Chrisostomos Sofoudis*, Garyfalia Bitzi, Georgios Salvanos
1st Department of Obstetrics and Gynecology, Elena Venizelou, Maternal Hospital, Athens, Greece.
Correspondence to: Chrisostomos Sofoudis, 1st Department of Obstetrics and Gynecology, Elena Venizelou, Maternal Hospital, Athens, Greece.
Received date: May 28, 2023; Accepted date: June 15, 2023; Published date: June 22, 2023
Citation: Sofoudis C, Bitzi G, Salvanos G. Vesicovaginal Fistulas (VVF): New Dilemmas and Prospectives Review of the Literature. J Obst Gynecol Surg. 2023;3(2): 10-14. doi:10.52916/jogs234034
Copyright: ©2023 Sofoudis C. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use,
distribution and reproduction in any medium, provided the original author and source are credited.
Although they were first described in 2050 BC in Egypt, Vesicovaginal Fistulas (VVF) still remain a challenging entity for both patients and healthcare services. They often result in the continuous, involuntary leakage of urine into the vaginal canal, leading to significant physical discomfort, psychological distress, and social isolation for the affected individuals.
Etiology of VVF remains miscellaneous, with the most common etiology being based on obstetric complications during prolonged labor, particularly in developing and low-resource settings. Other causes include pelvic surgery, radiation therapy, trauma, congenital and underlying medical conditions.
Effective diagnosis of VVF relies on the combination of clinical assessment, medical history, physical examination, and diagnostic procedures such as cystoscopy, imaging techniques, and dye tests. Proper detection consists crucial concerning successful treatment and can significantly improve the patient's quality of life.
Therapeutic mapping approaches for VVF include both surgical and non-surgical interventions. Conservative management may include catheterization, proper nutrition, and the use of vaginal pessaries. However, surgical intervention remains primary treatment option for most cases, aiming the repair of the fistula and restore normal urinary and reproductive function. Surgical techniques range from simple suturing to complex reconstructive procedures, and the choice of approach depends on the size, location, and complexity of the fistula.
While surgical repair offers high success rates, comprehensive postoperative care is vital to ensure optimal outcomes. Additionally, supportive care, including counseling, social reintegration, and rehabilitation, plays a crucial role in the overall recovery process.
Aim of our study consists assiduous understanding and knowledge of vesicovaginal fistula. The awareness and attention of the scientific society and healthcare providers need to be aroused regarding new prospectives, strategies and methods of detection and management of VVF.
Vesicovaginal fistula, Therapeutic mapping, Cystoscopy, Hysterectomy, Gynecology
Vesicovaginal Fistula (VVF) consists a pathological entity representing an abnormal and unusual connection between urinary bladder and vagina wall. This distressing disorder may have profound physical, emotional, and social consequences for the affected individuals.
The anatomy of female pelvis depicts a fundamental role among the development and manifestation of vesicovaginal fistulas. The urinary bladder is located in close proximity to the vaginal wall, with the vesicovaginal septum separating them. Under normal circumstances, this septum maintains the integrity of the bladder and vaginal compartments. This structure prevents any communication between the two. However, when the vesicovaginal septum is compromised, either due to injury, surgery, or underlying medical conditions, it can lead to the formation of a fistula [1].
Incidence of VVF varies globally, influenced by a multitude of factors. To be more accurate, in low-income nations and especially Africa, approximately 30.000 to 130.000 new cases are reported each year [1,2].
On the other hand, in advanced economies the incidence is relatively low. However, hysterectomy represents the main gynaecological operation leading to this complication with an incidence of 80%. Elucidating the incidence of VVF in each surgical approach of hysterectomy, laparoscopic method results in VVF in 2,2 in 1000 women, while laparotomy in 1 and transvaginal procedure in 0,2 in 1000 patients respectively [2].
In developing countries, where access to proper obstetric care may be limited, obstetric complications during childbirth account for a significant proportion of VVF cases. Prolonged and obstructed labor can exert excessive pressure on the bladder, causing ischemic injury and subsequent tissue necrosis, which can result in the formation of a fistula.
Additionally, pelvic surgery, including gynecological procedures and pelvic radiation therapy, can also contribute to the occurrence of VVF. Trauma, such as pelvic fractures or severe pelvic infections, and certain underlying conditions like bladder cancer or endometriosis, can also be associated with VVF development.
