 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Talha Arif1* , Humara Gull2
, Humara Gull2
1 4th Year Undergraduate Student, Rice University 6100 Main Street Houston, TX 77030, United States
2 Primary Care Physician, iMD Healthcare and Imaging 19411 McKay Dr. # 150 Humble, TX 77338, United States
Correspondence to: Talha Arif, 4th Year Undergraduate Student, Rice University 6100 Main Street Houston, TX 77030, United States.
Received date: January 21, 2022; Accepted date: January 28, 2022; Published date: February 06, 2022
Citation: Arif T, Gull H (2022) Anticoagulation in the Treatment of Pulsatile Tinnitus Caused by Internal Jugular Vein Stenosis: A Rare Case Report. J Med Res Surg
3(1): pp. 10-12. doi: 10.52916/jmrs224068
Copyright: ©2022 Arif T, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted
use, distribution and reproduction in any medium, provided the original author and source are credited.
Background: Anticoagulation is considered as a first line treatment of pulsatile tinnitus caused by internal jugular vein thrombosis. We present a case of non-thrombotic internal jugular vein occlusion which responded to Apixaban (Eliquis) therapy.
Case Presentation: A 54-year-old female with no significant past medical history presented with debilitating pulsatile tinnitus for two months. Her symptoms included inability to sleep, lower appetite, and intense pressure and throbbing in the face and ears. She described it as a ‘whooshing sound’ exacerbated in the supine position. She admitted to occasional episodes of neck throbbing and forceful heart beat over the years and had undergone multiple workups including Echocardiograms and Holter monitoring, with no apparent abnormalities.
The recent workup, including coagulation studies, Computed Tomography (CT) scans and Magnetic Resonance Imaging (MRI) of the head and neck, yielded negative findings. However, a CT angiogram revealed an isolated non-thrombotic occlusion of the most proximal aspect of the left Internal Jugular Vein (IJV), with extensive occipital and sub occipital collateral flow. She had been taking antihypertensive and diuretic medications without much effect. She was then prescribed anticoagulation therapy initially with IV enoxaparin (30 milligrams for two weeks) and then oral Apixaban (5 milligrams b.i.d.).
Eliquis 5 milligrams bid was continued for 8 months and tapered down to 2.5 milligrams bid for 4 months to completely off in 12 months. Her symptoms improved after eight weeks and were completely gone within a year. Repeat MR angiography showed improved flow in the jugular venous system.
Conclusions: A trial of anticoagulation is warranted and can be beneficial in patients with non-thrombotic internal jugular vein occlusion causing pulsatile tinnitus refractory to other treatments.
Pulsatile tinnitus, Anticoagulation, Internal jugular vein occlusion
Tinnitus refers to a ringing sound in the ears and can be pulsatile or nonpulsatile [1]. Pulsatile tinnitus is a specific form of tinnitus and commonly manifests as a “whooshing” sound synchronous with heartbeat, with its effects ranging from throbbing in ears to hearing loss and vertigo. Pulsatile tinnitus from a vascular etiology can be caused by blood flow turbulence if obstruction of an arterial or venous vessel has occurred [2]. Cases of pulsatile tinnitus associated with cerebral venous thrombosis (sagittal sinus) have also been published in the literature [3]. Non thrombotic IJV occlusion by itself is an uncommon condition. Most common causes of IJV occlusion are attributed to thrombosis secondary to IJV cannulation, trauma, surgery or irradiation [4]. External compression by an elongated styloid process has also been reported [5]. The clinical presentation of this condition is highly variable, ranging from insidious to symptomatic, such as headaches, dizziness, pulsatile tinnitus, visual impairment, sleep disturbance, and neck discomfort or pain. Standard diagnostic criteria are not available, and current diagnosis largely depends on a combination of imaging modalities [6]. Hence, investigating the IJV, whether occlusion or stenosis, is critical to minimize misdiagnoses and better understand its etiology.
Venous outflow mainly occurs through the internal jugular system in a supine position, making it more challenging to be diagnosed with noninvasive diagnostic modalities. In addition, gravity affects cerebral venous system output. Studies indicate jugular vein collapse in an upright position, with cerebral venous drainage occurring through the vertebral venous system instead [7]. In this case, we report left jugular vein occlusion presenting as pulsatile tinnitus in the supine position. Fewer case reports of IJV stenosis associated with pulsatile tinnitus and other symptoms have been reported [8,9].
A 54-year-old female with no significant past medical history was seen by her primary care physician for pulsatile tinnitus for two months. Her symptoms included inability to sleep, decreased appetite, and intense pressure and throbbing in the face and ears in supine position. She admitted to occasional episodes of forceful heartbeats for years and had undergone multiple workups including Echocardiogram and Holter monitoring, with no apparent abnormalities and no history of contraceptive medications in the past. The entire workup, including labs for coagulopathy, CT scans of the head, neck, and chest, and MRIs, yielded negative findings. She was seen by multiple specialists including a cardiologist, neurologist, Ears, Nose and Throat (ENT) surgeon, ophthalmologist, vascular surgeon, and hematologist oncologist. She was finally referred to a neurovascular interventionist for further investigation to rule out neurovascular abnormalities.
