 Journal of Clinical and Biomedical Investigation
PROVIDES A UNIQUE PLATFORM COVERING SCIENTIFIC KNOWLEDGE IN BIOMEDICAL SCIENCES AND CLINICAL RESEARCH
Journal of Clinical and Biomedical Investigation
PROVIDES A UNIQUE PLATFORM COVERING SCIENTIFIC KNOWLEDGE IN BIOMEDICAL SCIENCES AND CLINICAL RESEARCH
Journal of Clinical and Biomedical Investigation
PROVIDES A UNIQUE PLATFORM COVERING SCIENTIFIC KNOWLEDGE IN BIOMEDICAL SCIENCES AND CLINICAL RESEARCH
Journal of Clinical and Biomedical Investigation
PROVIDES A UNIQUE PLATFORM COVERING SCIENTIFIC KNOWLEDGE IN BIOMEDICAL SCIENCES AND CLINICAL RESEARCH
Kevin Lee*, Michael J. Herr, Jerry W. Jones
University of Tennessee Health Science Center, Memphis TN, USA
Correspondence to: Kevin Lee, University of Tennessee Health Science Center, Memphis TN, USA
Received date: February 07, 2022; Accepted date: February 25, 2022; Published date: March 03, 2022
Citation: Lee K, Herr MJ, Jones J (2022) Safety and Efficacy of Rescue Nerve Blocks. J Clin Biomed Invest 2(1): pp. 9-14. doi:
10.52916/jcbi224012
Copyright: ©2022 Lee K, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits
unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Background: The overall incidence of complications following peripheral nerve blocks is very low. Peripheral nerve blocks performed under ultrasound guidance are widely thought to present a lower risk to direct needle trauma than paresthesia and nerve stimulation techniques and have been shown to decrease opioid consumption by providing analgesia directly to the site of injury. Currently, when a nerve block fails altogether or provides inadequate analgesia, pain and opioid consumption increases which in turn decrease patient satisfaction and increases healthcare costs. Concerns remain whether the benefits of opioid reduction outweigh the risk of inadvertent needle trauma and other potential complications when performing a nerve block replacement, or ‘rescue block’.
Objective: Examine whether performing a rescue peripheral nerve block provides adequate analgesia to elicit a decrease in opioid consumption. Analyze the incidence of nerve injury following ultrasound-guided ‘rescue’ continuous peripheral nerve blocks.
Methods: Data was retrospectively collected from patient electronic medical records from a Level 1 academic Trauma Center at Regional One Hospital in Memphis, Tennessee from March 1, 2019 to May 31 2021. Inclusion criteria was patients over 18 years of age at time of admission who received consecutive continuous peripheral nerve blocks in the same relative location during a time when the peripheral nerves were likely partially or fully anesthetized (a rescue block). The primary outcomes assessed were 24-hour opioid consumption prior to the initial continuous nerve block, just prior to and after the ‘rescue’ block. Adverse outcomes potentially due to performing a ‘rescue’ block were also examined, including direct needle trauma, nerve injury related to extended exposure to local anesthetics, and local anesthetic systemic toxicity. Types of nerve blocks performed, range and median number of catheter days, and reason for rescue block was recorded for all patients. All available electronic healthcare records were reviewed to identify potential injury. Nerve blocks were categorized into low and high risk for direct needle trauma based on the incidence of needle trauma found in the literature and whether the needle was required to be adjacent to a discrete nerve or nerve bundle in order to perform the procedure.
Results: 55 patients were examined. Of the 55 patients, 5 had multiple locations both blocked and rescued, bringing the total rescue procedures examined up to 60. Additionally, 10 patients had their rescue site re-blocked multiple times due to either multiple surgeries, displacements, or duration of analgesia required bringing the total number of rescue blocks performed to 74. Patients that received an initial continuous peripheral nerve block consumed significantly fewer opioids during the 24 hour period following the block than the 24-hour period before the block was performed (P=0.033). Continuous peripheral nerve blocks (CNPB) were replaced or ‘rescued’ for two general reasons: Failed or Inadequate Analgesia (21) and to Extend the Utilization of adequately functioning infusions (35). Once a rescue nerve block was performed, there was no significant change in opioid consumption than after the original block (P=0.64). Of the 60 rescue blocks that were recorded, there were 0 adverse outcomes that were attributed to the rescue block procedure.
