 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Anubha Bajaj*
Consultant Histopathologist, AB Diagnostics, India
Corresponding author: Anubha Bajaj, Consultant Histopathologist, AB Diagnostics, India; E-mail: anubha.bajaj@gmail.com
Received date: April 12, 2020; Accepted date: April 21, 2020; Published date: April 28, 2020
Citation: Bajaj A (2020) Acutely Inflamed Mamilla - Mastitis and Abscess. J Med Res Surg. 1(3): pp. 1-7.
Copyright: ©2020 Bajaj A. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Mastitis is an inflammation of breast parenchyma, predominantly occurring in the breastfeeding period, with or without accompanying infection and appears as lactational or puerperal and non-lactational as is associated with duct ectasia. Breast abscess is a focal accumulation of purulent substances within the breast parenchyma emerging as a complication of mastitis and is common in lactating women. Comprehensive incidence of mastitis is around 33% whereas breast abscess arises in approximately 3% to 11% of subjects with mastitis.
An estimated two fifths (40%) of breast abscess or certain breast infections are poly-microbial and specific aerobes such as Staphylococcus, Streptococcus, Enterobacteriaceae, Corynebacterium, Escherichia coli and Pseudomonas along with anaerobes as with Pepto-streptococcus, Propionibacterium, Bacteroides, Lactobacillus, Eubacterium, Clostridium, Fusobacterium and Veillonella can engender the disease. Subjects with mastitis enunciate flu-like symptoms with malaise, myalgia, fever, mammary pain, decline in milk egress, local warmth, tenderness, firmness and swelling of breast region and localized erythema. Breast abscess usually delineates mammary pain and/or a breast lump. Lactational breast abscess morphologically recapitulates an acute inflammation whereas non-lactational breast abscess is commonly sub-areolar and appears as a fistula of lacteriferous ducts, eventually emerging as chronically draining sinuses and breast abscess adjacent to the areola. Squamous metaplasia of lacteriferous duct epithelium, duct obstruction, and sub-areolar ductal dilatation or duct ectasia can ensue.
Breast, Aerobes, Anaerobes
The infection of the mammary tissue is categorized into lactational and non-lactational varieties and puerperal and non-puerperal subdivisions. Breast infection can be enunciated within superficial cutaneous surfaces or deep-seated mammary tissue [1]. Mastitis is a frequently occurring condition of the breast which predominantly implicates the breastfeeding period, although no period is exempt.
Mastitis is denominated as inflammation of breast parenchyma with or without accompanying infection. Mastitis with infection can appear lactational or puerperal and non-lactational as is associated with duct ectasia. Non-infectious mastitis can be engendered as idiopathic granulomatous inflammation or as associated inflammatory conditions such as a foreign body reaction [1]. Breast abscess is designated as a focal accumulation of purulent substances within the breast parenchyma appearing as a complication of mastitis. Breast abscess is frequent in lactating women although non- lactating women can be implicated and demonstrates an enhanced percentage of reoccurrence.
Non-lactating females can demonstrate a non-resolving breast abscess and an exclusion of inflammatory breast cancer is required. The male breast can be implicated. Breast abscess can arise in neonates. Lactational breast abscess is usually peripheral whereas non-lactational abscess is typically periareolar or subareolar [1,2].
The global incidence of lactational mastitis is an estimated 1% to10% although a comprehensive incidence of mastitis can be up to around 33%. The incidence of mastitis is enhanced within the immediate postpartum period although incidence declines gradually. Duct ectasia, peri-ductal mastitis or ductular dilatation can be associated with inflammation in nearly 5% to 9% in nonlactating females. Breast abscess can arise in approximately 3% to 11% of subjects with mastitis with a rough incidence of 0.1% to 3% in breastfeeding women. Breast abscess commonly implicates females betwixt 18 years to 50 years of age. Women of reproductive age group commonly delineate lactational abscesses, although non-lactational abscesses can be discerned premenopausal, elderly females [2,3]. Neonatal mastitis commonly appears in term or near term infants, demonstrates a female preponderance with a female to male ratio of 2:1. Approximately half (50%) of infants demonstrating neonatal mastitis can delineate an ensuing breast abscess. Breast abscess can also be generated with infected sebaceous cyst and hidradenitis suppurativa. Aforesaid causes of breast abscess mandate a distinctive evaluation and treatment. Lactational breast abscess is usually situated within peripheral breast tissue and often appears as a manifestation of mastitis or inflammation of lactating breast tissue. Occasionally, haematogenous dissemination is observed from an adjacent or distant infection [2,3]. Lactational breast abscess is common in primigravida exceeding >30 years of age, gestation beyond >41 weeks and concurrent mastitis. Preliminary infection is confined to a singular breast segment and extension into abutting segments is delayed. Lactose rich breast milk is an ideal environment for bacterial multiplication, thus bacterial dissemination within dilated breast segment and adjoining vasculature is convenient.