He performed a cerebral angiogram which showed non thrombotic occlusion of the left IJV at the most proximal aspect with prominent occipital and sub occipital venous systems. The venous collaterals were well developed, suggesting a potential congenital or long-standing IJV abnormality. She was offered intravenous angioplasty and stenting versus conservative management. She opted for conservative management with anticoagulation, thiazide diuretics and nitrates. Thiazide diuretics and nitrates were discontinued after two weeks while anticoagulation was continued for a year. Her symptoms improved with anticoagulation and were completely gone within a year. A repeat MR angiogram showed improved flow in the jugular venous system.
Internal jugular venous outflow obstruction has been studied extensively. Multiple factors including intracranial and extracranial pathology have been cited [6]. However, due to limitations in the standard diagnostic tools, the IJV stenosis can be misdiagnosed resulting in prolongation of the debilitating symptoms. Venous outflow mainly occurs through the internal jugular system in a supine position. In addition, gravity affects cerebral venous system output. Studies indicate jugular vein collapse in an upright position, with cerebral venous drainage occurring through the vertebral venous system instead [7]. In this case report, pulsatile tinnitus presenting more in supine position due to IJV occlusion explains this patient’s symptoms. Similar case reports of IJV occlusion associated with pulsatile tinnitus have been reported [8,9].
This observed venous flow is congruent with prior studies examining increased collateral drainage in response to the reduction of IJV flow in Multiple Sclerosis cases as well [10]. Pulsatile tinnitus can likely be sourced to this increased collateral flow. Since IJV etiology is commonly overlooked, this report is important in beginning to address such misdiagnosed cases.
Furthermore, anticoagulants such as sodium enoxaparin may hold therapeutic value in addressing tinnitus, based on previous research [3,11]. This patient was offered intravenous angioplasty with stents versus conservative management with elevation of the head when sleeping, nitrates, diuretics, and oral anticoagulants. Nitrates and diuretics have been used to decrease venous congestion [12,13].
As this patient was seen by multiple specialists, there were differing opinions on how to manage the treatment, given the absence of apparent thrombosis in the IJV. However, the consensus was obtained, in cooperation with the patient, to give a trial of anticoagulation. Given the high risk of bleeding with pharmacokinetic Eliquis, a factor Xa inhibitor (Apixaban) [14,15], the patient was initially started on low molecular weight heparin Enoxaparin (Lovenox) 30 milligrams subcutaneously for two weeks, then switched to oral Eliquis (5 milligrams b.i.d.). Diuretics and nitrates were stopped after 2 weeks. Eliquis 5 milligrams bid was continued for 8 months and tapered down to 2.5 milligrams b.i.d. for 4 months to completely off in 12 months. Her symptoms qualitatively improved over a period of eight weeks and were completely gone in 12 months. A repeat MR angiogram showed improved flow in the jugular venous system.
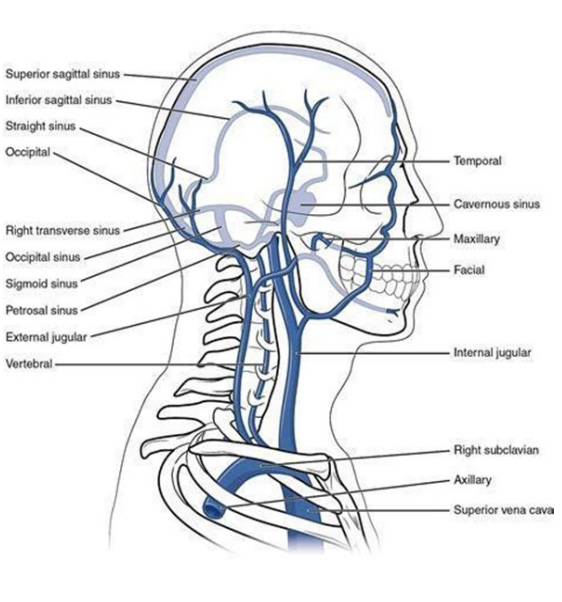
All investigations in this case did not reveal an apparent cause of IJV occlusion. The most likely explanation could be a gradual occlusion of the IJV by micro-clots in an already narrow or stenosed IJV by birth. The role of anticoagulants in this case could have been to prevent any further clotting and help build up collateral venous flow, thus reducing the symptoms of obstruction. Current guidelines exist for treatment for deep vein thrombosis, including the use of Enoxaparin and Eliquis [16]. However, further controlled studies are needed to evaluate the role of anticoagulants in this regard. Although their role may not be well documented, anticoagulants hold a promising role in IJV stenosis without apparent etiology. Their addition to the armamentarium for the treatment of pulsatile tinnitus would prove to be beneficial against infection or any obstructive etiology (Figure 1).
The authors have no financial disclosures.
No funding or grant support.

