 Journal of Clinical and Biomedical Investigation
PROVIDES A UNIQUE PLATFORM COVERING SCIENTIFIC KNOWLEDGE IN BIOMEDICAL SCIENCES AND CLINICAL RESEARCH
Journal of Clinical and Biomedical Investigation
PROVIDES A UNIQUE PLATFORM COVERING SCIENTIFIC KNOWLEDGE IN BIOMEDICAL SCIENCES AND CLINICAL RESEARCH
Journal of Clinical and Biomedical Investigation
PROVIDES A UNIQUE PLATFORM COVERING SCIENTIFIC KNOWLEDGE IN BIOMEDICAL SCIENCES AND CLINICAL RESEARCH
Journal of Clinical and Biomedical Investigation
PROVIDES A UNIQUE PLATFORM COVERING SCIENTIFIC KNOWLEDGE IN BIOMEDICAL SCIENCES AND CLINICAL RESEARCH
Christopher D. Castelow1* , Michael J. Herr2, Cory R. Evans3, Jerry W. Jones4
, Michael J. Herr2, Cory R. Evans3, Jerry W. Jones4
1College of Medicine, University of Tennessee Health Science Center, Memphis Tennessee, USA
2Department of Anatomy and Neurobiology, College of Medicine, University of Tennessee Health Science Center, Memphis Tennessee, USA
3Department of Surgery, College of Medicine University of Tennessee Health Science Center, Regional One Health Center, Memphis Tennessee, USA
4Department of Anesthesiology, College of Medicine, University of Tennessee Health Science Center, Memphis Tennessee, USA
Correspondence to: Christopher D. Castelow, College of Medicine, University of Tennessee Health Science Center, Memphis Tennessee, USA
Received date: February 07, 2022; Accepted date: February 25, 2022; Published date: March 03, 2022
Citation: Castelow CD, Herr MJ, Evans CR, et al. (2022) Effects of an Acute Pain Service on Planned Ventral Wall Hernia Repair in a Matched Retrospective Cohort.
J Clin Biomed Invest 2(1): pp. 1-8. doi:
10.52916/jcbi224011
Copyright: ©2022 Castelow CD, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits
unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Background: An Acute Pain Service (APS) has been shown to improve patient outcomes and decrease complications by achieving adequate pain control and decreasing opioid use. However, it is less obvious if having a dedicated APS postoperatively directly translates to patient-centered or hospital cost benefits. This study aimed to determine if there was a cost benefit between a matched cohort of patients with and without a dedicated APS after a planned ventral wall hernia repair.
Methods: A historical cohort study was conducted. After 1:1 matching, 40 patients were included for analysis. The non-APS group received a thoracic epidural postoperatively managed by the anesthesiology department. The APS group received various continuous peripheral nerve blocks and analgesia exclusively managed by a dedicated APS. Data was recorded for each group regarding surgical techniques, postoperative complications, opioid use and induced side effects, hospital length of stay, and resource utilization for both groups.
Results: Compared to the non-APS group, adjusted opioid consumption per day was almost half in the APS group (P= 0.0067). The average hospital length of stay was 3.4 days less (P= 0.0401) , and there was a statistically significant reduction in several recovery milestones that likely contributed to a timely discharge in the APS group. After factoring costs of APS utilization, the APS was shown to save an average of $5,440.59 of total cost per patient.
Discussion: The addition of a dedicated postoperative APS significantly reduced opioid consumption and improved outcomes of patients and resulted in reduced healthcare costs.
Anesthesia, Anesthesiology, Conduction, Cost savings, Pain management.
The Acute Pain Service (APS) was developed in the late 1980’s to provide an increased level of vigilance for advanced pain management. Early APS intervention utilized Intravenous Patient-Controlled Analgesia (IV PCA); however, the side effects were significant and treatment has evolved to utilize continuous epidurals and ultrasound-guided Continuous Peripheral Nerve Block (CPNB) infusions [1]. These modalities are often further combined with Multimodal Analgesia (MMA) and actively managed by the APS [2]. An APS operates as a dedicated hospital service, most often as a multidisciplinary team led by an anesthesiologist [3,4]. The APS formulates a comprehensive post-operative pain management plan which includes evaluating post-operative pain, adjusting or recommending pain treatments and medications on daily patient rounds, reducing opioid exposure and facilitating patient recovery [5].