Pathophysiologic mechanism of vesicovaginal fistulas is complex and multifactorial. Common underlying pathway involves the disruption of the vesicovaginal septum, allowing urine flowing from the bladder into the vaginal canal. This disruption can occur due to tissue ischemia, infection, trauma, or surgical interventions [1].
Factors that contribute to the development of VVF include tissue necrosis, poor wound healing, infection, inadequate blood supply, and compromised tissue repair mechanisms. These factors can lead to the persistence of a fistula, hindering the natural healing process and perpetuating the abnormal communication between the bladder and the vagina [1].
Proper understanding the intricate interaction between anatomy, incidence, and the mechanism of VVF is essential regarding the diagnosis, treatment, and prevention of this condition.
Aim of this study represents the evaluation of effectiveness and safety of novel techniques regarding vesicovaginal fistula repair, improving surgical outcomes and patient quality of life [2].
An assiduous literature research was conducted abstracting manuscripts from selected medical databases such as PubMed and Cochrane databases. The authors decided the inclusion and exclusion criteria through mutual agreement.
Moreover, all the selected studies were written in English language and retrieved by using the following key words: vesicovaginal fistula, therapeutic mapping, cystoscopy. Study population of included studies encompasses patients over 18 years old. Due to this limitation the congenital VVF were excluded.
Furthermore, the cause of VVF from the retrieved articles should not be neoplasia or another systemic clinical entity. In addition, debates, brief communications, literature reviews, non-peer reviewed articles were excluded.
The initial literature searches by using the above key words revealed 245 potentially acceptable articles. However, the 151 of them did not meet the inclusion criteria as they referred to rare types of VVF. The rest of them, 94 articles, were studied deeply and in their full length. Only 18 of them can be included in this literature overview as they comprise the requirements (Figure 1).
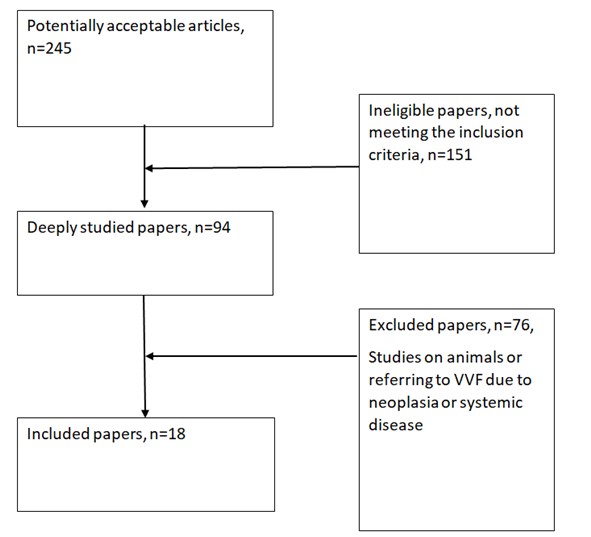 Figure 1: Flowchart of literature findings.
Figure 1: Flowchart of literature findings.Based on the information provided by the conducted research outlined in Figure 1 and Table 1 regarding different surgical interventions of vesicovaginal fistulas therapeutic mapping, it's possible to extract some general trends regarding the methods of administrating VVFs.
