 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Ninad Godghate1* , Neha Godghate1, Aniruddha Wargantiwar2, Krishnamohan Saindane3
, Neha Godghate1, Aniruddha Wargantiwar2, Krishnamohan Saindane3
1Director, Grace Orthocare and Multispeciality Hospital, Nagpur, Maharashtra, India
2Consultant, Phoenix Orthopaedic super-speciality Hospital, Nagpur, Maharashtra, India
3Director, Suyog Hospital, Dhule, Maharashtra, India
Correspondence to: Ninad Godghate, Director, Grace Orthocare and Multispeciality Hospital, Nagpur, Maharashtra, India
Received date: August 09, 2022; Accepted date: August 19, 2022; Published date: August 26, 2022
Citation: Godghate N, Godghate N, Wargantiwar A, et al. A Small Step to Improve Tibial Alignment in Knee Replacement. J Med Res Surg. 2022; 3(S2): 4-7.
doi: 10.52916/jmrs22S202
Copyright: ©2022 Godghate N, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted
use, distribution and reproduction in any medium, provided the original author and source are credited.
Introduction: Though total Knee replacement has proved to be a rewarding surgery for patients with
end stage knee arthritis, errors in surgical technique leading to malalignment of components can lead
to early failure. The aim of this study was to increase the accuracy in identifying the centre of ankle joint
which is the first step in achieving a proper tibial cut for a well placed tibial implant.
Technique: We propose a simple, reproducible technique to locate centre of ankle under image
intensifier.
Results: The above technique was used in 30 patients who were operated by two surgeons during a
period of 6 months from January 2022 to June 2022. Post-op measurements of the alignment of tibial
implant were done electronically on computer and physically on X-rays. 21 of the 30 cases (70%) had
good placement of the implant within 1 degree of ideal alignment and 9 (30%) within 2 degrees.
Discussion: A correct proximal tibia cut for a well aligned tibial component is achieved with the help
of precise application of the cutting jigs. Extramedulalry jigs used to make the proximal tibia cut have
to be aligned parallel to the axis of the tibia and centred over the midpoint of talus. Several methods
have been proposed by various authors to locate centre of the ankle joint. However, at present there is
no consensus on the best method. Even computer navigation relies on accurate feeding of anatomical
reference points which is done manually.
Conclusion: Our technique is precise, accurate, repeatable, objective and less time consuming. It adds
value to achieving the final aim of a good implant position. The technique has a dual advantage as it gives
a better estimate of not only the centre of the ankle but also the centre of the distal tibial mechanical
axis.
Centre of ankle, Tibial component alignment, Knee replacement, Fluoroscopic guidance, X-ray
AP: Antero-Posterior; ECG: Electrocardiogram; EHL: Extensor Hallucis Longus; MRI: Magnetic Resonance Imaging; BMI: Body Mass Index
Total knee replacement has proved to be a rewarding surgery for patients with end stage knee arthritis. Multiple studies have shown more than 95% prosthesis survival at 15 years. The placement of implants in proper alignment is crucial for successful outcome. Alignment errors of more than 3 degrees have been shown to result in early failure through accelerated wear and loosening of components. There is a significantly high revision rate for tibial components placed in varus [1-3].
The proponents of mechanical alignment aim to align the tibial prosthesis perpendicular to the mechanical axis of tibia with a deviation of no more than 3 degrees. The proximal tibial cut is usually the key step that determines the overall alignment of the knee. The role of Robotic Surgery and Computer Navigation in total knee replacement is now well established. However, most knee replacements done today rely on manual instrumentation and surgeon’s judgement to achieve the aim of ideal alignment.
Intra-medullary and extra-medullary alignment guides are the most used methods to execute the distal femoral and proximal tibial cuts, each having its own set of advantages and disadvantages [4]. Extra-medullary guides are more popular for tibial alignment. The aim is to align the guide on an axis connecting the centre of ankle to the centre of knee. Therefore, locating the centre of ankle is the crucial first step in the placement of this guide. Many techniques have been described to help the surgeon locate the centre of the ankle. A number of bony and soft tissue marker points have been proposed as distal tibial reference points; these include the second metatarsal, the extensor hallucis longus tendon, the tibialis anterior tendon, the extensor digitorum longus tendon, and the dorsalis pedis artery [5-9]. However, there is no consensus on the best method available.
Through this study, we propose a simple, objective and a repeatable technique to locate the centre of ankle joint using intra-operative fluoroscopic guidance.
The technique can be done before or after induction of anaesthesia. To save surgical time, we have also done it during induction. The ankle is internally rotated to get a mortise view which is checked on image intensifier ( Figure 1a). Under fluoroscopic guidance, a metal rod is placed over the ankle and adjusted so that it aligns with the centre of talus. It is further adjusted to align with the centre of lower third of tibia that is visible under the image intensifier (Figure 1a). The position is maintained and a permanent marker is used to draw a straight line along this rod (Figure 1b). The painting and draping ensues in a standard fashion. In case the mark fades after scrubbing, it is further reinforced with a sterile marker pen and covered with ioban to secure the mark (Figure 1c).