Broad implementation of the APS has largely been due to multiple studies indicating improved morbidity and mortality of postoperative patients treated by an APS [6]. Studies have indicated that patients seen by an APS have a decreased hospital Length of Stay (LOS) , lower pain scores, lower incidence of postoperative nausea and vomiting, reduced opioid requirements, and improved recovery milestones [7-17].
Despite the well-cited benefits from an APS to patient outcomes, hospitals contemplate investing in these services mostly due to their perceived high costs which are largely determined by adding the costs of physician and nursing time, disposables, drugs, lines, and pump systems [18-21]. There is a paucity of literature describing a true cost-benefit analysis of an APS especially as a matched cohort. However, the few studies that have sought to determine the economic impact of an APS have been favorable [9,20,21]. A more thorough cost analysis is needed to quantify the economic impact of an APS.
The purpose of this study is to determine if the implementation of a structured APS at our institution provided cost savings compared to post-operative care of patients without being followed by an APS. The primary endpoint was the difference in hospital cost between the two groups and secondary endpoints included length of stay, adverse events, post-operative opioid use and milestones related to discharge. The population of interest included patients undergoing post-traumatic planned ventral hernia repairs. This technique involves definitive hernia repair that usually occurs 6-12 months after skin graft placement and may also require adjunctive procedures such as toma reversal or fistula takedown [22]. These types of hernia repairs are very painful, traditionally requiring large doses of opioids and extended hospitalization post-operatively. This population was chosen based on the volume of these surgeries at our institution as well as the consistency of the operative techniques and surgeons during the time period of data collection. Furthermore, this population was selected based on the amount of these patients managed by the APS in addition to historic controls.
This study was performed in concordance with the STROBE Ethical Conducts of Research as well as in accordance to the Ethical Principles for Medical Research Involving Human Subjects outlined in the Helsinki Declaration of 1975. The requirement for written informed consent was waved by the Institutional Review Board (IRB). After IRB approval (20- 07378-XM), a historical cohort study was performed using information from the electronic medical record from patients undergoing elective open post-traumatic large ventral hernia repair from 2012-2020. This time frame was chosen because comprehensive patient data could be easily obtained from the medical record and represented a time before (2012-2016) and after (2016-2020) a structured APS was implemented. All data was recorded using a password-protected Microsoft Excel file (Redmond, WA).
Records were reviewed from 122 patients that underwent abdominal hernia repair. Patients who did not fulfill the criteria for elective open large post-traumatic ventral abdominal hernia repair were excluded. Patients were also excluded if they had pre-existing conditions, including severe Chronic Obstructive Pulmonary Disease (COPD), chronic constipation or neoplasmor surgical complications that would significantly influence selected outcomes or opioid utilization. Patients were also excluded if daily pre-operative opioid use was >30 Morphine Milliequivalents (MME). Forty-six patients were excluded because they had a ventral hernia repair but did not meet the definition of a planned open ventral hernia repair posttrauma admission. Twenty-three patients were excluded due to having a laparoscopic repair procedure. Two patients from the APS group were excluded due to having existing severe COPD. One patient from the non-APS group was excluded due to an aborted procedure, and another due to the inability of the researcher to retrieve the data from the EMR. One patient from the APS group was excluded due to a history of chronic pain and greater than 30 MME of opioid use prior to surgery, one was excluded due to necrosis of the graft post repair and another was excluded because they were still in the hospital at the time of data collection. In total, 46 patients were included and after matching 1:1 using age, sex, American Society of Anesthesiologists physical status score and the amount of time lapsed before their return visit, 40 patients were included with 20 patients in each group.
