 Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY
Journal of Medical Research and Surgery
PROVIDES A UNIQUE PLATFORM TO PUBLISH ORIGINAL RESEARCH AND REMODEL THE KNOWLEDGE IN THE AREA OF MEDICAL AND SURGERY



 Indexed Articles
Indexed ArticlesSelect your language of interest to view the total content in your interested language
Gerald C. Hsu*
EclaireMD Foundation, USA
Correspondence to: Gerald C. Hsu, EclaireMD Foundation, USA; E-mail: g.hsu@eclairemd.com
Received date: April 13, 2020; Accepted date: April 24, 2020; Published date: May 01, 2020
Citation: Hsu GC (2020) A Case Study of the Relationship Between Weight and Glucose Using Math-Physical Medicine. J Med Res Surg. 1(3): pp. 1-6.
Copyright: © 2020 Hsu GC. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use,
distribution and reproduction in any medium, provided the original author and source are credited.
The article is a case study of the Relationship between Weight and Glucose Using Math-Physical Medicine. For 2,245 days, the author, who has Type 2 Diabetes (T2D) for approximately twenty years, collected and processed about 1.5 million biomedical data regarding his health and lifestyle conditions, including 13,470 data for weight and glucose. There are approximately 20 influential factors (5 for FPG and 15 for PPG) for determining glucose levels. Also, the author has collected a complete set of PPG data for 1,075 days with 3,225 meals. In this article, the author will discuss the specific relationship between weight and glucose along with FPG and PPG. In conclusion, Based on the case study of this overweight but not obese (BMI < 30) patient’s data analyses, the results show that most of his FPG data (~93%) are almost directly proportional to his weight change according to a “fixed” slope.
Type 2 Diabetes, PPG, FPG, Weight and Glucose
For 2,245 days (1/1/2012 to 2/24/2018), the author, who has type 2 diabetes (T2D) for approximately twenty years, collected and processed about 1.5 million biomedical data regarding his health and lifestyle conditions, including 13,470 data for weight and glucose. This dataset includes medication, weight (measured after waking up and at bedtime), Fasting Plasma Glucose (FPG), Postprandial Plasma Glucose (PPG) × 3 times a day, carbs and sugar intake, exercise, stress, sleep, travel, weather, glucose measurement time delay, water intake, bowel movement, and nighttime urination. All of the above factors are interrelated to a different degree since the human body is a highly nonlinear, dynamic, and sophisticated “analog” system.
Initially, the author utilized advanced mathematics and nonlinear dynamic engineering modeling concept to develop a set of governing equations about metabolism. He specifically applied the “finite element” structural engineering concept to convert a human “analog” system into a “digitized” system to get approximate solutions.
Before 2012, he did not keep a detailed daily record of his metabolic conditions and lifestyle data; however, after 1/1/2012, he has collected a complete set of his metabolic conditions and lifestyle statistics for 2,245 days (1/1/2012 to 2/24/2018). He continues to gather more information for future datasets [1]. As shown in Health Data Comparison (Table 1), during 2010, he weighed 210 lbs./95.5 kg (BMI 31, obese), his peak PPG was 380 mg/dL, average daily glucose was 280 mg/dL, and A1C above 10.0%. After 2012, he has kept a complete record. His weight fluctuated between 166.9 lbs./75.9 kg (BMI 24.65) and 193.8 lbs./88.1 kg (BMI 28.65); therefore, his average weight was 178 lbs./81 kg (BMI 26.28). His glucose level varied from 52 mg/dL to 280 mg/dL, average daily glucose was 126.5 mg/dL, and A1C around 6.5%
Table 1: Health data comparison between 2010 and 2017.| Health Exam Record | 2010 | 2017 |
|---|---|---|
| A1C (< 6.4%) | 10 | 6.1 |
| 90-days Average Glucose (< 120 mg/dL) | 279 | 11.3 |
| ACR (< 30) | 116.4 | 12.3 |
| Triglyceride (< 150) | 1161 | 67 |
| HDL (>40 | 24 | 48 |
| LDL (< 130) | 174 | 74 |
| Total Cholesterol (< 200) | 253 | 118 |
| BMI (< 25.0) | 31 | 24.7 |
| Weight (lbs.) | 210 | 167 |
| 3Waistline (Inches) | 44 | 34 |
The author started with a simple task of predicting tomorrow’s weight output from the previous 3-day input of weight, food quantity, and bowel movement. His weight prediction model has reached 99.9% linear accuracy. This weight prediction is the pre-processor for predicting FPG in the morning which leads to the A1C estimation.