The lactation phase of childbearing women is commonly associated with breast infection which is enunciated in an estimated 10% to 33% instances. Lactational mastitis emerges in around 2% to 3% individuals and approximately 5% to 11% of subjects can develop a breast abscess. Lactational breast abscess appears during reproductive years with a mean age of 32 years [2,3]. Non- lactational breast abscess commonly peaks during the fourth decade. Obese and African- American females demonstrate a higher incidence of breast abscess. Also, nipple piercing can be associated with non-lactating sub-areolar breast abscess. Non- lactational breast abscess are frequent in obese women and smokers, in contrast to the general population. Smoking and diabetes mellitus are contemplated as significant factors in the emergence of periductal mastitis and non-lactational breast abscess. New-onset diabetes can represent as a breast abscess [2,3].
Mastitis can be categorized as infective or non-infective. Infectious mastitis and breast abscess are essentially engendered by bacteria colonizing the cutaneous surfaces. Staphylococcus aureus is a frequent contaminant and currently denominated as Methicillin-Resistant Staphylococcus Aureus (MRSA) with sequential coagulase-negative Staphylococci. An estimated two fifths (40%) of breast abscess or certain breast infections can be poly-microbial and specific aerobes such as Staphylococcus, Streptococcus, Enterobacteriaceae, Corynebacterium, Escherichia coli and Pseudomonas along with anaerobes as with Pepto-streptococcus, Propionibacterium, Bacteroides, Lactobacillus, Eubacterium, Clostridium, Fusobacterium and Veillonella can be recovered [3,4]. Anaerobes can occasionally be isolated from breast abscess and chronic instances with reoccurrence.
As such, primary and relapsing breast abscess delineate anaerobes (15%), especially in smokers. Infrequently discerned pathogens comprise of Bartonella henselae (cat scratch disease), Mycobacteria (tuberculosis and atypical tuberculosis), Actinomyces, Brucella, fungi (Candida and Cryptococcus), parasites and infestation with maggots. Uncommon infections of breast parenchyma can be indicative of infection with Human Immune Deficiency (HIV) [3,4]. Salmonella infection can induce breast abscess, especially in geographical areas of disease prevalence. Non-infectious mastitis ensues from concomitant duct ectasia such as peri-ductal or plasma cell mastitis and exceptionally from foreign bodies as exemplified with nipple piercing, breast implants or silicone. Lobular (granulomatous) mastitis is an idiopathic, benign disease probably due to Corynebacterium infection [3,4].
Lactational mastitis emerges on account of bacterial accumulation within the infant’s mouth which ingresses into the breast parenchyma through cracks and fissures of the nipple. Discontinuity of the primary defense mechanism provides the offending organisms with an ideal culture medium with rich nutrients of maternal milk which generates a brisk bacterial replication. Aforesaid bacterial propagation can be enhanced with excessive secretion and stasis of milk with consequent mastitis [3,4]. Neonates demonstrate a transient breast enlargement on account of the transmission of secreted maternal hormones with a consequent susceptibility to mastitis. Breast abscess appearing in lactating and non-lactating females are distinct clinical entities with diverse pathogenesis. Lactational breast abscess is a frequent condition albeit with a declining incidence. Aforesaid abscesses are initiated by infection with Staphylococcus aureus, Streptococcus species, and MRSA [4]. Breast abscesses arising on account of lactation are engendered by a tissue abrasion within the nipple wherein a bacterial ingress initiates the infection. Commonly enunciated within the second postpartum week, concurrent milk stasis enhances the infection. Besides Staphylococcus aureus and Streptococcal species, Staphylococci epidermidis can be implicated. The majority (90%) of non-lactational breast abscess appear within the sub-areolar region, preponderantly within the late reproductive phase, whereas around 10% of non-lactational breast abscess can be engendered by exceptional bacterial, fungal or granulomatous inflammation. Characteristically, a non-lactational breast abscess arises on account of infection with a mixed bacterial flora of Staphylococcus aureus, Streptococcus species and anaerobic bacteria [4,5].