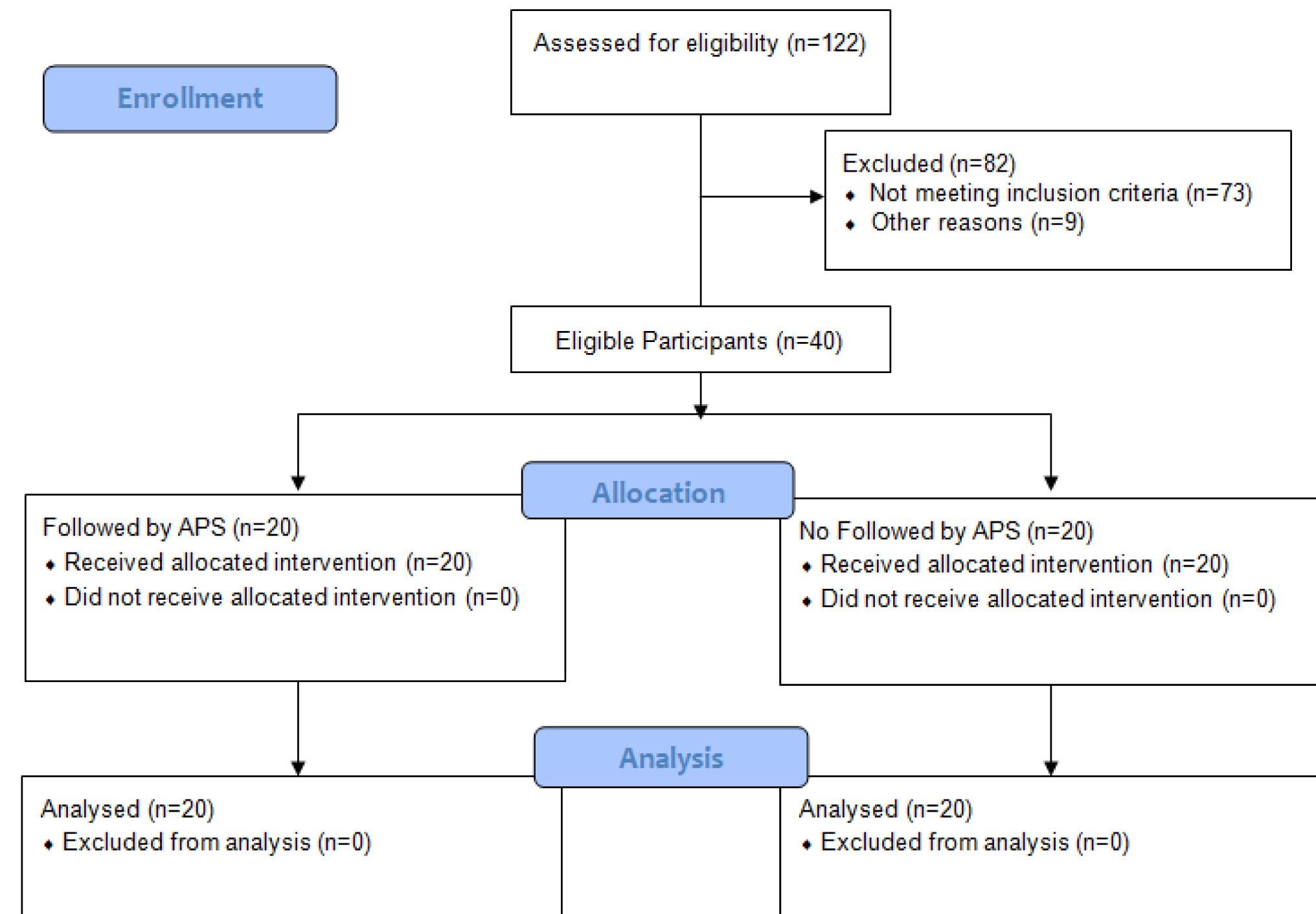 Figure 1: Patient enrollment
Figure 1: Patient enrollmentFigure 1 shows the number of patients eligible, allocated and analyzed. Patients were categorized into two groups based on whether they were under the care of APS during their stay. All patients received continuous regional analgesia for postoperative pain. All patients received a balanced general anesthetic during surgery as well as either CPNB or thoracic epidural catheter placement immediately before the procedure in the APS and non-APS groups, respectively. In some cases, CPNB placement was made by the APS in the operating room prior to emergence from general anesthetic. There were no mandated or generally followed anesthetic protocols in either group; however, practice patterns were comparable throughout the timeframe that included all studied patients. APS patients received either bilateral continuous paravertebral (PVB), subcostal transverse abdominus plane (SCTAP) or Erector Spinae Plane (ESP) nerve blocks (0.2% ropivacaine or 0.125% bupivacaine infusions) which was managed along with the rest of their postoperative analgesia by a dedicated APS. The nonAPS group received a continuous thoracic epidural (0.0625% bupivacaine with fentanyl 5 mcg/ml) which was managed by the Anesthesiology Department. Further analgesic needs not controlled by thoracic epidural anesthesia or after epidural removal in the non-APS group were managed by the trauma surgeons. Again, there was no set protocol for post-operative pain management used by the surgeons which consisted mostly of IV opioid monotherapy and IV patient-controlled anesthesia. Multimodal Analgesia (MMA) was not implemented in the nonAPS group. MMA was implemented in the APS group according to Joint Practice Guidelines on the Management of Postoperative Pain [23]. This included scheduled acetaminophen, gabapentin, methocarbamol or cyclobenzaprine and NSAID’s when not contraindicated. These medications and PO opioids every 4-6 hours were used for breakthrough pain in the APS group. IV opioids in the APS group were used only for pain unrelieved by CPNB infusion, MMA and PO opioids unless strictly NPO