Similar to glucose, weight is an output directly related to food and exercise, but it also can impact various chronic diseases. Weight is one of the outputs as well as one of the inputs of the complicated human metabolism system. Its main contribution factor includes food consumption quantity, food quality (fat, protein, carbs, & sugar), exercise amount, bowel and urine elimination, sleep quality, and emotional stress. Regarding glucose (i.e. A1C, daily average glucose, FPG, and PPG), it involves about 20 direct and indirect input factors with four major factors, including medication, weight, carbs/sugar, and exercise [2-4].
In 2015 - 2016, he spent ten months investigating FPG. Initially, he exhausted all avenues to find possible connecting factors, including a low correlation of ~0.9% between FPG and PPG. Although his 50-years of engineering training taught him to always look for relationships between input and output, he had to think “outside the box” to seek for a suitable answer. In the early morning of 3/17/2016, he had a dream about searching for the relationship among different body output categories. He then discovered that there was a high correlation of 84% between FPG and Weight.
The author has collected a complete set of PPG data for 1,075 days (since 6/1/2015) with 3,225 meals. This PPG-related data set, size of ~400,000 data, is only a small portion of his entire ~1.5 million data. Based on the knowledge he learned in the semiconductor industry, he initially utilized signal processing techniques to decompose a complicated glucose wave into many single-sourced waveforms. He then reintegrated them back to a predicted nonlinear glucose wave signal for comparison between measured vs. predicted glucose. Each single-sourced waveform is studied in detail for its intensity and importance level of contribution to glucose formation, and then further improved it via a “curve-fitting” trial and error engineering method which he learned from his defense work experience. He continuously compared these two sets of data and improved the prediction accuracy until it reached an extremely high linear accuracy while still maintaining a high correlation. High correlation means the trend of the predicted curve moving along with the measured curve like its “twin”.
Finally, he applied many statistical techniques to analyze these massive data, including linear accuracy, least-square means, correlation and determination coefficients, spatial analysis, time-series analysis, frequency-domain analysis via Fourier Transforms, etc. He has spent four years researching and interpreting the biomedical outcomes from his big data numerical simulation work. During this process, he developed his computational tools which utilized many techniques from the field of machine learning, auto-adjusting, Artificial Intelligence (AI), and optical physics [5-7].
There are approximately 20 influential factors (5 for FPG and 15 for PPG) for determining glucose levels. For FPG, weight is the most dominant factor contributing 80% to 90% to its value. In the time-series analysis, results shown between weight and FPG (Figure 1). indicated a high correlation of 84%. In the spatial analysis diagram of BMI vs. FPG (without time factor), there is a “quasi-linear” equation existing between two coordinates of BMI and FPG. The stochastic (random) distribution of data has two clear “relationship concentration bands” stretched from the lower left corner toward the upper right corner. In the spatial analysis, results show ~93% of the total collected data are covered by a +/- 20% band. This “relationship band” stretched from point A (24.5, 95) to point B (27.2, 150) on a spatial map with coordinates of x=BMI, y=glucose.
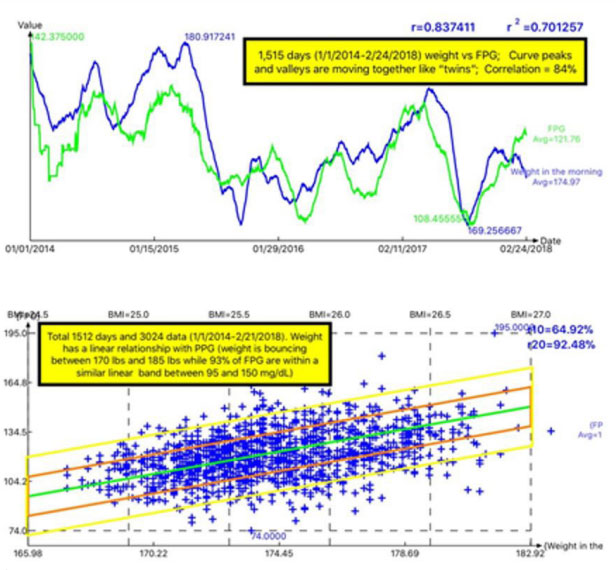 Figure 1: Relationship between Weight and FPG using time-series and spatial analysi.
Figure 1: Relationship between Weight and FPG using time-series and spatial analysi.The author has collected a complete set of PPG data including his lifestyle data for 2,245 days (1/1/2012 to 2/24/2018). However, he started to analyze and collect detailed data of his meals and exercise since 6/1/2015. In the past three years for PPG, he continuously explored and added all of the probable influential factors into the formation of the human PPG signal. His purpose was to improve the predicted PPG waveform’s contents and accuracy while maintaining a high correlation with the measured PPG waveform [8].