Untreated mastitis can generate sufficient decimation of mammary tissue with the subsequent appearance of an abscess. Mastitis or breast abscess demonstrates a typical clinical representation and a history. Breast abscess usually delineates mammary pain and /or a breast lump. Subjects with mastitis enunciate flu-like symptoms with malaise, myalgia, fever, mammary pain, decline in milk egress, local warmth, tenderness, firmness and swelling of breast region and localized erythema. A non-specific history of probable oedema, lactation, preceding breast infection and prior treatment can be elicited. Also, tachycardia, nausea, vomiting, purulent discharge from the nipple or erythematous foci are mentioned [4,5]. Physical examination demonstrates erythema, induration, warmth, and tenderness upon palpation.
Also, a palpable fluctuant mass with a purulent discharge from the nipple or incriminated site is observed. Reactive axillary lymphadenopathy is an accompaniment. In addition to the aforementioned symptoms, breast abscess demonstrates a well-circumscribed, fluctuant mass. The deep-seated mass may or may not be palpable [5]. Resistant, reoccurring or chronic infections with ensuing chronic pain and scarring can be cogitated [5].
Lactational breast abscess recapitulates an acute inflammation, although the morphology of lactating breast with loose, intervening parenchyma, engorgement of breast segment with stagnant milk can enhance the dissemination of infection within breast stroma and epithelium lined milk ducts [5,6]. Non-lactational breast abscess is commonly sub-areolar and was initially scripted by Zuska as a fistula of lactiferous ducts. Subsequently, chronically draining sinuses and breast abscess is configured adjacent to the areola. Squamous metaplasia of lacteriferous duct epithelium, obstruction of ducts and sub-areolar ductal dilatation or duct ectasia can ensue. Additionally, preceding inflammation of enveloping ducts, infection of terminal lacteriferous ducts, duct rupture with subsequent articulation of periareolar fistula and sub-areolar breast abscess is observed [5,6]. Lacteriferous ducts depict a squamous metaplasia or epidermalization which in association with keratin production can ensure a blockage of ducts with a subsequent configuration of breast abscess. Aforesaid breast abscess depicts a chronic pattern of evolution along with reoccurring obstruction of ducts, keratin plugs and a penchant for configuring extensive proportions of fistula [5,6]. Emergence of centric, periareolar, non-lactational abscess is secondary to peri-ductal mastitis. Duct ectasia delineates a specific sequence of events wherein inflammation of mammary ducts engender a distinct squamous metaplasia and ensuing.
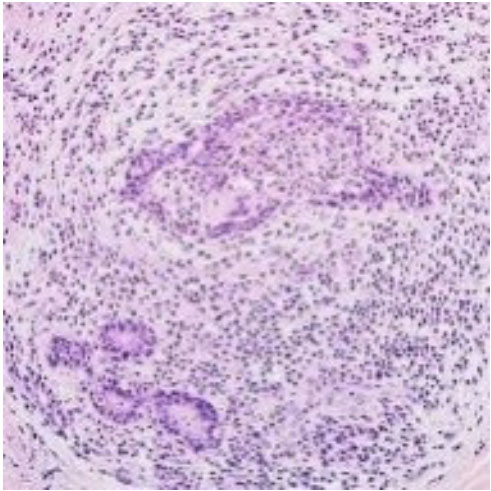 Figure 1: Mastitis-acute inflammation with duct ectasia, squamous metaplasia and peri-ductal inflammation [10].
Figure 1: Mastitis-acute inflammation with duct ectasia, squamous metaplasia and peri-ductal inflammation [10].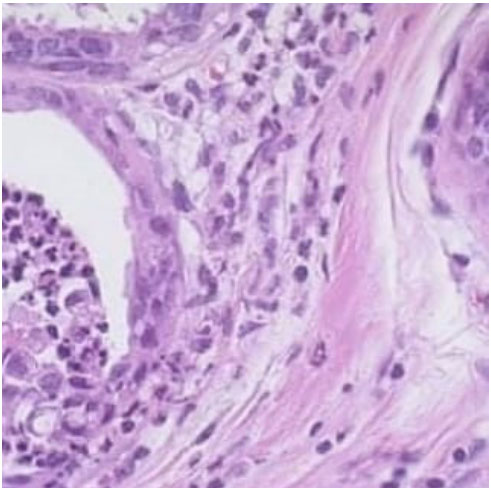 Figure 2: Mastitis- acute neutrophilic egress with duct dilatation and focal
squamous metaplasia [11].