Secondary endpoints were Hospital Length of Stay (LOS) , minutes in Post-Anesthesia Care Unit (PACU) , days in Intensive Care Unit (ICU) , stepdown unit, and floor bed, incidence of adverse events, days until tolerating room air, time until initial ambulation, number of doses of anti-nausea medication given, time until Nasogastric Tube (NGT) removal, time until Foley catheter removal, time until clear liquid and regular diet ordered, time until first bowel movement, and post-operative total and average daily opioid usage. Milestones such as tolerating room air, NGT removal and foley catheter removal as well as complications related to pain, opioid use and delays in patient recovery including pulmonary infection, ileus, and DVT were extrapolated from all provider’s daily progress notes. Post-operative opioid use was converted to MME using the Washington State Agency Medical Directors’ Group opioid calculator [24]. The fentanyl dose from epidural infusion for individual patients was included in the analysis; however, only completed bags of medication were included. If the epidural was stopped or discontinued and medication was wasted, this bag was not included in the analysis due to the inability to consistently determine how much of the medication had been infused. In addition, potential adverse effects from regional analgesia interventions including vascular puncture, bleeding, nerve damage, hypotension, Local Anesthetic Systemic Toxicity (LAST) , and catheter site infections, epidural hematoma, epidural infection and the number of administrations of diphenhydramine due to itching were recorded. Factors potentially suggestive of an increase in surgical complexity or postoperative pain including minutes in surgery, the number of component separations, the amount of time from the initial trauma discharge until planned ventral hernia repair and the incidence of an enterotomy were recorded.
Statistical analyses were performed using GraphPad Prism 8 version 8.4.1 (LaJolla, CA). Data sets were first tested using Kolmogorov-Smirnov test for normality. Non-normally distributed unpaired data was analyzed using a Mann-Whitney test to compare ranks. Normally distributed unpaired data was analyzed using a paired parametric t-test. Results were presented as a mean ± 95% CI of values as well as median with range in parentheses where appropriate. P values less than 0.05 were considered statistically significant. Patients were matched 1:1 based on age, sex, American Society of Anesthesiologists physical status score, and the time that had lapsed between their initial visit and date of operation. Priority was given in descending order of age, sex American Society of Anesthesiologists physical status score, then time until their return visit.