Conclusion: Following failed CPNB or when performed to extend the utilization of CPNB infusions, ultrasound-guided ’rescue’ nerve blocks result in reduced opioid consumption to a similar level as the initial peripheral nerve block, and do not result in an increase in the incidence direct needle trauma. Given the relatively low incidence of needle trauma and other nerve block-related complications, larger studies are needed to confirm these initial findings, however, ultrasound provides numerous clinical strategies that can be employed that may reduce the incidence of direct needle trauma compared with traditional nerve localization techniques.
Regional anesthesia, Continuous Peripheral Nerve Blocks (CNPB), Ultrasound, Acute Pain Service (APS), Local Anesthetic Systemic Toxicity (LAST)
The benefits of regional anesthesia for acute pain control have been well documented to include decreased opioid consumption, increased patient satisfaction, and decreased cost for both hospital and patient [1-4]. While many factors contribute to these findings, in order to examine the benefits of peripheral nerve blocks, a successful nerve block must first be defined. In a successful nerve block, the interests of the patient, anesthesiologist, and hospital administration must be aligned [5]. The most commonly cited definitions of block success include factors such as a block that has partial or complete sensory or motor block, no conversion to General Anesthesia (GA), and performed within a designated time period [5].
In order to achieve a successful peripheral nerve block, the correct nerve or plexus must be identified, and the needle must be placed sufficiently close to the nerve to ensure local anesthetic (LA) is surrounding the nerve [6]. Ultrasound (US), unlike other established regional anesthesia techniques, can be by used to consistently perform all three of these criteria simultaneously [6]. The benefits of using US in regional anesthesia have been shown as faster analgesic onset, shorter procedure duration, lower dose of LA used, decreased onset of Local Anesthetic Systemic Toxicity (LAST), and lower incidence of direct needle trauma [5-10].
However, not every nerve block performed meets the criteria for a successful block. When nerve blocks fail or are ineffective, there is usually an increased dependence on opioids or a forced a conversion to GA [5, 11]. Failed nerve blocks can be stratified as complete or partial failures. A complete failure is when a block shows no evidence of sensory or motor blockade in the desired location [12]. A partial failure does show evidence of sensory or motor blockade, but with inadequate or incomplete analgesia [12].
In many ways, performing a nerve block at a previously failed Regional Anesthesia (RA) site can be compared with the risks of performing RA while a patient is heavily sedated or under GA. In both cases, one cannot rely on patient feedback to determine needle positioning [13, 14].
Ultrasound has been shown as an effective tool for performing nerve blocks under GA or heavily sedated patients [13, 14]. In the same way, US can be used to perform a rescue nerve block at a site where LA has been previously administered. These differences over previous nerve localization techniques along with new appreciation of the negative consequences of opioids may represent a much different risk benefit ratio to perform rescue blocks in previous eras. This study examined the use of ultrasound in performing rescue nerve blocks at locations where previous RA has been administered and failed to provide sufficient analgesia.
Institutional review board approval was obtained through University of Tennessee Health Science Center before the study began (IRB acceptance 21-08120-XP). Patients were selected from Regional One Health, a 337 bed level 1 trauma center. Inclusion criteria consisted of being over the age of 18 at time of admission and having at least one failed nerve block that was replaced during a single in-patient visit. The study covered a 38-month period from March of 2019 through May 2021. Opioid use was defined as drugs including: codeine, fentanyl, meperidine, methadone, morphine, hydromorphone, propoxyphene, or oxycodone. Once selected, patient data was de-identified and collected into a password protected Excel sheet for analysis.
All peripheral nerve blocks utilized were grouped into high risk (Brachial plexus, Saphenous, Lateral Femoral Cutaneous, Popliteal Sciatic) and low risk (ESP, Subpectoral, Serratus, Rectus Sheath, Subgluteal Sciatic, Femoral, and Fascia Iliaca) categories based on needle proximity to nerve needed for effective analgesia. All opioids consumed were converted to Morphine Milli- Equivalents (MMEs) based on standard conversion ratios. To determine if a nerve block was working, assessment of Acute Pain Service (APS) progress notes for loss of temperature sensation or confirmed numbness and loss of motor strength when applicable was collected. A report of confirmed loss of sensation or numbness correlated to a confirmed working nerve block, while denial of loss of temperature sensation was inferred as a block that was not confirmed to be working. In situations where a physical exam was not reliable such as amputations, opioid consumption and reported patient pain sensations were examined to determine if the nerve block was effective.