Figure 2: Mastitis- acute neutrophilic egress with duct dilatation and focal
squamous metaplasia [11].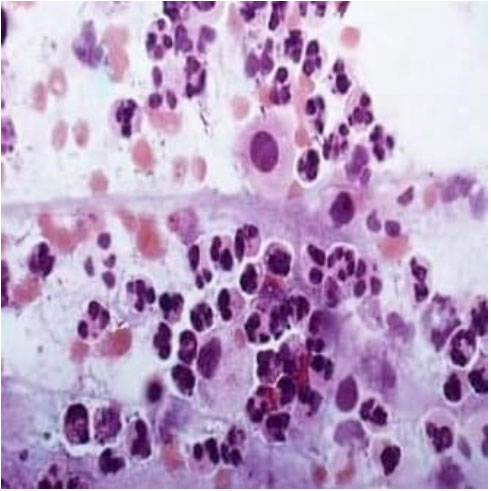 Figure 3: Mastitis upon fine needle aspiration with an accumulation of
acute inflammatory cells viz neutrophils admixed with few histiocytes and
occasional plasma cells [11]
Figure 3: Mastitis upon fine needle aspiration with an accumulation of
acute inflammatory cells viz neutrophils admixed with few histiocytes and
occasional plasma cells [11]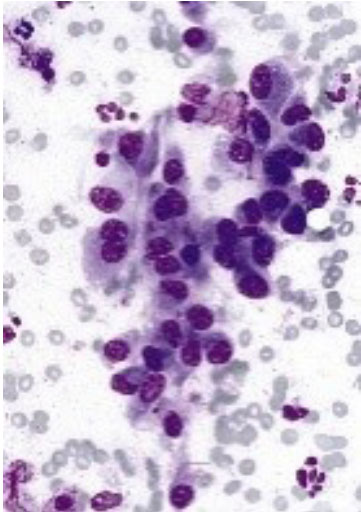 Figure 4:Mastitis as depicted on needle aspiration with aggregates of
acute inflammatory cells, macrophages, benign ductal epithelial cells and
adipose tissue fragments [12].
Figure 4:Mastitis as depicted on needle aspiration with aggregates of
acute inflammatory cells, macrophages, benign ductal epithelial cells and
adipose tissue fragments [12].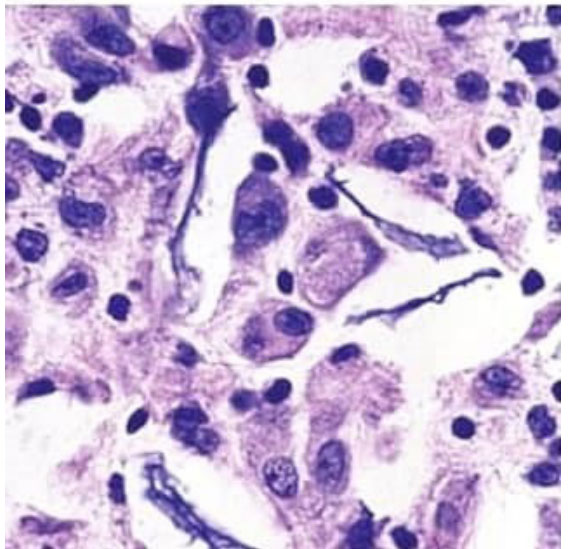 Figure 5:Mastitis demonstrating acute inflammatory egress, plasma cells,
macrophages with configured breast abscess delineating accumulation of
purulent material [12].