Patient demographics, American Society of Anesthesiologists physical status score, and months until return visit in the matched cohort are shown in (Table 1). Patient ages ranged from 19-65 years old. There were no statistically significant differences between the two groups in age, sex, and American Society of Anesthesiologists physical status score or in factors considered to possibly contribute to a more complex surgery including need for stoma reversal, number of component separations, incidence of enterotomy, and minutes in surgery (Table 2). Patient follow-up was variable and occurred through the inpatient hospital stay which ranged from 2-28 days. The length of time the catheter was in place for each patient varied at the discretion of the APS or anesthesiology department for the APS group and non-APS group respectively. The mean duration of catheter placement was 5.53 days ± 2.14 (standard deviation) with a range of 1 to 10 and a 95% confidence interval of the mean 4.76 to 6.30. The date of catheter removal was available for 32 patients.
| Gender M/F | Age | ASA 1/2/3 | Months until Return Visit | |
| APS | 18/2 | 40.85 ± 11.44α | 0/17/3 | 14.41 ± 8.99 |
| (CI: 35.49 to 46.21) | (CI: 9.79 to 19.03) | |||
| (Range: 20 to 58) | (Range: 7 to 45) | |||
| Non-APS | 18/2 | 42.75 ± 12.35 | 1/13/6 | 16.63 ± 16.63 |
| (CI: 36.97 to 48.53) | (CI: 4.06 to 29.21) | |||
| (Range 23 to 66) | (Range: 5 to 120) | |||
| P value | NS | 0.62 | NS | .11 |
| Number of Component Separations | Enterotomy | Minutes in Surgery | |
| APS | 1.26 ± 0.56α | 0.16 ± 0.69 | 360.60 ± 123.0 |
| (CI: 0.99 to 1.53) | (CI: -0.17 to 0.49) | (CI: 303.00 to 418.20) | |
| (Range: 0 to 2) | (Range: 0 to 1) | (Range: 166 to 626) | |
| Non-APS | 1.15 ± 0.37 | 0.25 ± 0.55 | 342.20 ± 118.4 |
| (CI: 0.98 to 1.32) | (CI: -0.01 to 0.50) | (CI: 283.30 to 401.10) | |
| (Range: 1 to 2) | (Range: 0 to 1) | (Range: 181 to 525) | |
| P value | 0.37 | 0.34 | 0.49 |
| α: mean ± standard deviation; CI: 95% confidence Interval | |||
The APS group showed a significant reduction of 3.4 fewer hospital days on average compared to the non-APS group (Table 3). There was also a 2.5-fold decrease in average total opioid consumption in MME after surgery in the APS group. When corrected for opioid consumption per day, the non-APS groups still consumed almost twice as many opioids as the APS group with an average of 32.54 MME in the non-APS group and 17.69 MME in the APS group (Table 3).
| LOS | Total Opioid Consumption (MME) | Daily Opioid Consumption (MME) | |
| APS | 8.15 ± 2.70α | 129 ± 103.30 | 17.69 ± 14.97 |
| (CI: 6.89 to 9.41) | (CI: 80.67 to 177.40) | (CI: 10.69 to 24.70) | |
| (Range: 2 to 14) | (Range: 0 to 366.5) | (Range: 0 to 33.75) | |
| Non-APS | 11.55 ± 6.14 | 330.40 ± 177.60 | 32.54 ± 18.08 |
| (CI: 8.67 to 14.42) | (CI: 244.90 to 416.0) | (CI: 23.82 to 41.25) | |
| (Range: 6 to 28) | (Range: 121 to 845) | (Range: 8 to 64.2) | |
| P value | 0.04 | 0.0001 | 0.0067 |
| LOS: Length of Stay; MME: Morphine Milliequivalents; α: Mean ± Standard deviation; CI: 95% Confidence Interval | |||
Of note, the mean total opioid consumption in the non-APS group was greater than one standard deviation above the mean compared to the non-APS group. Additionally, there was a significant reduction in days until first ambulation, days to first postoperative bowel movement, days to ordering a regular diet, days to tolerating room air, and number of days of indwelling Foley catheter in the APS group. The difference in number of doses of antiemetics and number of days with a NGT in place were not statistically significant, although there was a trend toward a decrease in both in the APS group (Table 4). There was also a trend toward a reduction in ICU and stepdown days in the APS group, but these did not reach statistical significance (Table 5).
