Vinita Singh*1 , Sangeeta Pradhan2, Vijaylakshmi Shanbhag2, Pushpawati Thakur1, Chandrashekhar Shrivastava1, Neetu Kumari2
, Sangeeta Pradhan2, Vijaylakshmi Shanbhag2, Pushpawati Thakur1, Chandrashekhar Shrivastava1, Neetu Kumari2
1Consultant, Department of Obstetrics and Gynaecology, All India Institute of Medical Sciences (AIIMS), Raipur, India
2Resident, Department of Obstetrics and Gynaecology, All India Institute of Medical Sciences (AIIMS), Raipur, India
Correspondence to: Vinita Singh, Consultant, Department of Obstetrics and Gynaecology, All India Institute of Medical Sciences (AIIMS), Raipur, India
Received date: January 02, 2023; Accepted date: January 14, 2023; Published date: January 21, 2023
Citation: Singh V, Pradhan S, Shanbhag V, et al. Laproscopic Assisted Ovarian Cystectomy: A New Approach. J Obst Gynecol Surg.
2023;4(1): 1-4. doi:10.52916/jogs234031
Copyright: ©2023 Singh V, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use,
distribution and reproduction in any medium, provided the original author and source are credited.
Ovarian cysts are fluid-filled sacs that are discovered incidentally, on physical examination, imaging or symptomatic. Recently there has been increase in ovarian cysts in unmarried, nulligravida young women, so ovarian preserving minimal invasive surgeries have come into role with compared to open surgeries done in the past which resulted in more adhesions, subfertility and poor reproductive outcome. This is a case report of 26 years, unmarried female who had large right ovarian cyst (20 × 16 × 14) cm with complaint of mass in abdomen since 4 years , underwent laparoscopic assisted ovarian cystectomy by mini laparotomy with no intraoperative or postoperative complications. So the ovarian cystectomy by laparoscopic guided mini laparotomy is a better alternative in minimally invasive surgery for huge benign ovarian cysts.
Ovarian cyst, Laparoscopic assisted ovarian cystectomy, Mini laparotomy, Minimally invasive surgery
Ovarian cysts are fluid-filled sacs that are discovered incidentally, on physical examination, imaging or symptomatic [1]. The etiology of ovarian cysts or adnexal masses ranges from physiologically normal (follicular or luteal cysts) to ovarian malignancy. Ovarian cysts can occur at any age but are more common in reproductive years and have an increased occurrence in menarchal females due to endogenous hormone production. Benign tumors are more common in young females, but elderly females frequently present with malignant lesions [2]. Recently there has been increase in the detection of ovarian cysts in symptomatic unmarried, nulligravida young women, which has led to evolution of ovarian preserving minimal invasive surgeries as open surgeries often results in adhesions, subfertility and poor reproductive outcome [3].
A 26-year, Nulligravida, unmarried female presented to the outpatient department of All India Institute of medical sciences, Raipur, India, with mass per abdomen extending up to xiphisternum which was insidious in onset and gradually progressive since 4 years. On examination the abdomen was over distended with tense cystic mass extending up to the xiphisternum and the lower border of the mass could not be felt suggesting its pelvic origin. Ultrasound Sonography Test (USG) and Contrast Enhanced Computerized Tomography (CECT) abdomen and pelvis were done which was suggestive of right adnexal enhancing simple cystic lesion possibly arising from right ovary of dimension (16 × 10 × 20) cm without any internal vascularity. All the tumor markers were done to rule out malignant ovarian tumor. CA 125 was raised (58 IU/ml) and rest others were within normal limit. Since the patient was young, unmarried and the investigations were pointing towards a benign etiology, a minimal invasive approach was planned for ovarian cystectomy in this patient. For laparoscopic cystectomy the size of the cyst extending up to the xiphisternum posed a problem and so the discission of laparoscopic assisted ovarian cystectomy through mini laparotomy was performed.
The procedure was performed under general anesthesia with the patient placed in dorsal position. Under all aseptic precautions painting and draping was done. A transverse mini-laparotomy (2-3 cm) incision in the midline 2 cm above the symphysis pubis to facilitate port insertion was given (Figure 1). The rectus sheath was opened in midline. Once the parietal peritoneum was opened tense glistening cyst wall was seen beneath. The cyst was punctured using veress needle followed carefully by trocar and canula insertion. A suction tube was attached and clear fluid of around 5 liters was drained out without spillage (Figure 1). The rent in the cyst wall was held using a long artery forceps inside the abdominal cavity. The right ovary and cyst wall were gently delivered outside through the mini-laparotomy skin incision (Figure 2).