Figure 5:Mastitis demonstrating acute inflammatory egress, plasma cells,
macrophages with configured breast abscess delineating accumulation of
purulent material [12].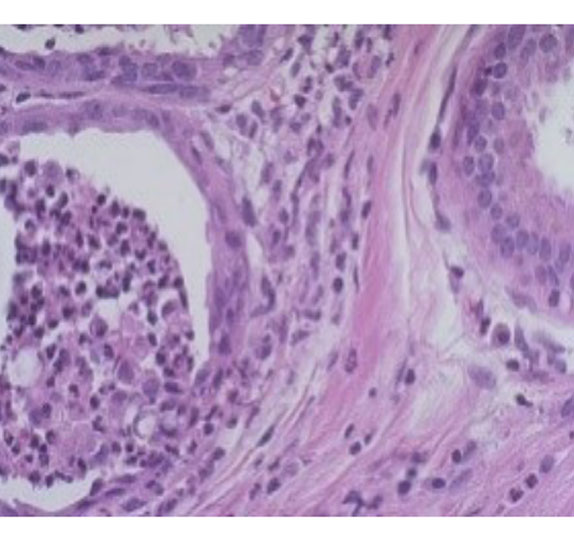 Figure 6: Mastitis with acute inflammatory infiltrate of neutrophils obstructing dilated ducts along with aggregation of purulent substance articulating a breast abscess [13].
Figure 6: Mastitis with acute inflammatory infiltrate of neutrophils obstructing dilated ducts along with aggregation of purulent substance articulating a breast abscess [13].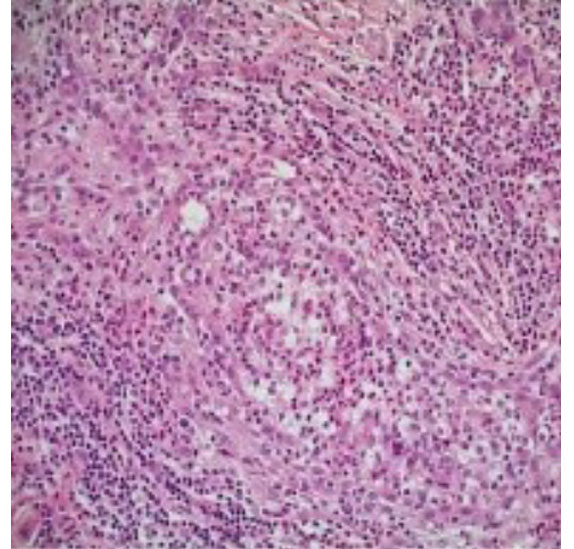 Figure 7:Mastitis delineating acute inflammatory cells impacting and surrounding mammary ducts accompanied by duct ectasia [14].
Figure 7:Mastitis delineating acute inflammatory cells impacting and surrounding mammary ducts accompanied by duct ectasia [14].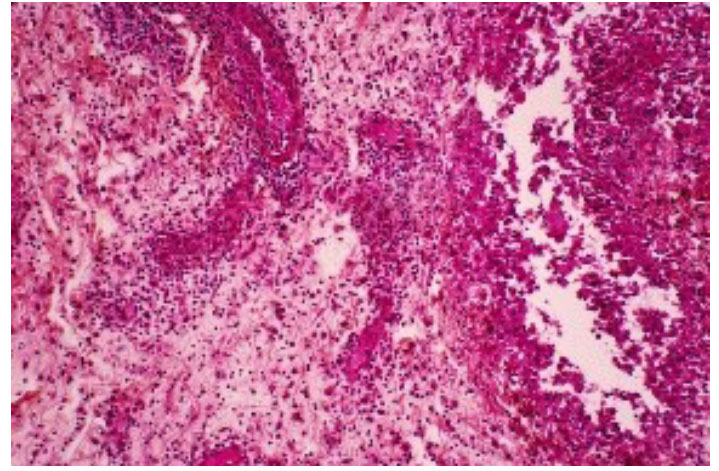 Figure 8:Mastitis elucidating accumulation of neutrophils, macrophages
and degenerated cells accompanied by suppuration and ductal dilatation
arranging a breast abscess [15].
Figure 8:Mastitis elucidating accumulation of neutrophils, macrophages
and degenerated cells accompanied by suppuration and ductal dilatation
arranging a breast abscess [15].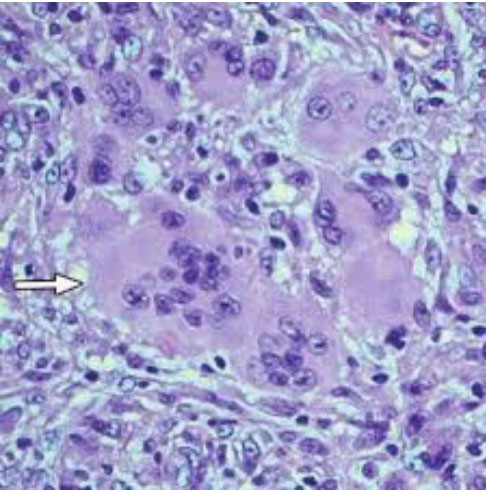 Figure 9:Mastitis demonstrating a chronic inflammatory egress of plasm
cells, lymphocytes, and histiocytes associated with a foreign body giant cell
reaction [16].