A sample size of 55 patients was identified, and 5 of the patients had more than one site both blocked and rescued making the total rescue blocks performed 60. Data was imported to Tableau for grouping, Excel was used for statistical analysis, and GraphPad was used to generate figures.
Patient’s characteristics are shown in Table 1. Of the 55 patients examined, 5 had more than one site both blocked and rescued so these were inc luded to bring the total rescue blocks performed up to 60. Additionally, 10 patients had their rescue site re-blocked multiple times due to either multiple surgeries, displacements, or duration of analgesia required bringing the total number of rescue blocks performed to 74. The incidence of factors known to be associated with an increased risk of nerve injury or complaints of ongoing neurologic symptoms such as morbid obesity, diabetes mellitus, and pre-existing neuropathy were collected.
n |
|
| Mean Age in years (range) | 45.7 (18-78) |
| Mean Weight in kg (sd) | 93.8 (30.4) |
| Male/female | 36/19 |
| Morbid Obesity, n (%) | 13 (24%) |
| Diabetes Mellitus, n(%) | 9 (16%) |
| Pre-existing Neurological Disorder, n (%) | 5 (9%) |
Table 2 shows the number of blocks performed from either the high risk or low risk categories as well as the average time to perform the initial block and the rescue block. There was no significant difference in time to perform block based on if it was the initial block or rescue block (P=0.633). Additionally there was no significant difference in time to perform block whether it was a high or low risk block (P=0.87).
| n | Time to Perform Initial Block (min) | Time to Perform Rescue (min) | Average Number of Days Block in Place | Average Number of Days Rescue in Place | Range of Days | |
| High Risk | 31 | 9.7 | 11.1 | 3.9 | 8.5 | 0-27 |
| Brachial Plexus | 10 | 11.2 | 9.8 | 5.3 | 8.3 | 43101 |
| Lateral Femoral Cutaneous | 4 | 11.5 | 9.3 | 5.7 | 5.5 | 44835 |
| Popliteal Sciatic | 16 | 11.6 | 12.9 | 4.7 | 7.2 | 0-27 |
| Saphenous | 1 | 7 | 13 | 0 | 13 | 0-13 |
| Low Risk | 29 | 14.5 | 7.9 | 4.9 | 9.9 | 0-27 |
| ESP | 13 | 13.3 | 12.6 | 4.4 | 7.5 | 43132 |
| Femoral | 1 | 12 | 9 | 2 | 27 | 46419 |
| Fascia Iliaca | 5 | 16.4 | 9.6 | 4.4 | 7.2 | 0-13 |
| Serratus | 5 | 13 | 8.6 | 8.6 | 4.2 | 42767 |
| Subgluteal Sciatic | 3 | 18 | 9.7 | 6 | 10.7 | 41640 |
| Subpectoral | 2 | 23.5 | 10.5 | 4 | 3 | 44654 |
Both the original nerve block and rescue block procedure notes were checked for noted difficulty during the procedure. There were only 3 (5%) patients that had both a complex original block and rescue block, while there were 12 and 13 patients that had noted complexity in the original and rescue blocks, respectively. The majority of the complexity noted in both original and rescue blocks was due to either subcutaneous air present making visibility difficult or difficult patient positioning due to existing injury.
The reason for block replacement was tracked to determine the reason a rescue block was needed. Most causes were due to catheter removal either accidental or for surgery. There was no significant correlation between the type of nerve block performed and the reason a rescue was needed (r= 0.48, P=0.27). Table 3 shows the reasons for replacement based on if the initial block was a high or low risk site.