For example, by the fall of 2016, the accuracy of his predicted PPG reached ~95%; however, in September of 2017, he identified that weather temperature had an impact on glucose value. Therefore, he selected 2 years (6/2015 to 7/2017) to examine his past travel schedule in detail. During the past seven years, the author traveled via air, an average of every 13days, and entered each day’s local ambient temperature of the city where he stayed. In this way, he was able to generate a new temperature sub-waveform which brought the accuracy of PPG prediction from 95% to 98%.
Another factor was that his glucose value was quite high when he was sick with two different flu viruses for 45 days at the end of 2017. After that health experience, he further enhanced his prediction model with the inclusion of the “physical sickness” factor which finally brought the accuracy of PPG prediction from 98% to 99.8%.
During his research on glucose prediction, unlike the case for FPG, he has proven that weight is no longer the dominating factor of PPG. Instead, the combined carbs and sugar intake with post-meal exercise occupied about 81% of the contribution and importance level of PPG. Weather generated ambient temperature counted approximately 10% and the other 12 combined factors were about 9%. In the time-series analysis, between weight and PPG (Figure 2).
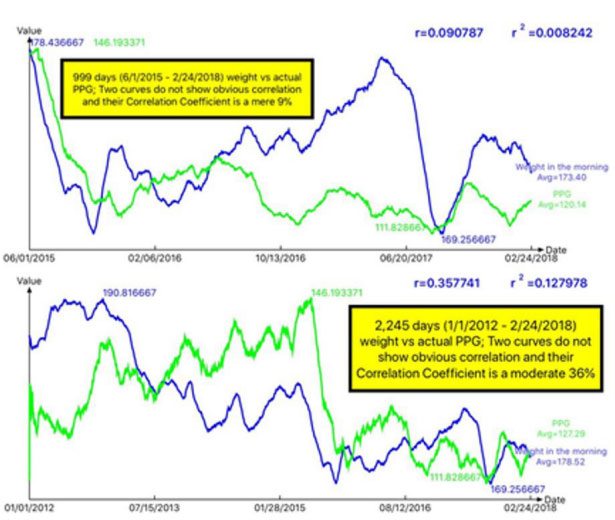 Figure 2: Correlation between Weight and PPG using two different windows of collected data (9% for 999 days vs. 36% for 2,245 days).
Figure 2: Correlation between Weight and PPG using two different windows of collected data (9% for 999 days vs. 36% for 2,245 days).their correlation is between a low 9% to a moderate 36% (depending on the window selection of collected data). In the spatial analysis, results also show 86% of the total collected data covered by a +/- 20% of a “horizontal” band which is centered around a“constant” PPG value of 127 mg/dL (Figure 3).
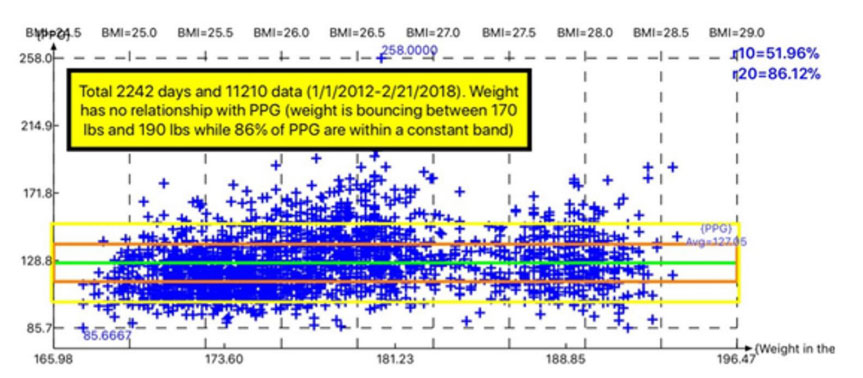 Figure 3:PPG data maintain within a constant band regardless of weight change.
Figure 3:PPG data maintain within a constant band regardless of weight change.Furthermore, in the stacking spatial analysis graphics over six years from January of 2012 through February of 2018 demonstrate that his BMI moved toward the lower range, while his PPG “data cluster” (cloud image) kept at a relatively constant level around 127 mg/dL (Figure 4).
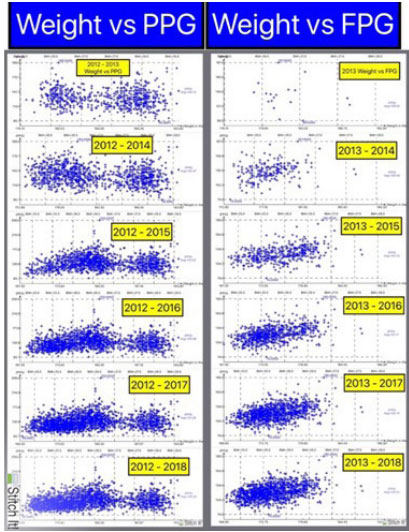 Figure 4:Glucose “data cluster” between Weight Reduction vs. Constant
PPG and Weight Change vs. FPG Change from 2012 to 2018 (annually accumulated glucose data).