Figure 9:Mastitis demonstrating a chronic inflammatory egress of plasm
cells, lymphocytes, and histiocytes associated with a foreign body giant cell
reaction [16]. 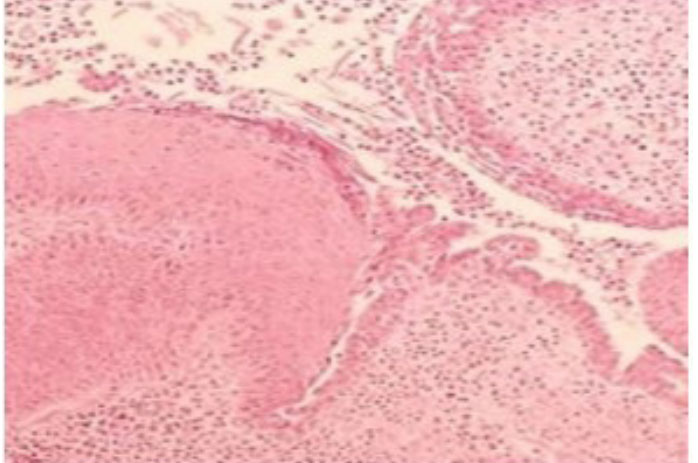 Figure 10:Mastitis with an inflammatory exudate of neutrophils and macrophages with a circumscription of ductal and peri-ductal region [17].
Figure 10:Mastitis with an inflammatory exudate of neutrophils and macrophages with a circumscription of ductal and peri-ductal region [17].Ultrasound examination is a preferred imaging modality for diagnosing breast infection within comprehensive age groups from neonates to the elderly. Ultrasonography is beneficial and depicts a breast abscess as a hypoechoic lesion. Alternatively, a well-circumscribed, macro-lobulated, irregular or poorly defined, probably septate mass can be delineated. Hypoechoic perimeter is suggestive of the thickened wall of a chronic breast abscess [6]. Fine Needle Aspiration Cytology (FNAC) is employed to evacuate a breast abscess for diagnostic and therapeutic purposes. Aspiration of purulent fluid with a needle is indicative of a breast abscess.
A routine cytological assessment can exclude a malignant transformation [6]. Additionally, aspiration of milk, fluid suppuration, and extracted tissue can be evaluated for culture and sensitivity. Bacterial growth appearing within a suitable culture medium indicates an infection and a cogent antibiotic sensitivity is applicable for the selection of appropriate, therapeutic antibiotics [6,7]. Unsuspected occurrence of mastitis in specific age groups such as adolescents mandates the exclusion of a pregnancy. Tissue examination is unnecessary for clear- cut instances of breast abscess. Individuals with suspicious breast abscess, atypical clinical presentation, debatable diagnosis or complications as with reoccurring infection or therapeutic failure mandate a cogent histological examination [6,7].
Pertinent tissue examination is inclusive of ultrasound-guided or non-guided FNAC. Tissue specimens can be obtained as an excisional or incisional biopsy, core needle biopsy or a vacuum-assisted biopsy. Tissue evaluation is required to discern infection, granulomatous inflammation or malignant conversion of mammary tissue [6,7]. Histological and cytological assessment of excised tissue is necessitated for diagnosing malignant transformation and tissue infection, especially with the employment of pertinent fungal stains or Ziehl-Neelsen stain for acid-fast bacilli, particularly in instances of refractory and relapsing disease. Punch biopsy of the skin can be utilized to detect inflammatory carcinoma of the breast [7].
