 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Manikumar CJ1* , Pardhasaradhi M2
, Pardhasaradhi M2
1Department of Orthopaedics, Government Medical College Vizianagaram, Andhra Pradesh, India.
2Department of Orthopaedics, Government Medical College Srikakulam, Andhra Pradesh, India.
Correspondence to: Manikumar CJ, Department of Orthopaedics, Government Medical College Vizianagaram, Andhra Pradesh, India.
Received date: December 28, 2023; Accepted date: January 15, 2024; Published date: January 22, 2024
Citation: CJ Manikumar, M Pardhasaradhi. Antibiotic Impregnated Cement Coated Intramedullary Nailing in the Management of Infected Fractures and Chronic Osteomyelitis of Long Bones. J Med Res Surg. 2023;5(1):1-5. doi: 10.52916/jmrs244126
Copyright: ©2023 CJ Manikumar, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted
use, distribution and reproduction in any medium, provided the original author and source are credited.
Background: In the era of modern transportation there is an increased incidence of compound fractures especially of long bones. As the skin barrier is broken, the bacteria from dirt, other contaminants can colonize at the wound site and thus can cause infection. Healing at the fracture site and that of soft tissues can be severely compromised by infection. So, treating the infection first followed by definitive fixation of fracture will nearly take 4-6 weeks. The antibiotic nailing technique can thus achieve both the targets in a short time. Local delivery of drug controls the infection and the fixation achieves stability. This even reduces the side effects due to over use of systemic and oral antibiotics.
Osteomyelitis is also very common which can be hematogenous or post traumatic. This can weaken the bone and can cause fractures with trivial trauma. Discharging sinuses may also be accompanying. So even in this scenario long term use of antibiotics systemically may be required causing side effects. Antibiotic nailing can be very useful in this scenario.
Methods: This is a prospective observational study. 20 patients above age of 20 years who were admitted or on follow up during the period of 2 years were considered for study. The patients with infected fractures with or without implant in situ and patients with chronic osteomyelitis with discharging sinuses were included.
ASAMI Criteria: The final outcome is graded based on ASAMI criteria proposed by Paley et al. This was usually developed for determining the outcome after treatment of nonunion with Ilizarov ring fixator. It was applied in our study with some modification.
Results: The average duration for achieving bony union was around 5 months (20 weeks). Minimum duration for bony union was around 4 months (16 weeks). Maximum duration for bony union was around 7 months (28 weeks) Average duration for control of infection in case of chronic osteomyelitis was around 4 months. Minimum duration for control of symptoms was 5 months. Maximum duration for control of symptoms was 7 months.
Conclusion: Antibiotic impregnated cement coated intramedullary nailing is a very good and effective treatment for infected nonunion and chronic osteomyelitis long bones with bone defect less than 2 cm. In case of infected nonunion, as the bone ends will be sclerosed, freshening of ends and bone grafting is needed.
Vancomycin, Methyl methacrylate, Infection, Antibiotic, Orthopedic treatment.
Paley et al. described novel technique of intramedullary antibiotic cement coated rods for intramedullary infections. This technique has evolved to antibiotic cement coated interlocking intramedullary nail insertion for the treatment of infected nonunion and the same was applied for treatment of chronic osteomyelitis.
Their aim was to identify the effective method in dealing with these difficult injuries. The use of reinforced antibiotic impregnated PMMA rods was studied to see if this could be an effective form of treatment. The use of such devices is beneficial because they provide stability that the fracture needs to heal and also provides a high concentration of antibiotic locally.
This is a prospective study conducted in Department of Orthopaedics and Traumatology, S.V.R.R Government General Hospital, Tirupathi, Andhra Pradesh, India. 20 cases admitted in hospital who were diagnosed of culture positive infected fractures of long bones and chronic osteomyelitis long bones were considered in the study. The study was conducted after obtaining approval from institutional ethical committee.