Figure 4:Glucose “data cluster” between Weight Reduction vs. Constant
PPG and Weight Change vs. FPG Change from 2012 to 2018 (annually accumulated glucose data).This means that PPG kept at a constant range regardless of his weight reduction. In contrast, his FPG “data cluster” or cloud moved from the upper right corner toward the lowerleft corner which means his FPG level became lower when his weight dropped (Figures 5,6).
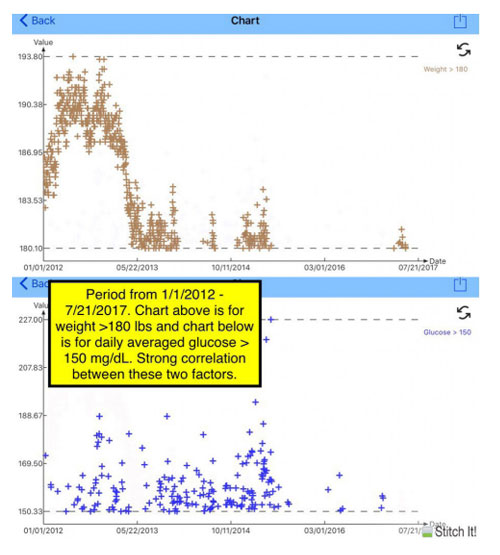 Figure 5:Weight over 180 lbs. and daily average glucose over 160 mg/dL.
Figure 5:Weight over 180 lbs. and daily average glucose over 160 mg/dL.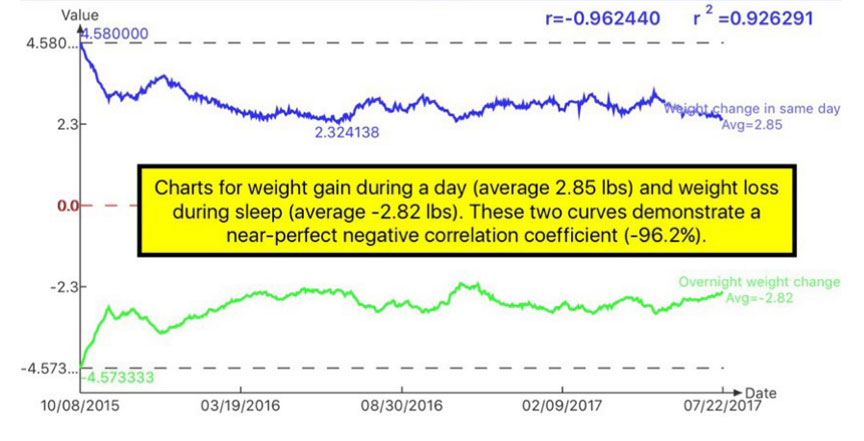 Figure 6:Weight Gain between morning and bedtime of the same day, Weight Loss between the previous day’s bedtime and this day’s morning.
Figure 6:Weight Gain between morning and bedtime of the same day, Weight Loss between the previous day’s bedtime and this day’s morning.Based on the case study of this overweight but not obese (BMI < 30) patient’s data analyses, the results show that most of his FPG data (~93%) are almost directly proportional to his weight change according to a “fixed” slope. However, most of his PPG data (86%) have been kept at a constant level of 127 mg/dL within the range of 102 mg/dL to 152 mg/dL. The PPG amplitude changes within this range are mostly determined by both carbs/sugar intake and post-meal exercise, but not directly by the weight itself [9].
In summary, both FPG and Weight have no relationship and influence on PPG. On the other hand, Weight is the primary factor of FPG. Weight is directly proportional to the total “quantity” of food consumption (the total amount of protein, fat, carbs, sugar, fiber, etc.), while PPG is directly related to food “quality”, specifically the intake amount of carbs and sugar. Of course, a person who eats a large quantity of food will likely take in more carbs and sugar. However, a knowledgeable and well-disciplined T2D patient can control both the quantity and quality of food intake. It should be noted that the above conclusion should be re-verified for extreme cases of lightweight and obese patients. Nevertheless, a strict weightreduction will be an effective and direct way for obese patients to put their glucose values (both FPG and PPG) under control [10].
First and foremost, I wish to express my sincere appreciation to a very important person in my life, Professor Norman Jones at MIT. Not only did he allow me to study at MIT, but he also trained me extensively on how to solve problems and conduct scientific research.
I would also like to thank Professor James Andrews at the University of Iowa. He helped and supported me tremendously when I first came to the United States. He believed in me and prepared me to build my engineering foundation during my undergraduate and master’s degree work.
There are no conflicts of interest