| 1st Ambulation (Days) | 1st BM (Days) | Antiemetic (Doses) | Foley Duration (Days) | NGT Duration (Days) | Time until Regular Diet (Days) | Time until Room Air (Days) | Minutes in PACU (Days) | |
| APS | 1.3 ± 0.73α | 4.10 ± 2.00 | 1.20 ± 2.31 | 3.35 ± 1.87 | 3.90 ± 2.43 | 4.50 ± 2.46 | 1.70 ± 2.47 | 147.90 ± 59.44 |
| (CI: 0.96 to 1.64) | (CI: 3.17 to 5.03) | (CI: 0.12 to 2.28) | (CI: 2.47 to 4.23) | (CI: 2.77 to 5.04) | (CI: 3.35 to 5.65) | (CI: 0.54 to 2.86) | (CI: 118.30 to 177.40) | |
| (Range: 0 to 3) | (Range: 1 to 10) | (Range: 0 to 8) | (Range: 1 to 7) | (Range: 1 to 9) | (Range: 0 to 10) | (Range: 0 to 10) | (Range: 58 to 305) | |
| NonAPS | 2.15 ± 1.39 | 6.30 ± 2.54 | 2.85 ± 4.32 | 5.60 ± 5.26 | 4.70 ± 2.68 | 6.95 ± 4.69 | 4.50 ± 5.91 | 189.80 ± 193.20 |
| (CI: 1.50 to 2.80) | (CI: 5.11 to 7.49) | (CI: 0.83 to 4.87) | (CI: 3.14 to 8.06) | (CI: 3.45 to 6.00) | (CI: 4.76 to 9.14) | (CI: 1.735 to 7.27) | (CI: 73.05 to 306.50) | |
| (Range: 1 to 6) | (Range: 1 to 13) | (Range: 0 to 18) | (Range: 2 to 27) | (Range: 2 to 13) | (Range: 4 to 25) | (Range: 1 to 24) | (Range: 76 to 733) | |
| P value | 0.02 | 0.0042 | 0.28 | 0.03 | 0.3 | 0.0072 | 0.0058 | 0.48 | α: Mean ± Standard deviation; CI: 95% Confidence Interval |
| Days in ICU | Days in Step-down | Days in Floor | |
| APS | 0.85 ± 2.41α | 3.55 ± 4.45 | 3.75 ± 3.64 |
| (CI: -0.28 to 1.98) | (CI: 1.47 to 5.64) | (CI: 2.05 to 5.45) | |
| (Range: 0 to 10) | (Range: 0 to 14) | (Range: 0 to 11) | |
| Non-APS | 2.30 ± 5.23 | 4.90 ± 2.85 | 4.35 ± 3.79 |
| (CI: -0.15 to 4.75) | (CI: 3.57 to 6.23) | (CI: 2.58 to 6.12) | |
| (Range: 0 to 22) | (Range: 0 to 10) | (Range: 0 to 11) | |
| P value | 0.3 | 0.25 | 0.42 |
| α: Mean ± Standard deviation; CI: 95% Confidence Interval | |||
The incidence of measured adverse outcomes and complications related to regional anesthesia was rare in both groups. There were no statistically significant differences between APS and non-APS patients, but the overall incidence of adverse outcomes was 2.3 time higher in the non-APS group with a total of one incident of a post-operative pulmonary infection, three incidences of ileus, once incidence of DVT, and two episodes of hypotension in the non-APS group compared to once incidence each of a pulmonary infection and an ileus in the APS group. None of the patients on the APS group had complications related to APS interventions.