| Reason For Nerve Block Replacement | High Risk | Low Risk |
| Extended Utilazation | 22 | 13 |
| Catheter dislodged or accidently removed | 6 | 6 |
| Standard Replacement | 6 | 1 |
| Surgery | 10 | 6 |
| Failed or Inadequate | 7 | 14 |
| Incomplete or unsuccessful block reports of pain | 6 | 13 |
| Problem with dressing | 1 | 1 |
| Other | 2 | 2 |
All peripheral nerve blocks performed were monitored to confirm either motor or sensory blockade was sufficient. This data was collected and shown in Figure 1. When bandages or dressings interfered with a proper physical exam of the blocked area, this is listed as unable to assess. Only 3 patients denied a decrease in temperature sensations on exam, but all three of these patients reported a decrease in pain sensation after initial block, as well as decreasing their opioid consumption after initial block. Of the 23 patients where the block was unable to be assessed by physical exam, 6 reported an increase in pain between the initial block and pre- rescue physical exam. Figure 2 shows the number of blocks grouped into complete failure, partially functioning, or fully functioning based on pre-rescue exam findings. Complete failure was defined as denial of decreased temperature sensation, increase of pain sensation, and increase in opioid consumption. A fully functioning block was defined as confirmed loss of temperature or motor sensation on physical exam, or when unable to assess, both decreased opioid consumption and decrease in pain sensations. The remainder were grouped into partially functioning.
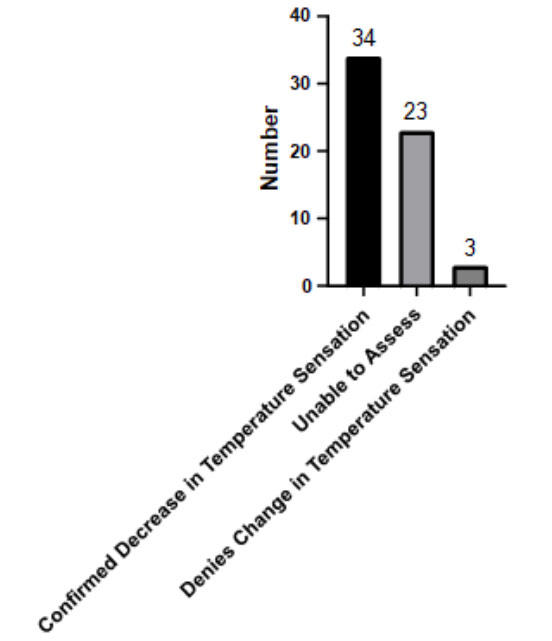 Figure 1: Confirmation of nerve blockade
Figure 1: Confirmation of nerve blockade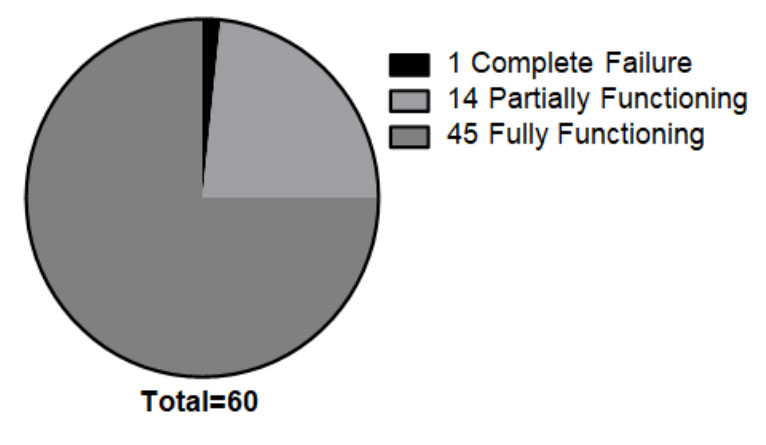 Figure 2:Type of failure
Figure 2:Type of failureOpioid consumption was examined before initial block was performed, after initial block, before rescue block, and after rescue block. Figure 3 shows overall opioid consumption by time relative to block performed. There was a significant decrease in average opioid consumption before and immediately after initial block (P=0.033), as well as a significant difference between the pre- block average and the post-rescue average (P=0.027). There was no significant difference between average opioid consumption immediately after initial block and post-rescue (P=0.64). Additionally, 24 (40%) patients reached zero opioid consumption an average of 2.9 (2.2 sd) days after the initial block as shown in Figure 4.
