 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Uzma Panhwer*, Bushra Shamim, Nimra Ali, Areeba Ahmed, Rida e Zainab
Liaquat National Hospital, Karachi, Pakistan.
Correspondence to: Uzma Panhwer, Liaquat National Hospital, Karachi, Pakistan.
Received date: November 13, 2023; Accepted date: November 28, 2023; Published date: December 05, 2023
Citation: Panhwer U, Shamim B, A, Ali N, et al. A Unique Case of Primary Subfrontal Lobe Meningioma with Intraorbital Extension. J Med Res Surg. 2023;4(6):112-114. doi: 10.52916/jmrs234121
Copyright: ©2023 Panhwer U, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted
use, distribution and reproduction in any medium, provided the original author and source are credited.
Introduction: Meningiomas, tumors originating from the meninges covering the brain, are typically considered benign. They primarily develop from arachnoid cap cells within the meninges and can manifest as primary orbital meningiomas (affecting structures like the optic nerve sheath) or secondary orbital meningiomas that extend from intracranial origins, such as the sphenoid wing and rarely from frontal lobe as in our case.
Case Presentation: This report documents a very rare case where a meningioma emerged in the subfrontal lobe of the brain and subsequently spread to the orbit. The presence of such malignant variants in the orbit poses unique diagnostic challenges due to their potential to compress critical adjacent brain structures.
Impact on Orbital Structures: The extension of these tumors into the orbit can have significant consequences, affecting structures like the cavernous sinus, superior orbital fissure, intraorbital contents, and the optic nerve. This further complicates their surgical management, given their proximity to essential neurological systems.
Conclusion: This case study underscores the atypical growth pattern of malignant meningioma and highlights the complexities associated with identifying and treating meningioma with orbital extensions. The propensity of these tumors to impact vital brain structures necessitates a comprehensive approach to their diagnosis and management.
Subfrontal, Meningioma, Intraorbital extension, MRI findings, Optic foramen, Optic nerve sheath.
Meningiomas are the most typical intracranial tumors, usually developing in people during their 4th and 6th decades of life. These growths often have a nonmalignant origin and develop slowly. Less than 10% of cases show aggressive features or distant metastases. They show a preference for women, with an incidence rate twice as high as that in males [1].
On the other hand, orbital meningiomas are thought to make about 3-9% of all intraorbital neoplasms [2,3]. Meningiomas of the primary orbital optic nerve usually compress the nerve as they grow in the subdural region. Axial proptosis or the forward displacement of the eye, optic atrophy, and injury to the optic nerve are all consequences of this compression. One eye also gradually loses eyesight. Disc shunt vessels may be visible during an ocular examination in circumstances when the anterior optic nerve is impacted. Headaches, nausea, vomiting, and papilledema, which is an enlargement of the optic disc, are all examples of clinical symptoms related to meningiomas coming from other parts of the skull [2-4].
Specifically, meningothelial cells or, less frequently, arachnoid tissue that is present ectopically are the genesis of primary orbital meningiomas, which develop in the sheath that protects the optic nerve. The subfrontal region, on the other hand, is the location of origin for secondary orbital meningiomas and only one case is reported in literature [1,3]. The orbital meningioma that developed in the subfrontal lobe is a unique instance that we report in the following description.
A 45-year-old male patient known case of hypertension was presented to OPD with complains of gradual loss of vision of right left eye and blurring of vision of left eye for 5 years.
On examination mild proptosis of right eye was noted. An MRI Orbit with contrast was done which showed a well-defined broad based extra axial abnormal signal intensity mass is seen in the right subfrontal region causing compression over the adjacent brain parenchyma. The mass was seen extending into the suprasellar cistern with encasement of the supraclinoid part of right internal carotid artery and its bifurcation with mild displacement of right middle and anterior cerebral arteries (Figure 1 and Figure 2). The intra cranial part approximately measures 2.4 × 2.4 × 1.2 cm.
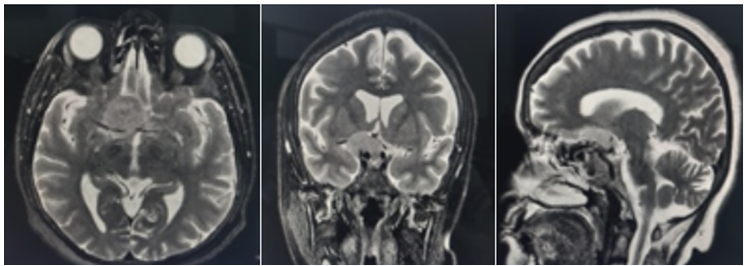 Figure 1: T2 WI axial, coronal and saggital view.
Figure 1: T2 WI axial, coronal and saggital view.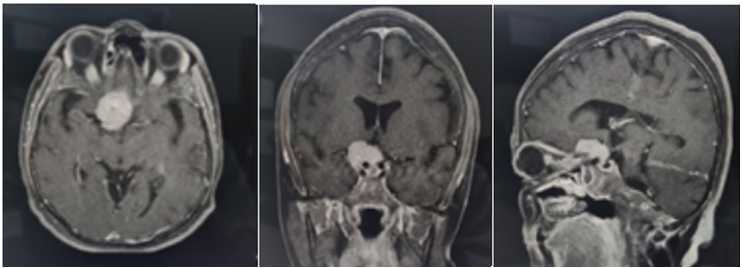 Figure 2: Post contrast bravo images.