Before considering the added costs of a dedicated APS, the average savings per patient from APS implementation due to decreased hospital LOS was determined to be $5,259.80 based on an average 3.4 day reduction and the average cost of one day in a floor bed in our state for a non-profit institution which was $1,547 in 2016 [25]. This year was used because it was at the mid-point of data collection. After factoring materials, fees, and medications, the total net savings per patient with a dedicated APS was $5,440.59. The total cost of direct physician services, materials, and medications for APS rounding and interventions was determined to be $740.79 per patient. This is based on reimbursements of $277.65 per PVB procedure, $100.25 per TAP procedure, and $172.98 per ESP procedure. Each of these procedures includes a 1.5x multiplier in reimbursement because each patient received bilateral catheters, and the second procedure received only half of the original reimbursement. There were a total of ten PVB, five TAP, and six ESP procedures. Therefore, the average cost of block placement by the APS was $205.51 per patient. Also included into the total cost for direct physician services was the $34 consultation and $131.45 rounding reimbursement fee which was determined by multiplying the $20.04 rounding fee per day for a level 2 visit by the average of 6.56 hospital days in the APS group. Additionally, the $17.42 facility fee for ultrasound during ultrasound guided PVB placement was added. The healthcare cost of medications for the APS group was determined to be $272.41 per patient. This is based on a charge of $20 price per 500ml bag of 0.125% bupivacaine with an average of 3.368 bags used per patient, and the cost of IV acetaminophen which was $35.53 per vial with an average 5.77 vials used for APS patients. The cost of materials and disposables for two $40 procedure kits was $80.
The cost of APS interventions was compared to the costs of performing and managing the standard treatment modality, a thoracic epidural. The total cost of anesthesia services, materials, and medications for the non-APS group was calculated to be $921.58 per patient. The cost of performing a thoracic epidural procedure was $63. Using the $198/day reimbursement and multiplying this by the average of 4.21 days followed by the Anesthesiology Department, the epidural rounding fee totaled $833.58. The cost of an epidural procedure kit tray was $25.
Based on these calculations, the healthcare costs for utilizing an APS ($740.79) when compared to the baseline cost of care ($921.58) at our institution had a savings of $180.79. Adding the $180.79 in savings from the APS services to the average savings of $5,259.80 due to a shorter length of stay resulted in an average savings of $5,440.59 per patient.
This study sought to discover whether, in addition to a continuous regional analgesia technique, the active management of a dedicated APS translated into cost savings for patients undergoing planned ventral hernia repair. We sought to observe objective data that would demonstrate tangible financial differences. In a 1:1 matched patient cohort undergoing an identical surgical operation, the addition of a dedicated APS significantly reduced most measured outcomes and strengthened the assertion that involvement of an APS during recovery improves outcomes in surgical patients [2,7- 15,17]. The reduction in opioid utilization in the APS group likely contributed to the improved patient outcomes and reduced healthcare costs [26,27]. More importantly, this study provides evidence that a dedicated APS may independently contribute to improved patient outcomes after major surgery beyond the utilization of continuous regional analgesia techniques. This impact may be exerted through increased vigilance in patient assessment mitigating unnecessary opioid utilization, a structured analgesia plan, additional psychosocial engagement or other unrecognized means. In a previous study assessing the impact of ERAS implementation and MMA utilization on opioid use in open VHR, the utilization of opioid analgesics was significantly reduced on POD 0-2 in the ERAS group further strengthening the assertion that improving postoperative pain lies in the development of formal organization rather than developing new techniques [28].
Hospital charges and reimbursements were not made available for analysis; however, the financial implications of both groups were factored into the cost analysis. Cost savings were quantified in this study from the perspective of total costs to deliver care compared to the baseline level of care previously provided. The economic savings in this calculation is a conservative estimate and does not take into consideration all associated healthcare costs. For example, the cost of inexpensive scheduled MMA medications utilized by the APS were not considered, and the cost of electronic pumps that were utilized for both groups were left out as well. The number of ICU and stepdown unit days was not statistically significant, and adverse outcomes were rare between the two groups; therefore, these differences were not included in cost calculations. It would be important to consider the costs of non-surgical complications in a larger patient population because the cost of treating minor and major complications may be significant. According to our institution’s estimated charges for services in 2019, the cost of treating a DVT was $18,732, treating a pulmonary embolism was $22,005, treating an ileus was $16,045, and treating a pulmonary infection cost $24,625 [29]. The incidence of these complications increase when the recovery milestones shown to be improved by the APS in our study are delayed.