 Figure 3: Opioid consumption
Figure 3: Opioid consumption 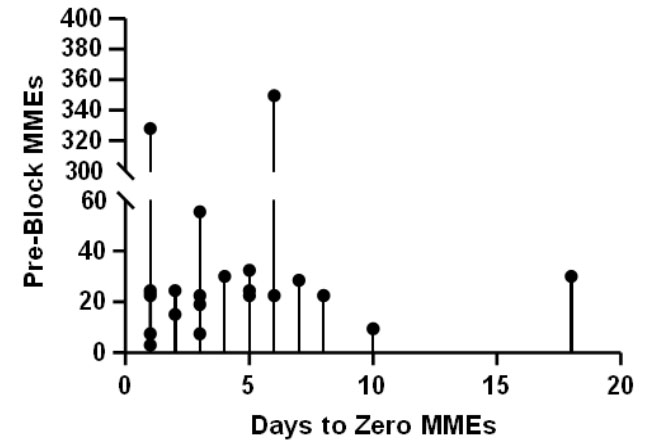 Figure 4: Days until zero opioid consumption following initial block
Figure 4: Days until zero opioid consumption following initial blockAdditionally, subjective data was collected and shown in Figure 5. There were 34 (56%) patients that reported a reduction in pain sensation after receiving the rescue block compared to 39 (65%) reporting reduction in pain after initial block.
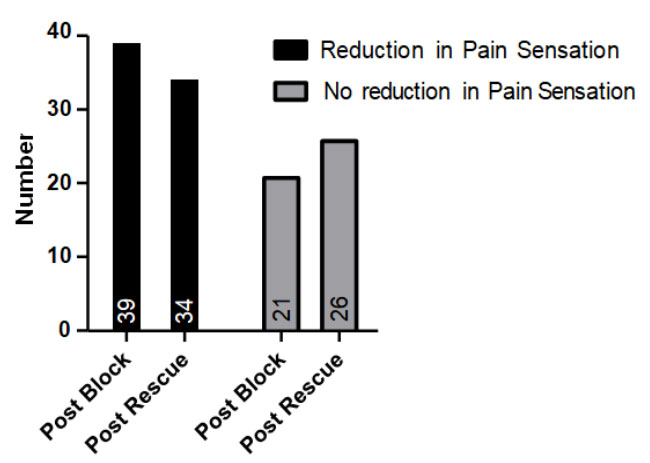 Figure 5: Reduction in pain reported
Figure 5: Reduction in pain reportedFollow up data was collected when present to determine if there was lasting damage to nerves that was attributable to the rescue nerve block and shown in Figure 6. There were 19 patients which no meaningful information could be found pertaining to their health or wellness after discharge.
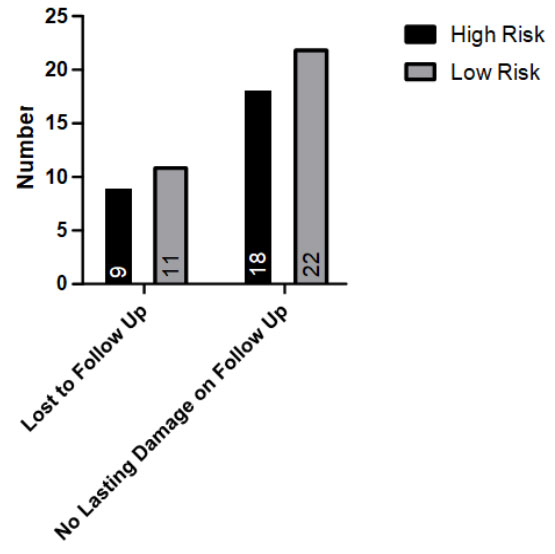 Figure 6: Follow up data
Figure 6: Follow up dataThroughout 60 recorded rescue blocks and 74 rescue blocks when including multiple replacements, there were no lasting complaints on follow-up that could be attributed to the nerve block performed.
The results showed that by replacing a failed nerve block, it brought opioid consumption back to the baseline immediately after initial block. This is supported by a similar number of patients that reported a reduction in pain sensation. The benefits of lowering opioid consumption by replacing a failed nerve block are: decreased hospital costs; decreased length of stay; lower 30-day readmission rate [1, 15]. Patient pain ratings are better controlled after both initial and rescue nerve blocks; this is both an indicator of block success and has been shown to correlate with patient satisfaction [5, 16].