Figure 2: Post contrast bravo images.Anteriorly the mass was seen extending through optic foramen, causing its widening and encasing optic nerve upto the right eye globe giving a tram track appearance. It appeared low on T1 and slightly hyperintense on T2 with homogeneous post contrast enhancement (Figure 2 and Figure 3). All those findings were concluded as a subfrontal meningioma on right side showing intra orbital extension through optic foramen and involving optic nerve sheath.
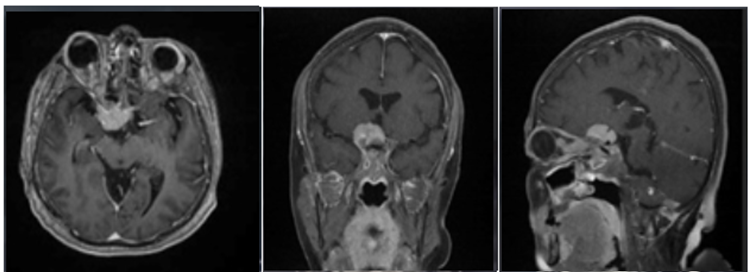 Figure 3: T1 post contrast FS images.
Figure 3: T1 post contrast FS images.Later the patient's was referred to ophthalmic plastics for further evaluation and management.
This case report delves into the intriguing behavior of meningiomas and their potential invasion into the orbit. One notable aspect of this case is the uncertainty surrounding the precise mechanism of orbital invasion [1]. The phenomenon of meningiomas invading the orbit through such sites is less common. The case is further complicated by radiological evidence strongly suggesting direct extension from the frontal lobe to the orbit, raising questions about the nature of the tumor's spread and highlighting the complex, multifaceted nature of orbital tumor invasion [2].
An alternative hypothesis proposed in this case is that the tumor penetrated the orbit through the optic foramina involving the optic nerve sheath. Certain subtypes of malignant meningiomas are known to exhibit bony destruction or hyperostosis, and they can extend into the orbit through the optic canal or the superior orbital fissure [2,3]. This mechanism of extension through the optic nerve has been documented in cases of various other brain tumors, including glioblastoma multiforme, pituitary tumors, and craniopharyngiomas. Notably, this case also underscores the rare extension of meningiomas, even without prior craniotomies, further emphasizing the uniqueness of the situation [3,4].
Magnetic Resonance Imaging (MRI), particularly gadolinium-enhanced fat-suppression sequences, is the preferred method for diagnosing meningioma with orbital extension, rendering tissue biopsies unnecessary [4]. Meningiomas appear isointense to grey matter on both T1 and T2 weighted MRI images, and they exhibit strong enhancement with gadolinium contrast compared to the non-enhancing optic nerve. This enhancement often presents as the "tram-track" sign on axial MRI scans as in our case, creating a "doughnut" or "non-enhancing dot" appearance on coronal imaging. The pattern of meningeal expansion around the optic nerve varies depending on the orbital extension of the meningioma [4,5].
Computed Tomography (CT) is valuable for imaging the orbit and skull, revealing bone structure and hyperostosis caused by secondary tumors, such as meningiomas. The "tram-track" sign can also be observed on CT scans. While meningiomas are not typically associated with metastasis, in rare instances where metastasis occurs, the lung is the most common site [4,5].
The management of orbital extension of meningiomas depends on the patient's symptoms and visual acuity. Patients with good visual acuity (20/50 or better) are usually monitored with regular neuroimaging and eye exams, while younger patients may require more frequent assessments [6] Surgical intervention is considered when tumors threaten vision or cause significant disfigurement, aiming for long-term tumor control, nerve function restoration, and cosmetic improvement. However, complete resection can be challenging, often requiring periodic debulking surgeries. Surgery can significantly improve visual acuity and proptosis in the majority of cases [7].
Radiation therapy is recommended before surgery for symptomatic patients, with careful consideration of the optic nerve and chiasm's sensitivity to radiation. Fractionated therapy with lower doses per fraction is favored to minimize the risk of damage. Studies suggest that radiation therapy as an initial treatment may lead to optimal visual outcomes [7]. Complications following surgery may include sensory issues and nerve problems, while ocular complications may arise post-radiation therapy [8].
Prognosis varies, with recurrence rates ranging from 17% to 42%, influenced by tumor grade and the use of radiation therapy [8]. Recurrence rates are lower when postoperative radiation is employed, and the tumor grade remains a key factor in prognosis. Management should be tailored to each case, taking into account symptoms, age, and tumor characteristics. Meningiomas originating over the brain's convexities are typically benign, with high potential for complete surgical excision when resected with a substantial margin. However, those with anaplastic pathology can exhibit high 5-year recurrence rates of up to 50%. Meningiomas are rarely metastatic, with distant extracranial metastases estimated to be as low as 0.001%, and the lung being the most common site [9,10].
In conclusion, this unique case report presents a secondary orbital meningioma originating from an unconventional site, the frontal lobe of the brain. The precise mechanism of orbital invasion remains uncertain. This case serves as a poignant reminder of the complex and occasionally aggressive nature of meningiomas, which may deviate from the conventional understanding of these tumors as typically benign. Careful consideration is imperative in the radiological reporting and surgical management of such cases to minimize risks and optimize patient outcomes.
The authors have no conflicts of interest to report.
No.
All authors have given their consent to publish this article.