 Figure 1: a): C-arm image of adjusting the marker at the centre; b): Marking of centre of ankle under image intensifier; c): Intra-operative image of leg covered
with Ioaban with visible marking.
Figure 1: a): C-arm image of adjusting the marker at the centre; b): Marking of centre of ankle under image intensifier; c): Intra-operative image of leg covered
with Ioaban with visible marking.After this the surgery proceeds along the routine steps using a midline skin incision and a medial parapatellar arthrotomy. The cruciate ligaments and menisci are cut and the tibia is subluxated anteriorly. The extra medullary jig is now placed so that the central rod aligns with the skin marking (Figure 2). The position of jig in AP plane and the height is adjusted as felt appropriate by the surgeon. The tibia is cut, measured and the alignment checked with rod extender over the tibial base plate. Rest of the surgical steps are carried out in a standard conventional manner.
 Figure 2: Tibia cutting jig aligns with marker
Figure 2: Tibia cutting jig aligns with markerThe above technique was used in 30 patients (9 males) who were operated by two surgeons during a period of 6 months from January 2022 to June 2022. Only primary knees with varus upto 15 degrees as measured on pre operative X-rays, were included. Patients with tibial bowing were excluded. The average BMI was 28. The average surgical time was 75 minutes. All cases were operated using the proposed technique for ankle centre location and the mean time required to mark the centre was 1.26 minutes. 3.2 C-Arm shoots were required on an average in each case.
Postoperatively, implant position was checked on anteroposterior X-ray of the operated knee and a full length Antero-Posterior X-ray of the tibia with limb in neutral rotation and patella facing anteriorly. Measurements were done electronically as well as physically on computer screen and X-rays respectively. A straight line was drawn from the centre of the ankle to the centre of the tibial base plate. The angle between this line and the line drawn parallel to the tibial base plate was measured (Figure 3). 21 of the 30 cases had good placement of the implant within 1 degree of ideal alignment and 9 within 2 degrees (Figure 4).
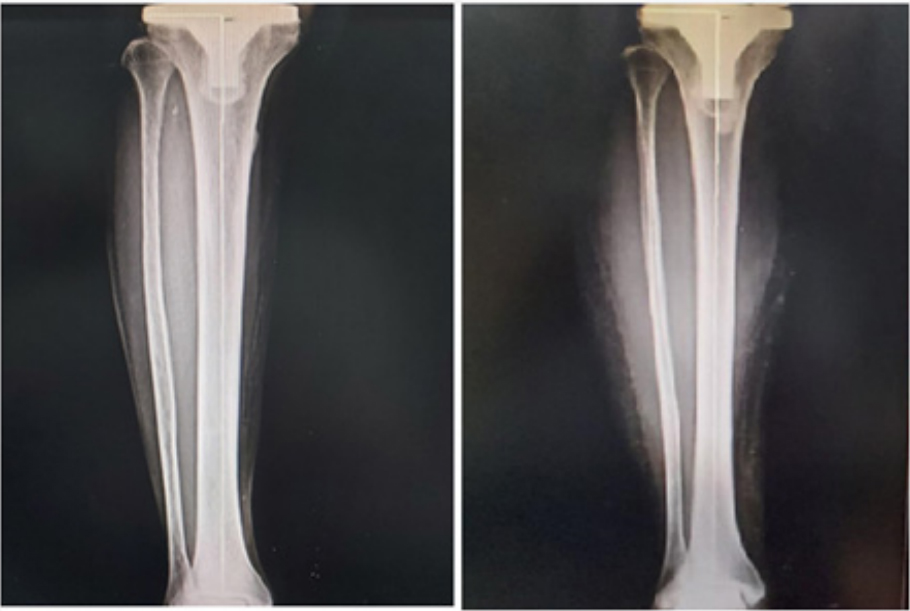 Figure 3: Measurement of tibial alignment on computer software
Figure 3: Measurement of tibial alignment on computer software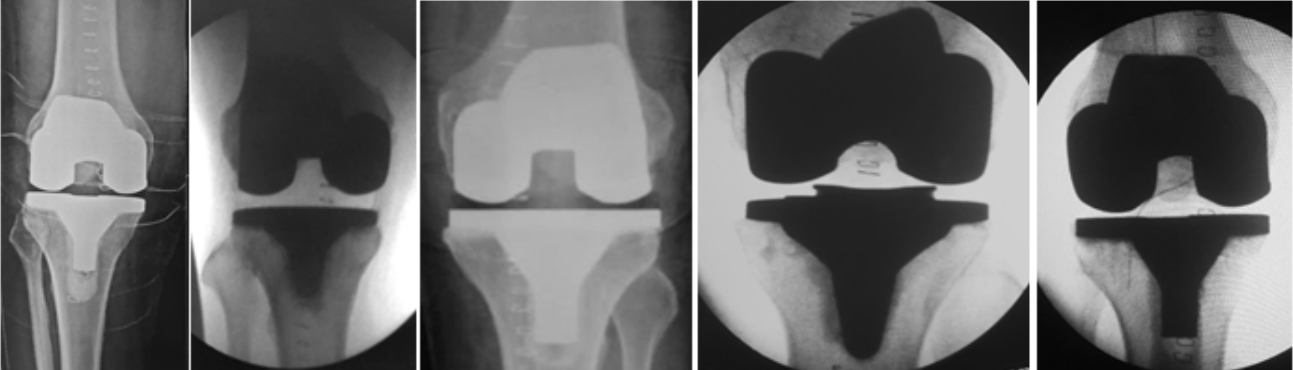 Figure 4: Post-operative radiological images of cases operated using this technique
Figure 4: Post-operative radiological images of cases operated using this techniqueMalalignment in knee replacement has been correlated with implant wear, loosening and poor outcome [10]. Studies have shown that upto 10% of knee replacement surgeries have errors in tibial and femoral components exceeding more than 3 degrees. Also, malalignnment of more than 4 degrees has been reported in almost 8 % of tibial cuts by Peter et al. [11]. Berend et al., have shown that knee failure rate can increase upto 17 times if varus is more than 3 degrees [12]. With an enormous increase in number of cases being done globally, this percentage translates into a very significant number of cases that may fail early. These findings suggest that tibial component alignment is one of the key steps in total knee replacement and error in initial surgical technique is most common cause of revision surgery.
A correct proximal tibia cut for a well aligned tibial component is achieved with the help of precise application of the cutting jigs. Extramedullary jigs used to make the proximal tibia cut have to be aligned parallel to the axis of the tibia and centred over the midpoint of talus, 3 mm medial to the centre of ankle joint. The current techniques available to locate centre of the ankle joint are dictated by the surgeons clinical judgement as it is estimated by palpating the medial and lateral malleoli. Using extra medullary guides, it has been reported that only 70% to 80% of patients have the tibial component placement with 3 degrees [13].
