factors and confounders. Transfissural pass was not included in the logistic regression analysis because of the low number of observations (<15).The alpha error level was accepted as 5% for statistical significance. Analysis was done with IBM SPSS v.20.
The median age of 247 patients was 63 (14-88). One hundred and eighty-three (74%) patients were male, and 64 (26%) were female. There was no significant difference between the core and FNA biopsy groups regarding age, gender, presence of other parenchymal diseases, lesion localization, and traversed lung (Tables 1 and 2). The most common parenchymal disease was emphysema (n=66, 19.2%). Mass as an indication for biopsy was significantly higher in the core biopsy group [98 (78.4%), 43 (35.2%), respectively, p<0.001]. And also, both median short and long-axis diameters of the lesion are significantly higher in the core biopsy group (Table 2). Median dwell time is significantly shorter in the core biopsy group [4 (2-21), 14 (7- 40), respectively, p<0.001] (Table 1).
Table 1: Comparison of age, lesion, and biopsy metrics between groups.|
|
Core Biopsy (n=125) Median (Min-Max) |
FNA Biopsy (n=122) Median (Min-Max) |
p-value |
|
Age |
62 (14-88) |
64 (26-86) |
0.514 |
|
Long axis diameter (mm) |
52 (20-141) |
27 (10-85) |
<0.001 |
|
Short axis diameter (mm) |
38 (17-101) |
20 (10-74) |
<0.001 |
|
Dwell Time (min) |
4 (2-21) |
14 (7-40) |
<0.001 |
|
Traversed lung (mm) |
21 (5-70) |
23 (6-73) |
0.239 |
|
|
Core Biopsy |
FNA Biopsy |
p-value |
|
|
n (%) |
n (%) |
|||
|
Gender |
Male |
99 (79,2) |
84 (68,9) |
0,063a |
|
Female |
26 (20,8) |
38 (31,1) |
||
|
Perifissural |
35 (28.0) |
24 (19,7) |
0,124a |
|
|
Subpleural |
51 (40.8) |
64 (52,5) |
0,066a |
|
|
Localization |
Lower lobe |
60 (48,0) |
53 (43,4) |
0,472a |
|
Upper/Middle Lobe |
65 (52,0) |
69 (56,6) |
||
|
Other Lung Diseases or CT Findings |
|
44 (35.2) |
44 (36.1) |
0,887a |
|
Type |
Emphysema |
31 (70,5) |
35 (79,5) |
0,056b |
|
Interstitial |
1 (2,3) |
3 (6,8) |
||
|
Pleural Effusion |
5 (11,4) |
2 (4,5) |
||
|
Mosaic attenuation |
1 (2,3) |
3 (6,8) |
||
|
Sequela |
2 (4,5) |
1 (2,3) |
||
|
Lymphangitic carcinomatosis |
4 (9,1) |
0 (,0) |
||
|
Indication for biopsy |
Mass |
98 (78,4) |
43 (35,2) |
<0,001,b |
|
Solitary pulmonary nodule |
10 (8,0) |
39 (32,0) |
||
|
Metastasis (patients with diagnosed malignancy) |
5 (4,0) |
32 (26,2) |
||
|
Others |
12 (1,0) |
8 (0,6) |
||
|
Pneumothorax |
- |
107 (85,6) |
92 (75,4) |
0,043a |
|
+ |
18 (14,4) |
30 (24,6) |
||
|
PX requiring treatment |
- |
118 (94,4) |
110 (90,2) |
0,212a |
|
+ |
7 (5,6) |
12 (9,8) |
||
|
Hemoptysis |
- |
115 (92.0) |
113 (92.6) |
0.854a |
|
+ |
10 (8.0) |
9 (7.4) |
||
|
Parenchymal Hemorrhage |
- |
111 (88,8) |
99 (81,1) |
0,092a |
|
+ |
14 (11,2) |
23 (18,9) |
||
|
Sample Adequacy |
|
108 (86.4) |
110 (90.1) |
0.358a |
|
a: Chi-Square Test; b: Fisher’s Exact Test |
||||
The overall complication rate of the study group is 36.4% (n=90). Pneumothorax is the most common complication, with a rate of 19.4% (n=48). Nineteen patients (7.7%) had pneumothorax requiring treatment. Chest tube placement was needed for 39.6% of all pneumothoraxes. Hemoptysis was seen in 19 (7.7%) patients, and parenchymal hemorrhage was seen in 37 (15%) patients. The biopsy specimen was adequate for diagnosis in 218 (88.2%) patients. Hemothorax, infection, air embolism, and seeding were not observed.