While a successful nerve block can be defined as one that provides sensory or motor block without any conversion to General Anesthesia (GA), a failed block must be defined as one that does not [5]. Ultimately, this can be simplified to say that a failed nerve block is one that does not provide the appropriate amount of LA to the correct location. In this study, most of the rescues are due to removal of the continuous nerve block catheter due to either being in the surgical field or inadvertent removal. However, other methods of failure should be considered such as poor catheter dressing, change to more effective block location, incomplete analgesia, or poor catheter placement due to difficult sonoanatomy differences [12].
Before performing a rescue nerve block, it is important to assess why the initial block failed in order to determine the risk involved. If a continuous block is working well and either needs to be replaced for continuing analgesia, or becomes dislodged due to surgery or accident, this would present a higher risk replacement due to anesthetized nerves at site of rescue procedure and thus a partial failure. However out of 55 rescue blocks performed on partially failed initial blocks, 37 were confirmed to have no damage related to the rescue block, and the remaining 18 were lost to follow up. Alternatively, a block that failed due to incorrect placement, or other situations where there is no LA getting to the desired location would represent a complete block failure, and thus a much lower risk of direct needle trauma on rescue. Of the 5 rescue nerve blocks performed under low risk conditions, 3 were confirmed to have no damage related to the rescue block while the remaining 2 were lost to follow up.
While the risks of LAST, or direct needle trauma when performing a rescue nerve block are not to be understated, there are also ways to minimize this through considering some specific approaches to nerve block techniques. When performing certain nerve blocks such as femoral or fascia iliaca, a plane approach can be utilized such as with an Erector Spinae Plane (EPS) block, In this scenario, the needle is aimed away from the nerve toward surrounding fascia, therefore not requiring the needle to come in close proximity with the nerve [12]. Additionally, in many cases, the presence of previously administered LA can provide a hypoechoic cushion surrounding the nerve making visualization of the target nerve easier on US. Taking a planar approach to a fascia iliaca block provides a space to enter the perineurium, in the case of a popliteal sciatic nerve block, without touching the common peroneal and tibial nerves as shown in the image below (Figure 7).
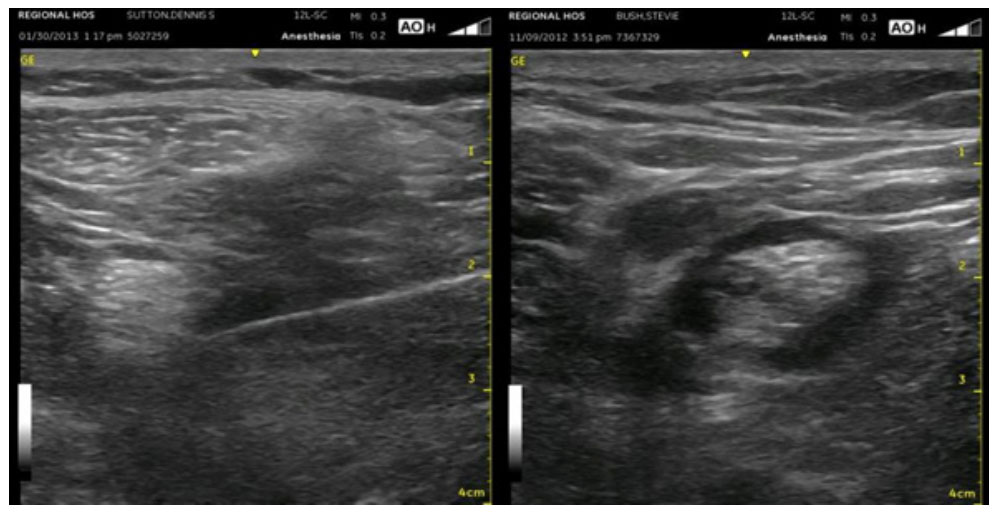 Figure 7: Hypoechoic cushion after LA injection
Figure 7: Hypoechoic cushion after LA injectionRescue blocks have been shown to be effective in keeping opioid consumption low, as well as improving patient pain sensations. While there are risks of performing rescue nerve blocks, 74 rescue procedures were performed with no related adverse outcomes.
There is no funding associated with this work.
This work is free of any conflicts of interest.