Besides, secreted milk, nipple discharge, purulent material or excised tissue can be subjected to Gram’s stains, culture and sensitivity for aerobic and anaerobic bacteria along with investigations for fungal and mycobacterial infection [7]. Mammography as an examining tool provides a limited benefit in the assessment in acute mastitis and breast abscess. The procedure can be painful and demonstrate nondiagnostic findings. Tissue anomalies, architectural distortion, spiculated nodule, cutaneous retraction and thickening, micro-calcifications and focal or diffuse enhancement of tissue density can be discerned. Aforesaid nonspecific mammographic features can recapitulate a malignant mass [7,8]. Mammography can be beneficial with the resolution of acute, infective phase to identify concurrent breast lesions. Women exceeding 40 years of age, subjects with complex or atypical clinical representations or an absence of suspicious malignancy will benefit from mammography performed at the termination of the acute phase. Investigations such as a complete blood count with a differential count and suitable blood cultures are applicable in suspected systemic infections, distinct soft tissue abscess, relapsing infection and therapeutic failure [7,8]. Lactational mastitis mandates an accurate examination of the infant’s oral cavity, cutaneous surfaces, and diaper zone. Recurrent mastitis can be suggestive of a Staphylococcal carrier state [8].
Competent management of mastitis with suitable antibiotics can circumvent ensuing complications. Appropriately timed referral is crucial in preventing the occurrence of severe infection or sepsis as delayed treatment can ensure inferior outcomes. Treatment regimens are composed of the administration of pertinent antibiotics. Breast abscess can be managed with percutaneous drainage and/or surgical incision and drainage [8,9]. Efficacious, ultrasound-guided, percutaneous drainage is frequently adopted which can circumvent the requirement of an invasive, surgical incision and drainage, even in enlarged breast abscesses. Microbial preponderance of Staphylococcal aureus permits a rational selection of sensitive antibiotics without the employment of a culture.
Following the resolution of the acute phase of breast abscess, chronically infected tissue and major lacteriferous ducts mandate a surgical extermination. Reoccurrence of breast abscess is engendered with a minimal duration of therapy, inappropriate or delayed administration of antibiotics/ therapeutic agents or the emergence of Staphylococcal carrier stage. Acute and chronic complications can emerge with breast abscess [8,9].
Acute complications can progress to a cessation of breastfeeding. Also, mammary infections are associated with haematogenous dissemination, bacteremia with consequent sepsis, especially cogitated in immunocompromised and elderly subjects. Chronic complications are exemplified as cutaneous and adjacent soft tissue scarring and breast infection. Inappropriately treated abscess can generate significant scarring. Relapsing mastitis can engender the deformity of the breast. Implicated infants can delineate asymmetry or hypoplasia of the breast. Mastitis with Staphylococcus aureus can demonstrate a significant proportion of cutaneous infections, particularly at extramammary sites [9].
The infection of the mammary tissue requires a rapid diagnosis and appropriate management to circumvent complications. Prompt administration of efficacious antibiotics in necessitated in suspected mammary infection in addition to a preliminary, appropriate, secondary referral which enhances prognostic outcomes. Lactational mastitis can be adequately managed with supportive care such as efficacious analgesia, employment of warm compress and milk extraction from an implicated breast. Instances devoid of indication of systemic infection or lack of bacterial isolation upon culture do not require therapy. Symptomatic subjects can be administered an accurate selection of antibiotics contingent on bacterial sensitivity [8,9]. Emergence of Methicillin-Resistant Staphylococcus Aureus (MRSA) engendering mammary infection requires adequate discernment. Infections devoid of MRSA can be treated with flucloxacillin, erythromycin or clarithromycin. Infections delineating MRSA can be managed with co-amoxiclav, clindamycin or vancomycin. Antifungal therapy may be necessitated for treating candidiasis of the nipple. Antibiotics such as tetracycline, ciprofloxacin or chloramphenicol are unsuitable for lactating mothers as breast milk can secrete aforesaid antibiotics [8,9]. Non-lactational mastitis can be managed with appropriate supportive care. Infections with minimal quantities of MRSA and lack of penicillin allergy can be administered flucloxacillin or topical antibiotics. Infections contingent to MRSA is treated with co-amoxiclav, clindamycin or vancomycin. Appropriate therapy is required to treat the definitive, underlying disease. Mastitis arising is neonates, infants or children below < 12 years can be managed with supportive care. Antibiotics such as flucloxacillin, cefazolin, trimethoprim or sulfamethoxazole are efficacious.
