Namita Jain1* , Isha Kriplani2, Seema Sharma3, Alka Kriplani4
, Isha Kriplani2, Seema Sharma3, Alka Kriplani4
1Consultant, Department of Obstetrics and Gynaecology, Paras Hospital, Gurugram, Haryana, India
2Associate Consultant, Department of Obstetrics and Gynaecology, Paras Hospital, Gurugram, Haryana, India
3Senior Consultant, Department of Obstetrics and Gynaecology, Paras Hospital, Gurugram, Haryana, India
4Head of Department of Obstetrics and Gynaecology, Paras Hospital, Gurugram, Haryana, India
Correspondence to: Namita Jain, Consultant, Department of Obstetrics and Gynaecology, Paras Hospital, Gurugram, Haryana, India
Received date: April 15, 2022; Accepted date: April 28, 2022; Published date: May 5, 2022
Citation: Jain N, Kriplani I, Sharma S, et al. (2022) Spontaneous Rupture of Huge Ovarian Endometrioma and Its Successful Laparoscopic Management: A Case-Study
and Review of Literature. J Obst Gynecol Surg 3(1): pp. 7-9. doi: 10.52916/jogs224023
Copyright: ©2022 Jain N, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted
use, distribution and reproduction in any medium, provided the original author and source are credited.
Endometriosis is a common entity with varying clinical presentation. Spontaneous rupture of a huge ovarian endometrioma presenting as an acute emergency is a rare occurrence. One such case presenting as an emergency and its successful laparoscopic management is discussed here.
Endometriosis, Rupture, Ovarian, Laparoscopic.
Due to emergency nature of surgery the option of preoperative uterine artery embolisation was not feasible and hence decision of stepwise de-vascularisation was taken. The devascularisation was done at the level of B/L uterine arteries (Figure 2), utero ovarian anastomosis bilaterally followed by removal of the three myomas. The largest myoma was found to have necrotic changes (Figure 3) and thus was removed completely from base. Intra-operative blood loss was approximately 400cc. Post operative period was uneventful and Patient was discharged on day 3 of LSCS.
Endometriosis is an enigmatic condition. Endometriosis has many complications like infertility, chronic pelvic pain, infection, torsion etc. Rupture of an endometrioma is a rare complication. It can become quite painful, ending in a surgical emergency. One should be conscious of such possibility to improve the patient outcome. The diagnostic gold standard remains laparoscopy.
Hereby, we discuss the rare presentation of spontaneous rupture of huge endometrioma leading to severe anaemia and massive intraperitoneal haemorrhagic collection managed laparoscopically. Very few such cases have been reported in literature and managed laparoscopically.
37 year old P1L1 presented to the emergency with severe abdominal pain and breathing difficulty. Her previous cycles were regular with gradually increasing dysmenorrhea over a period of 3 years. She gave history of intake of oral analgesics for dysmenorrhea with no prior history of hormonal medications. On admission, she had pulse rate 110bpm, respiratory rate 24/min, blood pressure 90/60mmHg and SpO2 of 97%. On an abdominal examination, gross distention with shifting dullness was observed. On per vaginal examination, fullness in right adnexa with tenderness was noticed. Her urinary pregnancy test was negative and USG showed huge right ovarian endometrioma and gross hemoperitoneum reaching upto hepatic pouch. A contrast MRI was done which suggested 14 × 12cm ruptured ovarian endometrioma with gross hemoperitoneum (Figure 1). Her haemoglobin and CA-125 came out to be 7.2gm/dl and 400 IU/l, respectively. Laparoscopic surgery was planned.
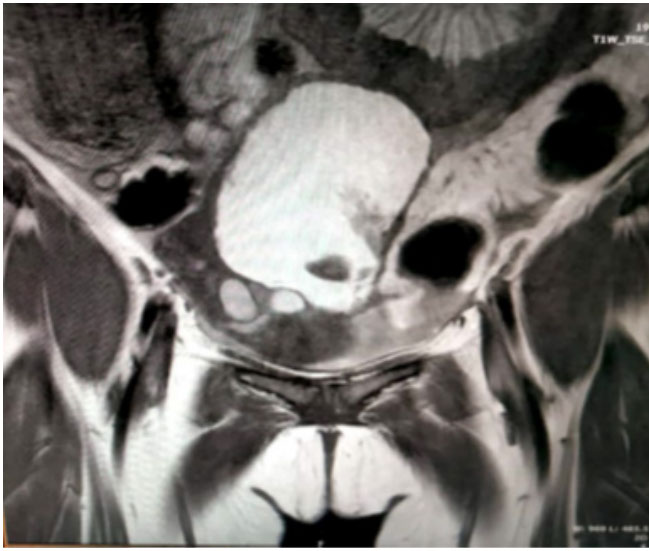 Figure 1: : MRI images showing huge ovarian endometrioma.