All cases were operated under regional anesthesia. The surgical parts were scrubbed, painted and draped. Wounds were subjected to through debridement. In case with implant in situ in case of nonunion and discharging sinuses, the implants were removed, the non-viable tissues thoroughly debrided till fresh bleed. The sclerotic ends of the fracture were freshened and sequestrectomy was done if needed. Osteotomy of fibula was done if necessary. Intra operative cultures were taken and sensitivity tested for deciding the post operative antibiotic protocol. After making the appropriate entry point, the guide wire is advanced till the fracture site, the fracture is adequately reduced and the guide wire is advanced into the distal fracture fragment. The guide wire is seated in the sub chondral bone. Serial reaming was done till the maximum diameter using hand held reamers. Nail diameter and length were determined. The cement mantle around the nail should be of around 2 mm. Hence the nail of 2 mm less than the required for regular nailing was chosen. In case if the nail of smaller diameter has to be chosen, solid nail was used.
Wound inspection at regular intervals of 48-72 hours till suture removal. Post operative complete hemogram, ESR and CRP were advised to assess the response to treatment. Systemic antibiotics were given for 5 days and there after oral antibiotics for 1 week. Range of movements exercises are started immediately on the first post operative day. Radiographs were taken post operatively in two planes, anteroposterior and lateral. Radiographs were taken thereafter at 6 weeks to assess the bony union. The patients were reviewed at 3 weeks to assess the status of infection control.
The effectiveness of antibiotic cement coated nail in management of infected fractures of long bones and chronic osteomyelitis long bones are evaluated through the following parameters: Improvement in symptoms like cessation of discharge, Reduction in signs of inflammation, Duration of hospital stay, Duration of union, Time period for weight bearing, Radiological confirmation of union, Complications.
The final outcome is graded based on ASAMI criteria proposed by Paley et al. This was originally developed for determining the outcome after treatment of nonunion with Ilizarov ring fixator. It was applied in our study with some modification.
The outcome can be graded as excellent only if the union is achieved without any bone grafting (Table 1).
|
Bony criteria |
Union |
Infection |
Deformity |
Limb length |
|
Excellent |
Union |
Nil |
<7 deg |
<2.5 cm |
|
Good |
Union |
With any two criteria |
|
|
|
Fair |
Union |
With any one criterion |
|
|
|
Poor |
Non union |
With or without above criteria |
|
|
|
Functional |
Activity |
Significant |
Stiffness at |
Soft tissue |
Pain |
|
Excellent |
Active |
Nil |
Nil |
Nil |
Nil |
|
Good |
Active |
With any one or two criteria |
|
|
|
|
Fair |
Active |
With three or four criteria |
|
|
|
|
Poor |
Inactive |
With or without the above criteria |
|
|
|
The final outcome is graded based on ASAMI criteria proposed by Paley et al. This was developed for determining the outcome after treatment of nonunion with Ilizarov ring fixator. It was applied in the present study with some modification.
Sample size of the present study was 20 (N=20). Age ranged between 20 years to 70 years. Male to female ratio was 9:1. That is 18 males to 2 females. Left sided limbs were more involved than to right in a ratio of 55% left to 45% right. Tibial fractures constituted 65% and femur fractures constituded 35%. Thirty percent of patients presented as chronic osteomyelitis and rest 60% presented as infected nonunion.
The average duration for achieving bony union was around 5 months (20 weeks). Minimum duration for bony union was around 4 months (16 weeks). Maximum duration for bony union was around 7 months (28 weeks), Average duration for control of infection in case of chronic osteomyelitis was around 4 months. Minimum duration for control of symptoms was 5 months. Maximum duration for control of symptoms was 7 months (Table 3). One patient did not achieve union and two patients achieved union in spite of sustained infection. Example of a case of infected non union both bones leg treated with anti biotic nail given in (Figure 1).
