Mouhamadou Mansour Niang1,2*, Fatou Samb2, Djibril Bahaid Sow3, Eric Armand Serge Wilson3, Cheikh Tidiane Cisse1,2
1Department of Obstetrics and Gynecology, Cheikh Anta Diop University of Dakar, Senegal
2Department of Obstetrics and Gynecology, Hospital Institute of Social Hygiene, Senegal
3Military Hospital of Ouakam, Senegal
Correspondence to: Mouhamadou Mansour Niang, Department of Obstetrics and Gynecology, Cheikh Anta Diop University of Dakar, Senegal
Received date: July 13, 2022; Accepted date: August 01, 2022; Published date: August 06, 2022
Citation: Niang MM, Samb F, Sow DB, et al. Hysterectomies for Benign Utero-Adnexal Lesions: Evolution of the Approach, Indications and Results About 392 Cases Collected at the Department of Gynecology and Obstetrics of Ouakam Military Hospital, Dakar, Senegal Between 2006 and 2016. J Obst Gynecol Surg. 2022;3(2):
18-22. doi:10.52916/jogs224027
Copyright: ©2022 Niang MM, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use,
distribution and reproduction in any medium, provided the original author and source are credited.
Objectives: To describe the socio-demographic characteristics of the patients, to analyze the evolution of the approach, the indications, the characteristics of the procedure (type of anesthesia, surgical procedure, per and postoperative complications, associated gestures, blood transfusion And duration of hospitalization) according to the approach and to specify the results of the hysterectomy for benign utero-adnexal lesions. Materials and methods: This was a retrospective, descriptive and analytical study of the hysterectomies performed for benign utero-adnexal lesions at the Department of Obstetrics and Gynecology of the Ouakam Military Hospital over a period of 11 years from 1st January 2006 to December 31st, 2016. Results: During the study period, we performed 392 hysterectomies among the 5,578 programmed gynecological surgeries, ie a frequency of 7%. There were 153 hysterectomies per laparotomy (39.03%), 222 vaginal hysterectomies (56.63%) and 17 coelio-prepared hysterectomies (4.3%). Between 2006 and 2016, laparotomy, vaginal and coelio-prepared hysterectomies rates increased from 76.9% to 23.1%, 39% to 56.6%, and 0 to 4.3%, respectively. Patients were aged 51.8 years (37-83 years) with an average parity of 5 (0-14). Indications were dominated by uterine fibroids (71.2%) in the laparotomy group, severe cervical dysplasia (36.9%) and uterine fibroids (28.8%) in the vaginal Benign endometrial disease (35.3%) and uterine fibroid disease (29.4%) in the "coelio-prepared" group. We performed 346 total interannexual hysterectomies (88.3%) and 46 total hysterectomies with bilateral adnexectomy (11.7%). The procedure was mostly spinal anesthesia (79.8%) and lasted an average of 89 minutes (45-215 minutes). The mean hemoglobin was 13.1 g/dL preoperatively and 11.1 g/dL postoperatively, a difference of 2g/dL on average. We recorded 11 intraoperative complications (2.8%). There were 6 severe haemorrhages, 3 digestive wounds and 2 bladder wounds. The duration of hospitalization was on average 4 days [2-7] and the follow-up was mostly simple (97.7%). Conclusion: This study on hysterectomies at the Military Hospital of Ouakam showed that the rate of laparotomy hysterectomies had decreased over the past decade in favor of vaginal and coelio-prepared hysterectomies. The indications for this procedure were dominated by uterine myomatosis and severe cervical dysplasia, and intraoperative complications, dominated by haemorrhages, were globally rare.
