 Journal of Clinical and Biomedical Investigation
PROVIDES A UNIQUE PLATFORM COVERING SCIENTIFIC KNOWLEDGE IN BIOMEDICAL SCIENCES AND CLINICAL RESEARCH
Journal of Clinical and Biomedical Investigation
PROVIDES A UNIQUE PLATFORM COVERING SCIENTIFIC KNOWLEDGE IN BIOMEDICAL SCIENCES AND CLINICAL RESEARCH
Journal of Clinical and Biomedical Investigation
PROVIDES A UNIQUE PLATFORM COVERING SCIENTIFIC KNOWLEDGE IN BIOMEDICAL SCIENCES AND CLINICAL RESEARCH
Journal of Clinical and Biomedical Investigation
PROVIDES A UNIQUE PLATFORM COVERING SCIENTIFIC KNOWLEDGE IN BIOMEDICAL SCIENCES AND CLINICAL RESEARCH
Anubha Bajaj *
Consultant Histopathologist, AB Diagnostics, India.
Correspondence to: Anubha Bajaj, Consultant Histopathologist, AB Diagnostics, India.
Received date: January 13, 2023; Accepted date: January 23, 2023; Published date: January 28, 2023
Citation: Bajaj A. The Cankerous Seepage-Adenocarcinoma Anal Canal: A Short Communication . J Clin Biomed Invest. 2023;3(1): 4-5. doi:
10.52916/jcbi234022
Copyright: ©2023 Bajaj A. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits
unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Adenocarcinoma of anal canal is an infrequently discerned malignant neoplasm demonstrating configuration of glandular articulations. The neoplasm primarily incriminates anal canal or arises within deep seated soft tissues adjacent to the anal canal. Adenocarcinoma of anal canal preponderantly emerging from extra-mucosal sites is additionally designated as perianal adenocarcinoma or perianal gland adenocarcinoma. Tumefaction necessitates distinction from adenocarcinoma secondarily involving anus as encountered with rectal carcinoma. Rectal adenocarcinoma with inferior tumour extension does not categorize as adenocarcinoma of anal canal. Notwithstanding, adenocarcinoma extending inferiorly from rectum is denominated as rectal adenocarcinoma. Adenocarcinoma of anal canal constitutes an estimated 5% of anorectal malignancies. The neoplasm is commonly discerned amongst elderly subjects or within seventh decade. A male predominance is observed. As categorized, adenocarcinoma of anal canal singularly incriminates the anus. Adenocarcinoma of anal canal may arise from anal glands, congenital anorectal duplications or occur along an anal fistula tract [1,2].
Exceptionally, the neoplasm may demonstrate accumulated Deoxyribonucleic Acid (DNA) of high risk subtypes of Human Papilloma Virus (HPV) as HPV18 DNA. Nevertheless, neoplastic cells may be devoid of HPV 16 DNA. Thus, infrequently occurring instances concurrent to Human Papilloma Virus (HPV) infection appear immune reactive to p16 [1,2]. Additionally, adenocarcinoma of anal canal possibly emerges due to association with chronic anal fistula, anal Crohn's disease or anal sexual intercourse. Adenocarcinoma of anal canal may represent within a fistula tract or appear as a vaginal cyst. The malignancy may be accompanied with history of occurrence of perianal fistula or anorectal abscess of extended duration or surgical intervention. The neoplasm demonstrates an indolent clinical course and is gradually progressive [2,3]. Upon gross examination, adenocarcinoma of anal canal appears as a nodular neoplasm with ulceration of superimposed mucosal surface. Tumour magnitude varies from ≥ 3 centimetres to 4 centimetres. Tumour is associated with deep seated infiltration into wall of anal canal along with proximal and distal dissemination into submucosa of distal rectum and proximal anus [3,4].