|
Time in months |
Number |
Percentage |
|
2 months |
- |
- |
|
3 months |
08 |
40% |
|
4 months |
03 |
15% |
|
5 months |
09 |
45% |
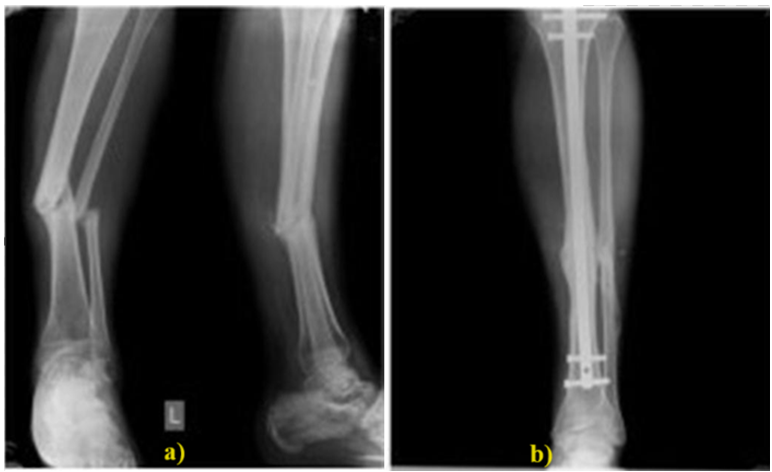 Figure 1: a): Infected non union both bones left leg pre-op; b): 12 weeks post-op.
Figure 1: a): Infected non union both bones left leg pre-op; b): 12 weeks post-op.Paley et al. in 2002 first used intramedullary rods coated with antibiotic cement to treat osteomyelitis in their series of 9 cases. Though union was not achieved, the infection was controlled in all cases with no recurrence [1]. The mean age of patients in present study was 39. This was comparable with the study population of Bhatia et al (mean age 39 years). The highest incidence of nonunion was in the patients of age 25 years to 40 years followed by age around 55 years [2].
The reason being most of their patients sustained compound fractures (13 patients) and most of them have Gustilo type IIIB. It accounts for nearly 50%. These compound fractures were more prone to infected nonunion and chronic osteomyelitis.
Present study population consisted of patients with bone defect of less than 2 cm. Shyam et al. in their study divided the patients into three groups based on the bone defect and mentioned that antibiotic nailing is effective in achieving the union with control of infection with bone defect of less than 4 cm. In between 4 and 6 cm, the technique was effective in controlling infection but not union. They opined that in case of bone defect of more than 6 cm, it is better to go for distraction osteogenesis by Ilizarov technique [3]. May et al. classified treatment by gap nonunion less than 6 cm and more than 6 cm group and obtained similar results [4]. In the present study patients had bone defect of around 2 cm and thus union was achieved in all cases.
With the present study, antibiotic cement impregnated nailing was used as an index procedure in 3 cases for infected fractures. For rest, the index procedure was either regular nailing and external fixator. Schmidmaier et al used gentamycin coated IM nail in 51.5% of his study population. Their study included only 21.2% compound fractures. Union was achieved in 71.2% population and nonunion was seen in 4.5% patients. This was the first study to conclude the use of antibiotic coated nail in prophylaxis of deep SSI [5].
Bony union was achieved in 13 out of 14 cases in our study. This was comparable with many other studies. Thonse et al achieved 84% bony union in their study of 52 patients, which was the largest study on antibiotic cement coated interlocking intramedullary nail for infected nonunion. In their study the union was around 73.1% of patients [6]. But Bhaitia et al. could achieve only 60 % of bone union. They used antibiotic coated K nail instead of ILN [2]. Shyam et al. studied the efficacy of infection control in infected nonunion using antibiotic cement coated interlocking nail and achieved union in 3 of 25 patients using antibiotic cement coated interlocking intramedullary nail alone [3]. Saravanan et al. achieved union in 23 out of 25 patients out of which 20 patients had union with antibiotic cement coated K nail.