Hysterectomy, Ways, Indications, Complications
Hysterectomy is, with cesarean section, one of the most frequent procedures: 75,000 hysterectomies were performed in France in 2002; 660,000 in the United States [1]. However, this rate varies from region to region and is dependent on the socioeconomic category, the level of education and the ethnic origin of the populations. In Senegal, its actual frequency is poorly estimated. Also, this intervention has sparked a lot of discussion regarding its indications, approaches and complications [2]. In developing countries where this procedure has long been performed by the abdominal route, we have been witnessing for a few years a widening of the routes first with the introduction of the vaginal and laparoscopic routes. The objectives of this study were to determine the frequency of hysterectomies for benign utero-adnexal lesions at the Gynecology-Obstetrics Department of the Ouakam Military Hospital, to describe the socio-demographic characteristics of the patients and to analyze the evolution of the pathway d First, the indications, the characteristics of the intervention (type of anesthesia, operating time, per and post-operative complications, associated procedures, blood transfusion and length of hospital stay) depending on the route.
It was a retrospective, descriptive and analytical study concerning hysterectomies performed for benign utero-adnexal lesions at the Gynecology-Obstetrics Department of the Ouakam Military Hospital over an 11-year period from January 1, 2006 to December 31 2016. We retained 392 files. We excluded hysterectomies performed for cancer and obstetric hysterectomies for hemostasis.
The parameters studied were the characteristics of the patients (age, parity, period of genital activity, history of pelvic surgery), the approaches, the indications and the per and postoperative data (type of anesthesia, operating time, complications per and post-operative, associated gestures, blood transfusion and length of hospitalization).
The data were entered and analyzed with the SPSS version software.
During the study period, we performed 392 hysterectomies for benign utero-adnexal lesions among the 5578 scheduled gynecological surgical procedures, i.e. a frequency of 7%. They were distributed as follows: 153 hysterectomies by laparotomy (39.03%), 222 vaginal hysterectomies (56.63%) and 17 coelioprepared hysterectomies (4.3%).
The patients were on average 51.8 years old [37-83 years old]. The average age in the “laparotomy”, “vaginal route” and “coelio-prepared route” groups was 48.5 years, 55.2 years and 51.6 years, respectively. The average parity of 5 [0-14]. The characteristics of the patients are summarized in Table 1.
| Patients characteristics | Laparotomy (n=153) |
Vaginal route (n=222) |
Coelio-prepared (n=17) |
| Average age (years) | 48.5 (37-70) |
55.2 (38-83) |
51.6 (41-64) |
| 30-39 | 15 (9.8%) |
9 (4%) |
0 |
| 40-49 | 83 (54.2%) |
75 (33.8%) |
7 (41.2%) |
| ≥ 50 | 55 (35.9%) |
138 (62.2%) |
10 (58.8%) |
| Parity | |||
| nulliparous | 25 (16.3%) |
10 (4.5%) |
0 |
| primiparous | 11 (7.2%) |
17 (7.6%) |
3 (17.6%) |
| paucipares | 44 (28.7%) |
39 (17.5%) |
3 (17.6%) |
| Multipar | 63 (41.2%) |
156 (70.3%) |
11 (64.7%) |
| Period of genital life | |||
| Genital activity | 91 (59.5%) |
71 (32%) |
5 (29.4%) |
| Menopause | 62 (40.5%) |
151 (68%) |
12 (70.6%) |
| History of pelvic surgery | 0 |
7 (3.15%) |
0 |
| Average pre-operative hemoglobin level (g/dl) | 13.3 |
12.7 |
13.4 |
Between 2006 and 2016, the rates of laparotomic and vaginal hysterectomies fell from 76.9% to 23.1%, respectively to 39% to 56.6%. During the same period, the rate of coelio-prepared hysterectomies increased from 0 to 4.3% (Figure 1).