The pneumothorax rate was 24.6% (n=30) in the FNAB group and 14.4% (n=18) in the core biopsy group, and the difference was statistically significant (p=0.043). There was no significant difference between core and FNA biopsy groups in the rate of pneumothorax requiring treatment [7 (5.6%), 12 (9.8), respectively, p=0.212]. There was no significant difference in hemoptysis and parenchymal hemorrhage rates between the two groups (Table 2).
A Receiver Operating Characteristic (ROC) curve was drawn to determine the threshold time value for the occurrence of pneumothorax in the core biopsy group (Figure 1). According to the ROC curve, 5.5 minutes can be accepted as the threshold value for pneumothorax occurrence. The area under the curve (AUC) for this value was 0.701 (0.552-0.850) and was statistically significant (p=0.006). Specificity, sensitivity, positive and negative predictive values were 72.2%, 69.2%, 28.3%, and 93.7%, respectively. A statistically significant cut-off value could not be determined as a threshold for the occurrence of pneumothorax in the FNA biopsy group.
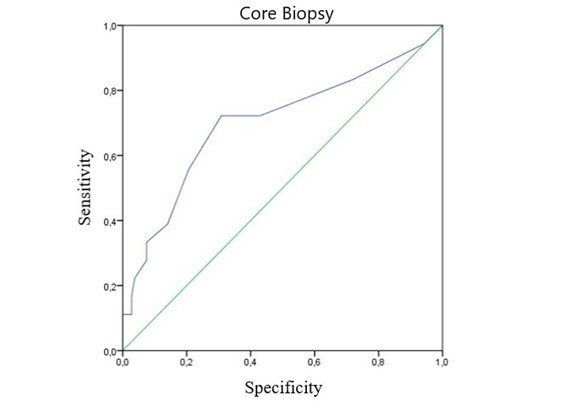 Figure 1: Receiver Operating Curve of dwell time in core biopsies.
Figure 1: Receiver Operating Curve of dwell time in core biopsies.In the logistic regression analysis performed to investigate the independent risk factors associated with pneumothorax in all biopsies, each one-unit increase in a patient’s age reduces the possibility of pneumothorax by 2.2% (p=0.001). While lesion size and its proximity to the fissure or pleura do not affect the pneumothorax risk, the presence of other parenchymal diseases increases this risk 2.9 times (p=0.002). Each millimeter increase in the traversed lung tissue increases the risk by 3% (p=0.016). Dwell time does not increase the pneumothorax risk in the analysis of all biopsies (p=0.330). The biopsy method (core or FNA biopsy) does not affect the risk of pneumothorax (p=0.741) (Table 3).
Table 3: Logistic regression analysis of pneumothorax risk factors in all patients.|
|
OR |
%95 Confidence İnterval |
p-value |
|
|
Lower |
Upper |
|||
|
Age |
0,972 |
0,955 |
0,989 |
0,001 |
|
Long-axis diameter |
0,992 |
0,955 |
1,029 |
0,656 |
|
Short-axis diameter |
0,978 |
0,931 |
1,027 |
0,372 |
|
Perifissural lesion |
1,181 |
0,523 |
2,669 |
0,689 |
|
Subpleural lesion |
0,533 |
0,250 |
1,140 |
0,105 |
|
Parenchymal disease |
2,981 |
1,504 |
5,908 |
0,002 |
|
Dwell Time |
1,034 |
0,967 |
1,105 |
0,330 |
|
Traversed lung (mm) |
1,031 |
1,006 |
1,057 |
0,016 |
|
Biopsy (Core or FNA) |
0,724 |
0,265 |
1,975 |
0,528 |
|
Nagelkerke R Square: 0,513 |
||||
According to the logistic regression analysis performed to investigate the independent risk factors associated with pneumothorax in the core biopsy group, each millimeter increase in the traversed lung tissue increases the pneumothorax risk by 5% (p=0.018). While the patient’s age, parenchymal disease, lesion size, and proximity to the fissure or pleura do not affect the pneumothorax risk, a dwell time of more than 5.5 minutes increases the pneumothorax risk 4.9 times (p=0.007) (Table 4).
Considering the diagnostic adequacy, biopsy material was sufficient for the definite diagnosis in 86.4% (n=108) in the core biopsy group and 90.1% (n=110) in the FNAB group (p=0.358).