Infection control was achieved in 4 of 6 patients. So, the percentage of infection control is around 66.6% [7]. Thonse et al. reported 85% of infection control in the year 2008 of his study [6]. Shyam et al reported that use of antibiotic cement coated nailing achieved infection control better than union even in defect nonunion of up to 6 cm bone loss. Infection was controlled in 80% of population. But union was achieved in patients with bone defect of more than 6 cm only by use of ilizarov technique [3].
Perhaps the most famous study conducted on antibiotic cement coated intra medullary spacers was done by Paley et al. in 2002, which is the first study to report the use of fabricated intra medullary spacers and they achieved control of infection in all 9 patients. These antibiotic coated rods act as intra medullary spacers filling the dead space and eluting antibiotic maintaining higher concentration locally even up to 36 weeks and providing stability at the same time. A combination of vancomycin and tobramycin was used in their study [1]. Bhatia et al. achieved 95% infection control using vancomycin and teicoplanin.
Konstantinos Anagnostakos et al. recommended certain combinations of antibiotics with PMMA cement depending on the authors experience and the recommendations of the manufacturers advise [9]. A list of cauasative organisms and the antibiotic combinations with PMMA cement were given in the Table 4.
|
Pathogen |
Antibiotic Combination |
|
Methicillin-susceptible S.aureus |
0.5 g gentamicin + 2 g vancomycin |
|
Methicillin-resistant S. aureus |
0.5 g gentamicin + 2 g vancomycin |
|
Methicillin-susceptible coagulase-negative Staphyloccoci |
0.5 g gentamicin + 2 g vancomycin |
|
Methicillin-susceptible coagulasenegative Staphyloccoci |
1 g gentamicin + 1 g clindamycin + 2 g vancomycin |
|
Enterococci |
0.5 g gentamicin + 2 g vancomycin or 0.5 g gentamicin + 0.8 g teicoplanin |
|
E. coli |
0.5 g gentamicin+ 2 g cefotaxime |
|
Pseudomonas aeruginosa |
0.5 g gentamicin + 2 g cefotaxime or 0.5 g gentamicin+ 2 g meropenem |
The addition of second antibiotic increases the elution of both the antibiotics. This is defined as passive opportunism [10].
The average duration of bony union in the present study was about 20 weeks and that for control of symptoms was around 16 weeks. This was in accordance with other studies. Bhatia et al. showed 32 weeks as an average duration of bone union [2]. Saravanam et al showed 26 weeks for tibia and 24 weeks for femur [7]. Han et al. showed union times of 26.4 weeks for tibia and 31.5 weeks for femur. All studies report an average time union of around 5 to 8 months [8].
ASAMI criteria were used to assess the bone and the functional outcome in the present study. The bone criteria were excellent in 12, good in 6 and poor in 2. Similarly, the functional outcome by ASAMI criteria was excellent in 12, good in 6 and poor in 2 patients. The above results suggest that the infection control and bony union can be achieved much early and by cost effective methods using antibiotic impregnated cement coated intramedullary nailing that has been agreed on to by various authors based on their result as cited above. Newer advancements in antibiotic cement coated interlocking intramedullary nail like MRI compatible carbon fiber antibiotic cement coated interlocking intra medullary nail has been used to see the progress of osteomyelitis using imaging techniques based on the excellent results achieved in various studies.
The biggest advantage of the antibiotic nail is that both the union and the infection can be addressed at the very same time. Single staged antibiotic nailing technique provides good results, lessens the duration of hospital stay, reduces the morbidity in infected nonunion of long bones with defect less than 2 cm. In patients with defects more than 4 cm antibiotic cement coated nailing can control the infection but to a lesser extent the nonunion. Thus, to say finally antibiotic impregnated cement coated intramedullary nailing is a very good and effective treatment for infected nonunion and chronic osteomyelitis long bones with bone defect less than 2 cm. In case of infected nonunion, as the bone ends will be sclerosed, freshening of ends and bone grafting is needed.
The authors have no conflicts of interest to report.
No.