Upon microscopy, adenocarcinoma of anal canal is comprised of disorderly dissemination of miniature neoplastic glands demonstrating scant mucin production. Neoplastic glands appear to invade wall of anorectal zone and delineate absence of an intraluminal component. Frequently, neoplastic glands appear as mucinous glands with >50% of tumour volume comprised of mucin secretion. Granulomatous reaction to accumulated mucin may ensue. Neoplastic glands may be imbued with melanin pigment possibly due to tumour cell phagocytosis of melanin arising from constituent melanocytes. Adenocarcinoma of anal canal represents with distinctive subtypes as ~colorectal subtype which originates within layering columnar epithelium or mucosa and may be accompanied by a residual mucosal lesion. Histologically, the subtype is identical to colorectal adenocarcinoma. ~extra-mucosal fistula or anal gland subtype is devoid of accompanying superimposed mucosal lesion. Tumefaction is predominantly associated with chronic anorectal fistula or may be associated with Crohn's disease. Majority of neoplasms appear as mucinous tumours and >50% of tumour volume exhibits a mucinous component. Foci of ductal or tubular differentiation may be observed. Adjacent cutaneous surface may demonstrate Paget’s disease. The malignant lesion may undergo ulceration [3,4].
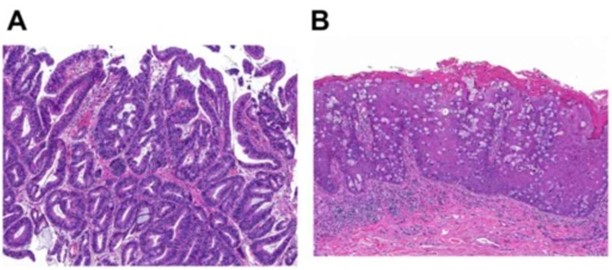 Figure 1: Adenocarcinoma anal canal demonstrating closely packed neoplastic glandular articulations with minimal mucin secretion and a layering of atypical columnar epithelial cells. Intervening stroma is desmoplastic. Adjacent stratified squamous epithelium exhibits pagetoid pattern of tumour dissemination [5].
Figure 1: Adenocarcinoma anal canal demonstrating closely packed neoplastic glandular articulations with minimal mucin secretion and a layering of atypical columnar epithelial cells. Intervening stroma is desmoplastic. Adjacent stratified squamous epithelium exhibits pagetoid pattern of tumour dissemination [5].
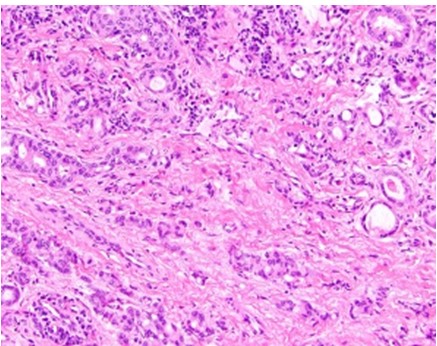 Figure 2: Adenocarcinoma anal canal delineating accumulated neoplastic glandular configurations with minimal mucin secretion and layering of atypical columnar epithelial cells. Circumscribing stroma is desmoplastic [6].
Figure 2: Adenocarcinoma anal canal delineating accumulated neoplastic glandular configurations with minimal mucin secretion and layering of atypical columnar epithelial cells. Circumscribing stroma is desmoplastic [6].Adenocarcinoma of anal canal is immune reactive to CK7 or MUC5AC. Adenocarcinoma of anal canal is immune non reactive to CK20, CDX2, and p16. Adenocarcinoma of anal canal requires segregation from neoplasms such as anal mucoepidermoid carcinoma, secondary involvement with rectal adenocarcinoma or squamous cell carcinoma [3,4].
Adenocarcinoma of anal carcinoma can be appropriately treated with standard therapeutic regimen as abdominoperineal surgical resection. Adjuvant chemotherapy and radiation therapy may be adopted to ameliorate prognostic outcomes. Adenocarcinoma of anal canal is associated with adverse prognostic outcomes. Generally, the malignant neoplasm is associated with advanced tumour stage, significant regional lymph node metastasis and enhanced histologic grade of the neoplasm [3,4].