Table 4: : Logistic Regression analysis of pneumothorax risk factors in core biopsy group.|
|
OR |
%95 Interval |
p-value |
|
|
Lower |
Upper |
|||
|
Age |
0,977 |
0,950 |
1,004 |
0,097 |
|
Long axis diameter |
1,005 |
0,956 |
1,056 |
0,853 |
|
Short-diameter |
0,957 |
0,896 |
1,022 |
0,188 |
|
Perifissural lesion |
1,844 |
0,555 |
6,123 |
0,318 |
|
Subpleural lesion |
0,445 |
0,132 |
1,505 |
0,193 |
|
Disease |
1,034 |
0,314 |
3,406 |
0,956 |
|
Traversed (mm) |
1,052 |
1,009 |
1,098 |
0,018 |
|
Dwell (>5.5 min.) |
4,886 |
1,551 |
15,393 |
0,007 |
|
Nagelkerke R Square: 0,670 |
||||
This study shows the threshold time value for the occurrence of pneumothorax in the core biopsy group according to the ROC curve was 5.5 minutes with a 93.7% negative predictive value, meaning that if the co-axial needle of the core biopsy dwell time is less than 5.5 minutes, the patient will most likely not experience pneumothorax with high sensitivity. Complication rates increase with the time of the procedure as a general acceptance. However, we set a specific cut-off dwell time value for transthoracic core lung biopsy regarding the pneumothorax risk. The literature data on this is very limited. Ko et al. investigated the effect of dwell time in a study with 160 FNA biopsies and 39% pneumothorax rate and stated that longer dwell time did not correlate with pneumothorax (mean, 29 minutes; range, 12-66 minutes, p:0.81) [6]. We added this specific cut-off dwell time value to the logistic regression analysis group as an independent risk factor for pneumothorax.
We found that a dwell time of more than 5.5 minutes increases the pneumothorax risk by 4.9 times. One recent study by Zhou et al. showed that longer dwell time is related to a higher risk of pneumothorax in 1100 consecutive patients [OR:1.963 (1.736 2.219), p=4.938 × 10-27] [7]. On the other hand, another recent research on 1110 patients by Li et al. stated that, although dwell time was significantly correlated with pneumothorax on univariate analysis, it was not confirmed to be an independent predictor on multivariate analysis [OR:1.001 (0.999–1.003), p=0.217] [8]. Considering all the biopsies in our study, dwell time was not found to be an independent risk factor of pneumothorax also.
We compared CT-guided transthoracic core and FNA lung biopsies regarding dwell time, complications, and diagnostic adequacy. There was no significant difference between core and FNA biopsy groups in terms of age, gender, presence of other parenchymal diseases, lesion localization, and traversed lung. The lesions' short and long-axis diameters were higher in the core biopsy group. Dwell time and pneumothorax rates are higher in FNA biopsy. The main reason for the longer dwell time is, FNA biopsies are accompanied by on-site cytology. Longer dwell time and smaller lesion size are two main factors of higher pneumothorax rates of FNA biopsy. Total pneumothorax and pneumothorax requiring treatment rates are 19.4% and 7.7%, respectively. Relevant literature data is somewhat incoherent. Pneumothorax is reported in the literature at rates varying between 7 and 53.5% [9,10]. Pneumothorax requiring treatment rates are reported between 0-18.6% [11,12].
There are many confounders for pneumothorax risk, such as patients’ age, lesion size and localization, presence of parenchymal disease, longer traversed lung, number of crossed pleural surfaces, and fissures, biopsy method, and needle gauge [13]. Therefore, a logistic regression analysis is imperative to assess which independent variables contribute to the pneumothorax and to what extent. Even though the pneumothorax rate of the FNA biopsy is significantly higher than the core biopsy, logistic regression analysis reveals that the biopsy method does not affect the risk of pneumothorax.
This study is the only one in the literature assessing the biopsy method in multivariate analysis as an independent risk factor. The pneumothorax rate was 14.4% for the core biopsy and 24.6% for the FNA biopsy. Some papers report a higher complication rate for core biopsy than FNA [14,15]; other studies do not [16]. A systematic review by Yao et al. comparing core and FNA biopsies concluded that there is no difference in complication rates between the two techniques [17]. A meta-analysis by Heerink et al. showed that pneumothorax rates of FNA biopsy were significantly lower than that of core biopsy [18.8% (14.6-23.9%), 25.3% (22.2-28.6%), respectively, p=0.027] [3]. Two prospective studies showed no difference between FNA and core biopsy in pneumothorax [16,18]. These controversial results are probably due to many other confounders stated before. Also, there is no consensus on the needle Gauges for TTLB, which may be another reason for these results. We perform core biopsies with 17-18 G and FNA biopsies with 19-20/22 G co-axial systems in our center. Priola et al. stated in their study on 73 patients that 14G tru-cut needles have a higher complication rate, while 18G needles do not increase the complication rate compared to FNAB [19]. We also found that the biopsy technique does not increase pneumothorax risk with 17-18 G core and 19-20 G FNA biopsy needles.