Figure 1: : MRI images showing huge ovarian endometrioma.lntra-operatively, omental adhesions were seen. Peritoneal cavity was filled with 5 litres of chocolate colored fluid (Figure 2A). Uterus was bulky, 14 × 12cm ruptured huge right ovarian endometrioma stuck to posterior wall of uterus (Figure 2B). and in left ovary 5 × 5 cm endometriotic cyst were seen. Right salpingo-oopherectomy was done as no healthy ovarian tissue identified. Good amount of left ovarian tissue could be preserved after endometriotic cystectomy. 2 units of PRBC were transfused during surgery. Her post-operative period went uneventful. She was discharged on day 3 of her surgery. Her histopathology report confirmed endometriosis. She was symptom free after one year of surgery. Follow-up USG showed normal uterus and normal left ovary.
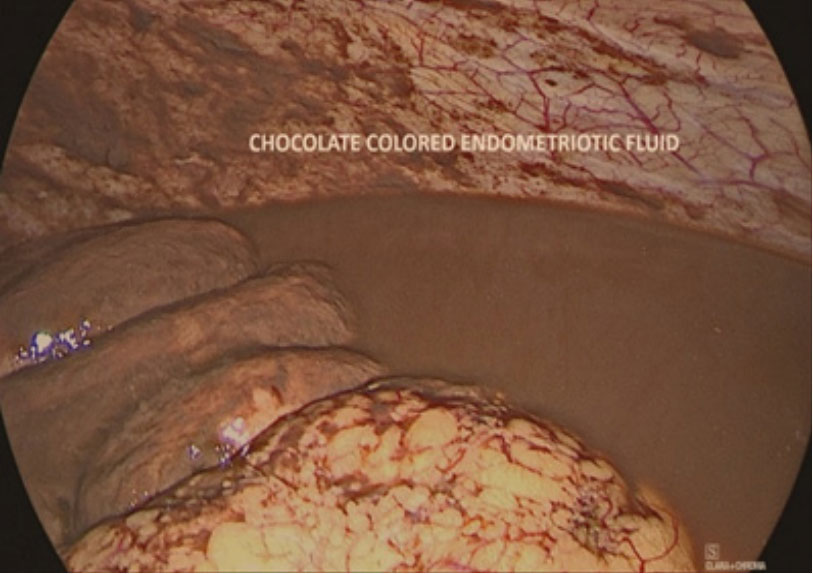 Figure 2A: : Intra operative images showing chocolate colored endometriotic fluid.
Figure 2A: : Intra operative images showing chocolate colored endometriotic fluid.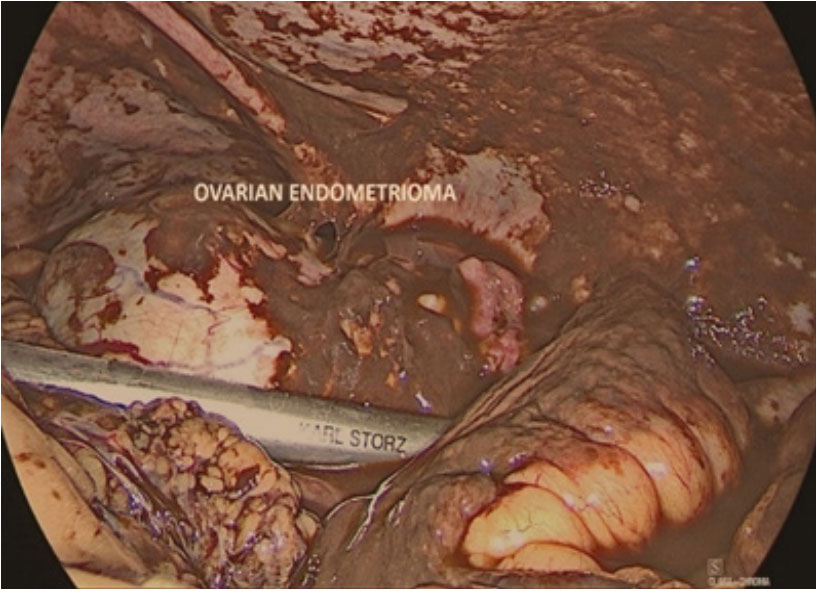 Figure 2B: : Intra operative images showing ovarian endometrioma
Figure 2B: : Intra operative images showing ovarian endometriomaThe most common presenting symptoms of endometriosis are dysmenorrhea and pelvic pain. Spontaneous rupture of a huge ovarian endometrioma presenting as an acute emergency is a rare occurrence. Such presentation might be unknown even to the experienced clinicians. Massive hemoperitoneum with endometriosis is extremely rare with less than 100 cases reported in literature. All patients were of childbearing age likely due to hormonal levels and occurrence of menses.