Several methods have been proposed by various authors to locate the centre of the ankle joint. Broadly, they are classified as anatomical and kinematic. In the former, the surgeon relies on digital palpation of medial and lateral malleolus and judging a centre based on the transmalleolar axis [14]. In the later method, the surgeon moves the foot and ankle in a defined motion and an algorithm estimates the centre. The study concluded that anatomical methods were more repeatable [6].
The surgeons best estimate of the centre of ankle in frontal plane using a digitised vector was investigated by Krackow et al. [15]. Nofrini et al., digitised tibialis anterior tendon onto the transmalleolar axis and examined the ability to locate the midpoint between the most distal apexes of the malleoli [5]. Rajadhyaksha et al., on an MRI study found encouraging results with the use of tibialis anterior tendon as a reliable distal anatomical landmark [7]. On the contrary, Schneider et al reported that the average distance between the lateral border of Tibialis anterior and centre of talus was more than 1 cm. They found EHL to be a more reliable landmark [8].
Ikeuchi et al., proposed use of multiple anatomical landmarks to reduce errors in component alignment. They advocated use of the dorsalis pedis artery and the anterior tibial crest rather than using only the intermalleolar centre to achieve accurate coronal alignment of the tibial component [9]. Inspite of all the literature available, at present there is no consensus on the best method.
Though mechanical instrumentation system keeps on upgrading continuously, they still rely on the operating surgeons visual inspection and clinical judgment. Even computer navigation relies on accurate feeding of anatomical reference points which is done manually. Thus the centre of ankle estimation remains more or less similar in both navigated and non navigated techniques with an inter observer variability. This variability may be compounded further in obese patients with excessive fat and hefty soft tissue cover.
Any technique being used for the same can be significant if it is precise, accurate, repeatable, objective and less time consuming [6]. Sobti et al located the ankle centre under image intensifier using ECG leads and reported better alignment postoperatively [16]. Similarly, the technique used in the present study vitally assisted in reducing the assumption and subjectivity involved in locating the centre of the ankle. This surgical step allowed good placement of tibial component and improve overall alignment. Since many variables affect the surgical outcome, an overall good result cannot be solely attributed to this surgical step. However, we believe it adds value to achieving the final aim of a good implant position. We admit that a comparative study with a longer follow up will make this research more effective.
The primary objective of knee replacement is to restore mechanical alignment. Identifying the mechanical axis begins with locating the centre of ankle joint. We propose a new method to achieve the same using C-Arm guidance that can provide reliable information to the operating surgeon to make better intra operative decisions. The technique has a dual advantage as it gives a better estimate of not only the centre of the ankle but also the centre of the distal tibial mechanical axis.
I wish to convey that all authors have taken the consent of hospital ethics committee. All patients who were enrolled in the study were made aware of the study design. The confidentiality of the patient has been maintained.
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.