Pneumothorax requiring treatment rates between core and FNAB were not significantly different in the meta-analysis by Heerink et al. [3]. Our study revealed similar results. 5.6% of the core biopsy group and 9.8% of the FNA biopsy group required chest tube placement with a p-value of 0.212. There is a clear tendency for higher chest tube requirements in the FNAB group. Since only 19 patients out of 247 had pneumothorax requiring treatment, there may be an α-type error in the statistic. Parenchymal hemorrhage and hemoptysis rates were not different between core and FNA biopsy groups.
Besides the biopsy technique, lesion diameters and localization (perifissural, subpleural) do not affect the risk. We excluded 10 FNA biopsy patients to avoid selection bias since there is no core biopsy patient with a lesion smaller than 10 mm. Seven out of these ten patients had pneumothorax, and 4 had chest tubes. Consequently, the effect of lesion short-axis diameter on the pneumothorax risk might be underestimated in the logistic regression as an outlier handling bias. However, Geraghty et al. did a retrospective review of 846 consecutive CT-guided TTLB procedures, with 226 (26.7%) pneumothorax. None of the analyzes performed with cut-off values of 1 and 2 cm showed a significant difference in pneumothorax rates between the smaller and larger lesion groups [20]. Also, in a multivariate logistic regression analysis of pneumothorax risk factors in the article of Zhao et al., the short-axis diameter of the lesion was not found to be an independent risk factor [OR:0.992 (0.981- 1.004), p=0.194] [5]. Again Heerink et al. proved that mean lesion size does not affect the major complication risk in a metaanalysis [12 studies, 2357 procedures, OR:0.97 (0.93-1.00), p=0.073] (3).
The patient’s age is inversely related to pneumothorax risk in our series. The inverse relation between a patient’s age and pneumothorax risk might seem contrary to expectation. As a reminder, each unit’s decrease in patient age increased the risk of pneumothorax by 2.2%. The association between age and pneumothorax is not a well-established subject against common sense. According to a meta-analysis including 32 studies and 8133 procedures, the mean patient age does not significantly affect the pneumothorax risk [OR:1.09 (0.81-3.23), p=0.171] [3]. Logistic regression of a study by Zhao et al. showed that the patient’s age was not an independent risk factor even though there was a significant difference between pneumothorax and non-pneumothorax groups in the univariate analysis (60 ± 10.2, 58.8 ± 10.7 respectively, p=0.008) [5]. However, the inverse relationship in this study is an abnormal finding overall and needs to test in larger series.
As for what increases the risk of pneumothorax, the presence of other lung diseases and longer traversed lung parenchyma for all biopsies. These are well-established risk factors for complications of transthoracic lung biopsies. We included other parenchymal diseases such as interstitial involvements, lymphangitic carcinomatosis, mosaic attenuation, and pleural effusions. Clinical data were not considered, so only thorax CT findings were noted. Even emphysema was 75% of the other lung diseases; we did not include spirometry measures or Global Initiative for Chronic Obstructive Lung Disease (GOLD) staging of the patients. The presence of an additional lung disease multiplies the pneumothorax risk by 3 times according to the logistic regression analysis of the entire biopsies. Cox et al. found that the presence of emphysema increased the rate of pneumothorax; also, patients with emphysema were three times more likely to require a chest tube placement [21]. Each millimeter increase in the traversed lung tissue increases the pneumothorax risk by 3% in this study. We confirm the published findings of many publications emphasizing that the depth of the lesion [22-24] and passing through aerated lung tissue [25] are increasing pneumothorax risk.
88.3% of the biopsies were diagnostic and diagnostic adequacy of core and FNA biopsies does not show a significant difference. Core biopsy sample adequacy may be slightly lower than the literature data, as none were accompanied by on-site cytology. In the study of Yeow et al., they applied transthoracic lung core biopsy and performed three samples per procedure; diagnostic efficiency was reported to be 95% in 631 biopsies [26].
Retrospective design is the main limitation of the study and leads to a lag in the real dwell time since there has to be a span between the time the needle retracted and the last control CT images. However, this span was applied to all the patients, so it probably does not affect the statistics. One should understand that the 5.5 minutes cut-off value for core biopsies that increase pneumothorax risk is lower than we calculated. We did not investigate the effect of operators’ experience on the complication risk since even the less experienced operator has five years of TTLB experience. As a natural outcome, the lesions in the core biopsy group were larger in diameter.
In conclusion, both FNAB and core biopsies can be performed safely in CT-guided transthoracic lung biopsies. Diagnostic adequacy and major complication rates of core biopsies are similar to FNAB. Short procedure time is an advantage of core biopsies. Although pneumothorax rates were higher in FNA biopsies, it was found that the biopsy type did not affect the development of pneumothorax in multivariate analysis. The threshold time for the safe procedure in CT-guided transthoracic core biopsies has been 5.5 minutes.
Author declares there is no conflicts of interest.
No source funding for this article, author's own expenses.