Ineffective treatment requires a re-evaluation of diagnosis [8,9]. Peri-ductal mastitis is associated with tobacco abuse. Thus cessation of smoking is recommended. In the absence of MRSA infection, breast abscess can be treated with supportive care, appropriate analgesia, and flucloxacillin. Breast abscess with the isolation of MRSA can be managed with trimethoprim, sulfamethoxazole, clindamycin, doxycycline or vancomycin along with cessation of breastfeeding and supportive measures. Antibiotics such as nafcillin, unasyn or augmentin can be administered. Severe instances necessitating hospitalization can be administered antibiotics such as linezolid, tigecycline, and daptomycin. The duration of antibiotic administration is usually 7 days to 10 days(9). Breast abscess discerned in neonates, infants or children are subjected to antibiotic therapy contingent to the isolation of pathogen. Community-acquired MRSA can be administered trimethoprim, sulfamethoxazole or clindamycin. Doxycycline applies to children beyond >8 years of age. Vancomycin is effective in hospital-acquired MRSA infection. Abscesses delineating gramnegative bacilli can be managed with levofloxacin, especially in non-breastfeeding women, ceftriaxone or cefotaxime [8,9]. Breastfeeding or milk drainage with a breast pump to evacuate the incriminated ducts is recommended. Pain can be curtailed with Non-steroidal Anti-inflammatory Drugs (NSAID) and/or prescription narcotics.
Also, warm compress and moisturizer can be employed to circumvent cracked nipples [9]. Surgical therapeutic procedures are a requirement in fluctuant breast abscess. Breast abscess arising on account of an obstructed or ectatic lacteriferous duct may mandate a surgical extermination. Aspiration of the abscess with an 18 gauge to 21 gauge needle with a local anesthesia with or without ultrasound guidance is an efficacious manoeuver. Aspiration of the purulent material is associated with superior cosmetic outcomes and palliation. Multiple aspirations can be attempted in a duration of 5 days to 7 days for achieving a comprehensive drainage. Nonlactational breast abscess depicts an enhanced percentage of reoccurrence with a consequent necessity of multiple procedures of drainage Needle aspiration is suitable for breast abscess below 3 cm in magnitude or lactational breast abscess [8,9]. A shiny, stretched, necrotic and attenuated superimposed skin requires a miniature incision and drainage. Mini-incision is accompanied by an excellent cosmesis. Relapsing breast abscess following a needle aspiration can be managed with incision and drainage. Incision and drainage depict a minimal proportion of the reoccurrence rate.
However, as an invasive mechanism, the procedure is accompanied by scarring and inferior outcomes, in contrast to a needle aspiration [8,9]. Enlarged incisions with drainage of purulent substance under general anesthesia are beneficial where aspiration and miniature incision is inadequate and in draining abscesses beyond >5 cm diameter. A drainage catheter is advantageous in extracting voluminous quantities of pus. Enlarged breast abscess or the emergence of signs of sepsis may necessitate a hospital admission. Enlarged cavitation following incision and drainage can be packed to enhance the drainage of purulent material and prevent the closure of skin incision upon an insufficient drainage. Healing is brisk and usually by secondary intention [9].
Ultrasonography is a preferred and advantageous diagnostic modality and depicts a breast abscess as a hypoechoic lesion. Alternatively, it can demonstrate a well-circumscribed, macrolobulated, irregular or poorly defined, probably septate mass. Efficacious, ultrasound-guided, percutaneous drainage is frequently adopted which circumvents the requirement of an invasive, surgical incision and drainage. Appropriately timed referral is crucial in preventing the occurrence of severe infection or sepsis. Reoccurrence of breast abscess occurs with a minimum duration of therapy, inappropriate or delayed administration of antibiotics/ therapeutic agents or the emergence of the Staphylococcal carrier stage. Treatment regimens are composed of the administration of pertinent antibiotics. Breast abscess can be managed with percutaneous drainage and/or surgical incision and drainage.
MRSA engendering mammary infection requires adequate and preliminary discernment and is amenable to therapy with flucloxacillin, erythromycin or clarithromycin. Breast abscess wherein MRSA is isolated can be managed with trimethoprim, sulfamethoxazole, clindamycin, doxycycline or vancomycin along with cessation of breastfeeding and supportive measures. Antibiotics such as nafcillin, unasyn or augmentin can be administered. Severe instances require hospitalization and can be administered antibiotics such as linezolid, tigecycline, and daptomycin.
There are no conflicts of interest.