 Figure 1: Minilaprotomy incision and insertion of veress needle.
Figure 1: Minilaprotomy incision and insertion of veress needle. Figure 2: Delivery of affected ovary after fluid aspiration.
Figure 2: Delivery of affected ovary after fluid aspiration.Carefully the cyst wall was enucleated from ovarian tissue (Figure 3). The ovary was preserved and cyst wall was completely excised. Haemostatic sutures were taken and cautery was avoided to prevent any damage to the ovary. The right ovary and the tube were carefully reposited back. Then an umbilical port was inserted to visualize ovaries, uterus, other pelvic structures, to check hemostasis and proper placement of ovaries inside abdominal cavity (Figure 4). The mini laparotomy incision and port site were closed with subcutaneous sutures. The patient was discharged on post-operative day 2 without any complications and followed up in Outpatient basis. The histopathology report was suggestive of benign serous cystadenoma of ovary.
An ovarian cyst can be broadly classified as physiological and pathological [4]. Follicular cysts and luteal cysts as physiological; benign, malignant, and borderline ovarian tumors as pathological. Laparotomy is the oldest and traditional approach for removal of ovarian cyst and is an entirely invasive procedure. Laparoscopy has emerged as a less invasive technique for invasive procedures in pelvis over the last 2 decades [5].
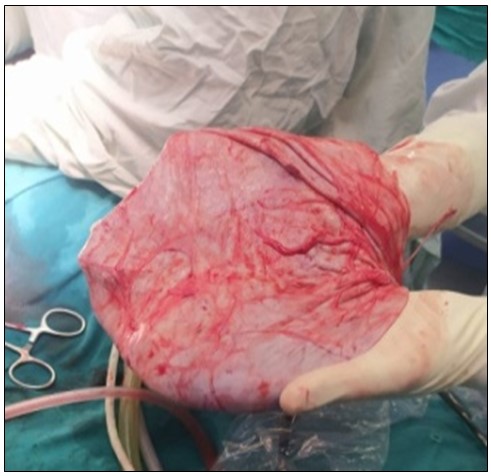 Figure 3: Excision of cyst wall.
Figure 3: Excision of cyst wall.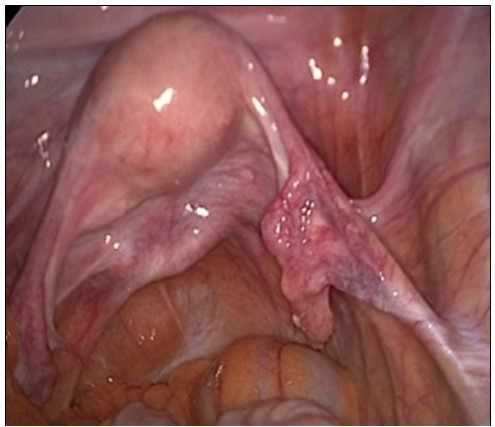 Figure 4: Restoration of ovary inside pelvis.
Figure 4: Restoration of ovary inside pelvis.Benign giant ovarian cysts over 15 cm are rarely encountered nowadays because most are diagnosed and treated at an early stage. Standard surgical management requires a midline laparotomy to minimize the risk of cell spillage in case of unexpected malignancy. This surgical technique, though ontologically safe, is associated with an increase in morbidity, especially post-operative pain, as well as an increase in hospital length of stay. Between laparoscopy and laparotomy another possible alternative is the minilaparotomy, which represents because of a small incision (2-4 cm) an interesting option. A new approach of laparoscopic assisted ovarian cyst removal by mini laparotomy was tried in this case which is of great advantage especially in a low resource setting.
Another minimally invasive approach for ovarian cystectomy is vaginal ovarian cystectomy. Vaginal Ovarian Cystectomy (VOC) refers to the management of ovarian cysts through the vaginal canal. The peritoneal cavity is entered at the Pouch Of Douglas (POD) or cul-de-sac through an incision at the posterior vaginal fornix allowing access to the pelvic organs [6]. But it has not gained widespread acceptance. This is secondary to the potential difficulty in entering the peritoneal cavity through the posterior fornix (requiring posterior colpotomy or culdotomy) and its close proximity to the rectum [7]. So the ovarian cystectomy by laparoscopic guided mini laparotomy is a better alternative in minimally invasive surgery for huge benign ovarian cysts.
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
The authors declare no conflict of interest.
No.