Table 1: Reported medical complications in women with fistula (n=210).|
Authors |
Fistula numbers |
Cause of fistulas |
Type of surgery |
Fistula location/size |
Follow-up |
|
L. Dutto [3] |
1 simple fistula |
Laparotomy-hysterectomy |
Robotic repair with perisigmoid fat flap interposition |
Vaginal vault, 1cm from the right uterine orifice/8 mm |
6 months uneventful |
|
O. A. Ojengbede [4] |
2 cases of simple fistulas |
Superior rami fracture Prolonged obstructed labour |
Vaginal approach |
Mid-vaginal fistula 2 × 2 cm and 1 × 2 cm |
2 weeks- uneventful |
|
Soo-Hwan Park [5] |
1 simple fistula |
Hodge pessary insertion |
Conservative treatment |
Vaginal fornix- right side of the bladder/ 1 cm |
1 year- uneventful |
|
V. Agrawal [6] |
10 simple fistulas |
Hysterectomy (2 vaginal, 3 open, 3 laparoscopic, 2 robotic-assisted laparoscopic ) |
Robotic-assisted laparoscopic repair |
Supratrigonal/size not mentioned |
4 to 44 months- uneventful |
|
T. D. Javali [7]
|
22 cases of simple fistulas |
Hysterectomy (vaginal, open, laparoscopic- assisted vaginal), Bilateral salpingo-oopherectomy |
Simplified Laparoscopic Approach- The M.S. Ramaiah Technique |
Supratrigonal/4 mm-1.8 cm |
2-45 months- uneventul |
|
A. S. Sawant [8] |
1 simple fistula |
Abdominal hystrectomy |
Cyanoacrylate injection in the fistula tract |
Trigonal 4 mm single fistula on the right side |
5 months- uneventul |
|
A. Gedik [9] |
53 cases of simple fistulas |
Normal delivery (6) C-section (25) Total abdominal hysterectomy (22) |
Transabdominal transvesical repair (TAV)(28) or transvaginal repair (TV) (25) |
Supratrigonal (46) Trigonal/infra trigonal (7) 15-20 mm |
Successful rate TAV group 96,4% and TV group 100% 1 year follow-up- uneventful |
|
D. H. Hernández [10] |
1 multi-tract fistula and 1 simple fistula |
Vaginal hysterectomy Abdominal hysterectomy |
Transvesical laparoscopic repair Extra vesical laparoscopic repair |
Supratrigonal at the right ureteral meatus/ size not described Uterus midline/1 cm |
1 year- uneventful 6months- uneventful |
|
B. Johnson [11] |
1 simple fistula |
C- section |
Robotic-assisted laparoscopic total hysterectomy with repair of both her vesicovaginal and vesicouterine fistula with omental interposition flap |
2 cm from her left ureteral orifice/ large- exact size not described |
3 months- uneventfully |
|
S. Niu [12] |
1 simple fistula |
Laparoscopic total hysterectomy and bilateral salpingectomy |
Minimally invasive complete urinary tract drainage |
Posterior bladder wall/ 1 cm |
1 year- uneventful |
|
G.S. Bora [13] |
29 cases of simple fistula 1 case of complex- multiple fistula |
Hystrestomy (27) Obstructed labour (2) Unknowed (1) |
Robotic-assisted repair |
Supratrigonal (27) Trigonal (2) Cervicovesicouterine (1)/10.4 mm
|
38 weeks 2 recurrences (the complex fistula and an supratrigonal fistula 2.5 cm) |
|
M.K. Shirvan [14] |
12 cases of simple fistula |
Hysterectomy (6) C-section (6) |
Autologous Platelet Rich Plasma Injection and Platelet Rich Fibrin Glue Interposition |
Position not described/ 2>5 mm 10<5 mm |
6 months- uneventful |
|
L. A. N Bragayrac [15] |
3 cases of complex fistula 1 simple fistula |
Abdominal hysterectomy |
Robotic repair with trans peritoneal-transvaginal approach
|
Position not described/ 0.3-2 cm
|
1-21 months- uneventful |
|
J.R. Miklos [16] |
44 cases of fistula |
Hysterectomy (41) Mesh surgery (1) Unknown cause(1) |
Laparoscopic extravesical repair |
Position and size not described |
17,3 months- 1 recurrence |
|
C.S. Pietersma [17] |
1 complex fistula |
Hysterectomy |
Robotic-assisted laparoscopic repair |
Top of the vaginal wall/ Size not described |
6 months- uneventful |
|
C. Reinenauer [18] |
4 cases of simple fistula |
C-section (3) Forceps- assisted labor (1) |
Abdominal-vaginal fistula excision and closure with omentum flap (3) Transvaginal excision and multilayer closure (1) |
Upper third of the anterior vaginal wall (3) Vaginal apex(1) 3-40 mm |
3 months- uneventful |
A wide variety of surgical approaches can be used for the treatment of VVFs. These approaches include laparotomy-hysterectomy, robotic repair, vaginal approach, laparoscopic-assisted repair and conservative treatment, as well.
Novel techniques, scientific accomplishments, cutting-edge technology, substances and biological fluids have been tested by a good many researchers and surgeons in order to find new ways for managing the VVFs.
Although tested in small population, all of them have leaded in a successful management of the patients without great complications. A majority of the cases are reported as "uneventful" or "successful," suggesting that the applied techniques were generally effective in treating the vesicovaginal fistulas.