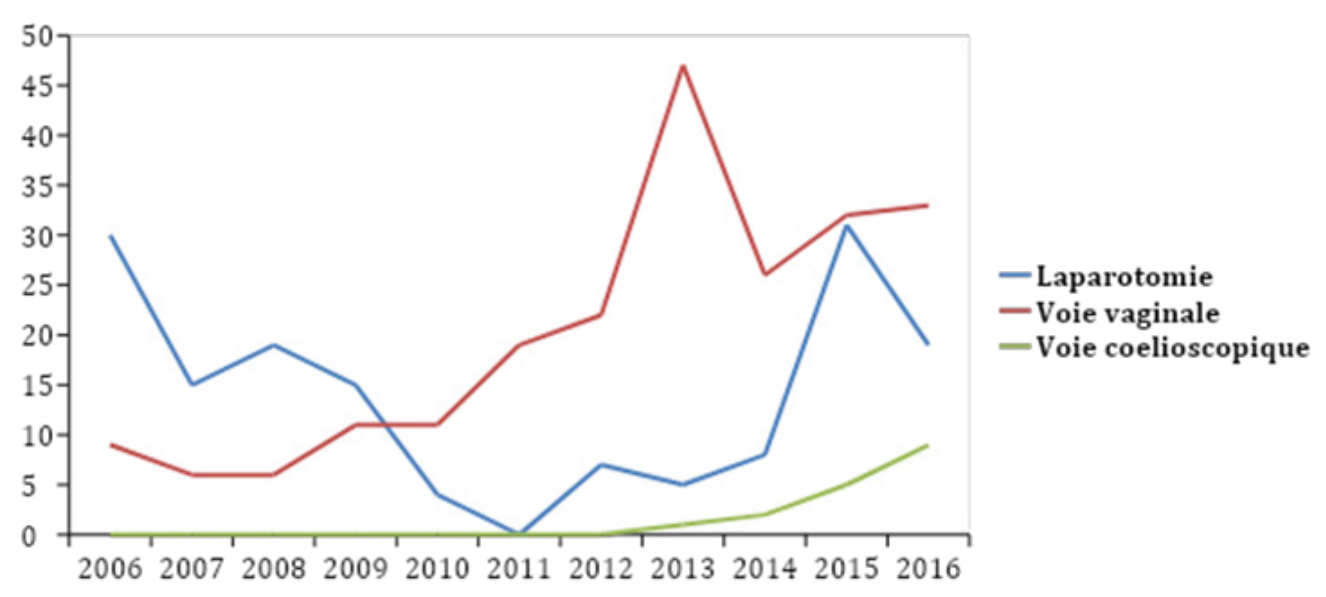 Figure 1: : Evolution of the hysterectomy approach route
Figure 1: : Evolution of the hysterectomy approach routeUterine fibroid was the most common indication in the laparotomy group (71.2%). In the “vaginal route” and “coelioprepared route” groups, the most frequent indications were severe cervical dysplasia (36.9%) and benign endometrial pathology (35.3%), respectively (Table 2).
| Surgery indications | Laparotomy (n=153) |
Vaginal route (n= 222) |
Coelio-prepared (n=17) |
| Uterine fibroids | 109 (71.2%) |
64 (28.8%) |
5 (29.4%) |
| Endometrial pathology (hyperplasia, polyp) | 5 (3.3%) |
10 (4.5%) |
6 (35.3%) |
| Organic ovarian cyst | 14 (9.1%) |
1 (0.4%) |
4 (23.5%) |
| Genitourinary prolapse | 1 (0.6%) |
60 (27%) |
1 (5.9%) |
| Severe cervical dysplasia | 24 (15.7%) |
82 (36.9%) |
1 (5.9%) |
| Adenomyosis | 0 |
5 (2.25%) |
0 |
The data of the surgical intervention (type of anesthesia, operating time, intraoperative complications, associated surgical procedures, average hemoglobin level in the postoperative period (g/dl) and blood transfusion) are summarized in Table 3.