Differential diagnosis most commonly is the ruptured ectopic pregnancy, ovarian or adnexal torsion, ruptured dermoid cyst, pelvic inflammatory disease, follicular rupture in women with coagulopathy, abdominal tuberculosis, ovarian hyperstimulation, ovarian malignancy or surgical emergencies.
Medical management has been attempted but 89% cases of patients ultimately underwent a surgical procedure. The average volume of abdominal collection was 4470 ± 2625 mL. Various surgical interventions reported include drainage of collected blood, excision or endometriotic spot fulguration through laparotomy or laparoscopy, lysis of adhesions, abdominal hysterectomy, uni or bilateral salpingo-oophorectomy, ovarian wedge resection or a combination of these [1].
Several aspects of the case like acute presentation, size of endometrioma and its laparoscopic management are the main highlights.
Why endometrioma ruptures, the exact cause is not known but a huge endometrioma due to rapid accumulation can cause weakening of the cyst wall. It can present as chemical peritonitis due to the leakage of old blood. Various predisposing factors like sexual intercourse, ovarian aspiration for IVF or PID could be identified in the literature.
Morgan et al. reported a case of a 27-year-old who presented with pain and required multiple blood transfusions [2]. Ultimately, a diagnostic paracentesis was performed and 4.5 litres of grossly bloody ascitic fluid was removed. Oral contraceptive pills were started with diagnosis of endometriosis. At 2 weeks followup visit, no recurrence of symptoms noted. However, some authors suggest early tendency towards surgical exploration to minimise long term effects like chronic pelvic pain, adhesions and infertility.
Pandey et al. published a case of 23 year nulliparous women who presented with acute pain abdomen [3]. Her CT showed 12 cm left ovarian mass with fluid collection in the intraabdominal cavity and thickened omentum mimicking ovarian cancer. The patient’s CA-125 and CA–19-9 levels were 25,149 U/ mL and 5379 U/mL, respectively. On laparoscopy, ruptured left ovarian endometrioma with diffused chocolate content all over intra-abdominal cavity was seen. They concluded that highcombination CA-125 and CA–19-9 concentrations could indicate the presence of a ruptured endometrioma. Our case also had high CA-125 levels.
Huge ovarian endometrioma with gross intraperitoneal collection with raised CA 125, can masquerade as ovarian malignancy. Rao et al4 reported a case of bilateral ovarian endometrioma (6.5cm) with unilateral leak with moderate haemorrhagic fluid and raised CA 125 of 8482 managed laparoscopically [4]. Rare instances of malignancy have been documented, therefore, histology specimen must be sent in cases of ovarian endometrioma and/or deep infiltrating endometriosis.
Wang L, et al. published a case of a 35-year-old unmarried female had multiple episodes of pain in the left lower abdomen that recurred during menstruation. Ultrasound examination suggested a 4.9 cm × 4.6 cm left endometriotic cyst [5]. CT of the abdomen and pelvis revealed a low-density focus measuring approximately 38 mm in diameter, a blurred mesentery fat plane in the pelvic cavity, and pelvic effusion. Left ovarian cystectomy, electrocautery for endometriotic lesions, myomectomy, and pelvic adhesion lysis were performed under laparoscopy. The postoperative diagnosis was left ovarian chocolate cyst rupture.
Rupture of endometrioma is also reported during pregnancy. Zhen lieu et al6 reported a case of ruptured endometrioma of approx. 5cm in pregnancy at 18 weeks and CA 125 1010 managed laparoscopically. Author suggested rapid growth under hormonal stimulation or increased blood supply or due to increased pressure effect of rising uterine size on the endometriotic cyst might be a predisposing factor. They concluded that such event can be life-threatening and managing it timely improves maternal and fetal outcome.
Size of endometrioma or massive hemoperitoneum is not a contra-indication for laparoscopy. Certain deviations we used to manage it laparoscopically were supraumbilical primary port in place of umbilical port, irrigation with high pressure fluid and 10mm suction irrigation tips. Irrigating more mature clots will help lyse the solid portions, also facilitating removal of blood collection.
Early and accurate diagnosis is paramount. Emphasis should be towards early surgical intervention with aim of effective disease eradication and in long term, preventing adhesion formation and preserving fertility.
The author declares no conflict of interest.