Table results reveal fistulas types located in different regions (e.g., vaginal vault, mid-vaginal, supratrigonal) and varied in size. This highlights the importance of tailoring the surgical approach to the specific characteristics of each fistula, which could impact the overall success of the treatment.
The follow-up durations range from a few weeks to over a year. This suggests that researchers were interested in evaluating the long-term effectiveness of their chosen techniques. Longer follow-up periods allow for a better understanding of the recurrence rates and overall success of the procedures.
The conducted research had strict criteria regarding the causes of the vesicovaginal fistulas. These could vary, including factors like obstructed labor, hysterectomy, pelvic fractures, and more. This reflects the complexity of the condition and the need for adaptable treatment approaches based on the underlying cause [19,20].
Vesicovaginal Fistula represents a multifactorial entity that reflects the abnormal connection between the vaginal wall and the bladder leading to involuntary leakage of urine into the vaginal canal.
At the turn of our century the technological advances have resulted in the develοpment of new ways of management of several medical conditions and as a result of the vesicovaginal fistulas [1,2].
The management of VVF involves not only surgical repair and conservative approach under different circumstances. Advancements were being made to improve outcomes and reduce the recurrence rate [11,12]. To outline briefly, prospective approaches are cited here. Minimally Invasive Techniques such advances in laparoscopic and robotic-assisted surgeries have shown potential in VVF repair. These techniques offer smaller incisions, reduced trauma, and faster recovery times for patients. Minimally invasive procedures may result in less scarring and fewer complications compared to traditional open surgery [20].
Robotic surgery has become increasingly popular for the repair of Vesicovaginal Fistulas (VVF), as it offers several advantages over traditional open surgery. This technique utilizes a robotic surgical system to perform precise and intricate procedures with smaller incisions.
A typical robotic surgery for VVF repair includes the steps contextualized below. The preoperative preparation and plan is necessary for the thorough evaluation of patient’s condition and includes various diagnostic tests [3,5].
The patient is placed under general anesthesia in a lithotomy position. The patient positioning provides the surgeon access to the pelvic area while allowing optimal robotic instrument manipulation.
Additionally, prophylactic antibiotic treatment is administered to the patient. Small incisions (usually 3-4) are made in the abdomen, through which trocars (hollow tubes) are inserted. The robotic surgical system's arms and camera are then docked into these trocars. The surgeons control the robotic arms, which hold surgical instruments, through a console interface. They carefully identify the vesicovaginal fistula's location, size, and extent using the camera and robotic instruments [3].
The fistulas are sutured meticulously sutures and tightly closed. In some cases, the surgeon may use tissue grafts or other materials to reinforce the closure and improve its durability. A careful inspection of the area ensures no leaks or other complications. Once the procedure is completed, the robotic instruments are removed [3,6,11].
Furthermore, use of substances like cyanoacrylate or fibrin glue interposition and other drainage techniques have been used as alternative ways of conservative treatment or in order to facilitate minimal invasive technologies [8,12].
The above techniques like all the surgical repair techniques described in the literature had no or small percentage of complications. The only complication mentioned was the recurrence of the fistula and concerned a complex and a large (over 2.5 cm) fistula respectively [13].
Moreover, only one of the selected studies used the conservative approach. This VVF repair technique was used for the treatment of a simple fistula, 1 cm diameter size [5].
In all the other studies, invasive surgical interventions were preferred.
Vesicovaginal fistula management remains a complex field with numerous variables, and individual patient outcomes. Researchers likely aimed to contribute to the overall understanding of effective treatment approaches and patient outcomes for this condition.
Conductive studies of current literature have led to minimal invasive techniques such as robotic-assisted repair and substance interposition concerning optimal therapeutic strategy.
There is a shift towards the use of substances that inhibit the communication between the anatomical structures of the vagina and the urinary bladder. Ultimate scope appears to be replacing surgical sutures in the respective fistula with the application of appropriate substances.
In addition, invasive methods appear to be preferable and more effective compared with the conservative one.
To conclude, conservative ways of VVF management and traditional surgical approaches have not been abandoned. Prevention strategies remain crucial parameter regarding the treatment of VVF.
Identifying and addressing risk factors that contribute to the development of VVF can help prevent this condition. Access to skilled obstetric care, timely management of prolonged obstructed labor, and safe delivery practices can play a crucial role in reducing the incidence of VVF, particularly in developing countries where it remains a significant problem.
No