Laparotomy (n=153) |
Vaginal route (n= 222) |
Coelio-prepared (n=17) |
p |
|
| Type of anesthesia | ||||
| Spinal Anesthesia (SA) | 113 (73.8%) |
200 (90.1%) |
0 |
0.005 |
| General Anesthesia (GA) | 40 (26.1%) |
14 (6.3%) |
17 (100%) |
|
| SA converted to GA | 0 |
8 (3.6%) |
0 |
|
| Surgery duration (min.) | ||||
| <60 | 18 (11.7%) |
73 (32.9%) |
0 |
0.002 |
| 60-119 | 102 (66.6%) |
137 (61.7%) |
16 (94.1%) |
|
| ≥ 120 | 33 (21.6%) |
12 (5.4%) |
1 (5.9%) |
|
| Surgery complications | ||||
| Severe hemorrhage | 4 (2.6%) |
2 (0.9%) |
0 |
0.07 |
| Digestive wound | 2 (1.3%) |
1 (0.45%) |
0 |
|
| Bladder wound | 1 (0.65%) |
1 (0.45%) |
0 |
|
| Associated actions | ||||
| Adnexectomy | 13 (8.5%) |
21 (9.45%) |
12 (70.6%) |
|
| Folding of Halban fascia | 0 |
53 (23.9%) |
1 (5.9%) |
|
| Pre-rectum fascia plication | 0 |
15 (6.7%) |
0 |
|
| Average postoperative hemoglobin level (g/dl) | 11.1 |
10.4 |
11.8 |
0.005 |
| Blood transfusion | 3 (1.96%) |
2 (0.9%) |
0 |
|
The complication rate was 3.92% in the “laparotomy” group, 1.35% in the “vaginal route” group and zero in the “laparoscopic route” group. A hospital stay of 3 days was noted in 66.7% of patients in the "vaginal route" group and 88.2% of patients in the "laparoscopic route" group (Table 4).
| Laparotomy (n=153) | Vaginal route (n= 222) | Coelio-prepared (n=17) | p | |
| Post surgery complications | ||||
| Severe anemia | 3 (1.96%) | 2 (0.9%) | 0 | |
| Digestive fistula | 2 (1.31%) | 0 | 0 | |
| Urinary fistula | 1 (0.65%) | 0 | 0 | |
| Acute retention of urine | 0 | 1 (0.45%) | 0 | |
| Duration of hospitalization | ||||
| <3 days | 1 (65.3%) | 8 | 1 (5.9%) | 0.001 |
The frequency of hysterectomies is variously appreciated by African authors. In fact, the frequency recorded in our series was higher than those found in the Republic of Guinea and Côte d'Ivoire, which were 4.3% and 3.2% respectively [2,3]. On the other hand, it was lower than that reported by Nzau [4] in the Democratic Republic of Congo (DRC) (13.34%). This relative variability in the frequency of hysterectomies could be explained by the inclusion criteria, which differ according to the study. However, it constitutes, with the cesarean section, the most practiced surgical intervention in Gynecology-Obstetrics [5]. It was often performed in elderly patients in the pre- or postmenopausal and multiparous period. In our study, the average age of the patients was 51.8 years and the average parity was 5. A similar finding was made by most of the authors [1,6].
The evolution of surgical practices has developed the realization of vaginal hysterectomy with or without laparoscopic assistance. In 1982 Dicker still had almost 70% abdominal hysterectomies and Wilcox another 75% in 1994 [6]. In our series, between 2006 and 2016, the rates of laparotomic and vaginal hysterectomies fell from 76.9% to 23.1% and from 39% to 56.6% and the rate of coelio-prepared hysterectomies from 0 at 4.3%. During the last decade, the approach to hysterectomies has thus evolved in our structure with a drop in laparotomy rates accompanied by an increase in the rates of vaginal and coelio-prepared hysterectomies.
The choice of the first approach for a hysterectomy is not the subject of any consensus and depends on different parameters: the training and the habit of the surgeon, the patient's wish, the anatomical considerations, the history and pathology [7]. In our structure, hysterectomies were performed for a long time by laparotomy because it was the approach first mastered by gynecological surgeons.