Potential complications with CPNB that were used in the APS group and with epidural analgesia that was used in the non-APS group were evaluated. There were no complications identified from CPNB in the APS group, but there were two incidences of hypotension necessitating either cessation or pausing the epidural infusion in the non-APS group. One non-APS patient required intubation and ICU transfer due to respiratory distress on postoperative day 3. One patient in the APS group required reintubation shortly after surgery due to pneumothorax, and another had a delayed extubation at the end of surgery, but neither a CPNB-related cause or surgical cause could be identified.
The limitations of this study are the retrospective nature of data collection, the lack of available data for direct comparisons of charges and reimbursements and the relatively low overall number of included patients. Inclusion criteria was stringent, and 1:1 matching resulted in a comparison of only 40 total patients over an 8-year time period. Increasing the number of patients may identify significant differences in complication rates. Despite the group size, we were able to find statistically significant differences in several major outcomes and clinical milestones. Due to the retrospective nature of this study, inconsistencies and gaps in pain score reporting did not allow for a comparison between the two groups.
There is also the possibility that changes in care other than that specifically related to the implementation of an APS could have led to improved patient outcomes between the two groups, and as a result, cost savings. As this study assessed patients over the span of almost a decade and the APS was not implemented at our institution until 2016, the patients in the APS group were hospitalized and had surgery more recently. As hospital stays for several surgeries have been decreasing nationwide, there could be confounding factors contributing to the overall decreased length of stay in the APS in our study. This point has been discussed in other retrospective studies comparing patient outcomes and length of stay before and after the implementation of an APS [9]. The surgical techniques, intra-operative anesthesia protocols, and discharge criteria throughout the course of the study were consistent, however, minimizing this risk.
Since charges, reimbursements and cost of stay at our institution were not available, we estimated the daily healthcare costs for hospital length of stay based on published averages for nonprofit hospitals in our institution’s state. Other costs of care were omitted or estimated due to the lack of availability of this data. Notably, the cost for dedicated APS personnel and costs to the hospital for staff education and building infrastructure to support an APS were omitted. Justifying the addition of necessary APS personnel and other hospital resources is unique to each healthcare facility and requires validation which is beyond the scope of this study. However, the current study does provide evidence that, in addition to benefits that have been recognized through the utilization of continuous regional analgesia after major surgery, significant healthcare savings are possible with a dedicated APS. The degree of healthcare cost savings may not be applicable to other surgical patient populations or patients excluded from this study. Further, the exact cause for the demonstrated savings in the APS group cannot be determined from this study.
Future prospective studies examining actual healthcare costs should be performed to validate these findings with larger patient populations and to determine the degree to which the various elements of APS care impact savings. Those elements may include the increased utilization of MMA, the utilization of specific regional analgesia techniques, aspects of the active vigilance implicit in a dedicated APS or other unrecognized factors.
This study provides evidence that the implementation of an APS significantly reduces opioid utilization, hastens postoperative recovery, shortens length of stay and demonstrates reduced healthcare costs for patients undergoing major elective open abdominal surgery following trauma. This supports the notion that the benefits of implementing an APS outweigh the costs of providing these services.
Christopher Castelow: This author helped with investigation, methodology, data collection, formal analysis, and writing. Michael Herr: This author helped conduct with investigation, formal analysis, formulation and editing of the manuscript, as well as supervision. Cory Evans: This author helped conduct the investigation, conceptualization, and editing of the manuscript. Jerry Jones: This author helped with conceptualization, investigation, resources, methodology, editing, and supervision.
None
This work was supported by the University of Tennessee Health Science Center Department of Anatomy & Neurobiology and Department of Anesthesiology from the medical student research foundation.
IRB number: 20-07378-XM