In 2008, we received training in vaginal surgery and were introduced to laparoscopic surgery in 2012. This allowed us to develop the practice of hysterectomy by these routes first with all the advantages that they entail. The vaginal route is the route of choice [8-11]. It is beneficial compared to laparotomy for the average length of stay, analgesia, resumption of transit and length of convalescence. In a randomized study of the large uterus, celio-preparation did nothing for the vaginal tract despite certain usual contraindications [11]. The vaginal route would also be less expensive compared to laparoscopy and laparotomy [12]. However, this approach has certain limits or contraindications. These are the large uterus extending beyond the umbilicus, the narrowness of the vulval opening making vaginal access, the uterus fixed, and deep endometriosis impossible [1]. Faced with these situations, coelio-preparation would be an interesting alternative to the vaginal route. It makes it possible to obtain a vaginal excision, whereas a laparotomy would be necessary. The superiority of the coelovaginal route has been confirmed by 4 randomized studies compared to laparotomy in terms of reduction in the average length of stay, post-operative pain and the duration of convalescence. A decrease in dyspareunia has also been observed after laparoscopic hysterectomy by vaginal route compared to hysterectomy by laparoscopic exclusive [13]. Also, annexectomy would be easier by laparoscopic route compared to the vaginal route in case adnexal pathology. In our series, we performed adnexectomy in 70.6% of coelioprepared hysterectomies compared to only 9.45% in cases of vaginal hysterectomy. Despite these numerous advantages, coelio-preparation could expose the patient to a risk of hemorrhagic and urinary complications, particularly in the case of polymyomatous uteri wedged in the cul-de-sac of Douglas which make access to the uterine pedicles difficult. These situations are often encountered in our developing countries where, due to the delay in consultation and diagnosis, we are often required to take care of large polymyomatous uterus far beyond the navel. This would explain why our laparotomy rate, despite the drop recorded, still remains high. In a study carried out in Lille, the authors found 9.3% of indications for abdominal hysterectomies which they considered essential and essential. It involved poor vaginal access and / or a large uterus or the existence of a history of adhesiogenic surgery [6]. The Society of Obstetrics and Gynecology of Canada (SOGC) [14] recommends, for benign gynecological indications, to perform the hysterectomy preferably via the vaginal or laparoscopic approach.
In our series, the indications were dominated by uterine fibroids (71.2%) in the “laparotomy” group, severe cervical dysplasia (36.9%) and uterine fibroids (28.8%) in the “route” groups vaginal ”, benign endometrial pathology (35.3%) and uterine fibroma (29.4%) in the“ coelio-prepared route ”group. This predominance of uterine fibroids in our hysterectomy indications has been noted by other authors. Indeed, Mitsingou [15], in Congo, reported a rate of 36% of hysterectomies for uterine fibroma. In France, Lansac [5] found that fibroids represent 70% of indications for hysterectomies for benign lesions.
In our series, intraoperative complications were more frequent in the “laparotomy” group (4.55%) compared to the vaginal (1.8%) and coelio-prepared (0%) routes without any difference. statistically significant (p=0.07). In the literature, the rates of intraoperative complications vary between 0 and 8.5% [6]. Our complications were dominated by hemorrhages (2.6% in the laparotomy group and 0.9% for the vaginal route). This is explained by the fact that the cases selected for abdominal hysterectomy were more difficult. These were often patients with large polymyomatous uteri or with major surgical history. In the “vaginal route” group, we also recorded a digestive wound (0.45%) and a bladder wound (0.45%). The vaginal route would have fewer complications. Several previous studies have shown decreased morbidity and mortality from vaginal hysterectomy. The complications of vaginal hysterectomy were mainly intestinal [5].
In our series, the length of hospital stay was shorter in the “vaginal route” and “coelio-prepared route” groups compared to the “laparotomy” group with a statistically significant difference (p=0.001). This observation was made by other authors [1,6]. In fact, in the study by Boukerrou [6] in Lille, the average hospital stay was 3.8 +/- 2, 3.9 +/- 1.3 and 6.42 +/- 3.5 respectively in the “vaginal route”, “laparoscopic route” and “abdominal route” groups.
Between 2006 and 2010, the rate of laparotomy hysterectomies fell at the Ouakam Military Hospital in favor of vaginal and coelioprepared hysterectomies. However, there are still indications of abdominal hysterectomy, especially for the myomatous uterus, which was the most frequent indication in our series. Intraoperative complications, which are generally rare, were more common in hysterectomy by laparotomy.

