 Journal of Clinical Anesthesiology Research
PROVIDES COMPLETE AND TIMELY COVERAGE OF ADVANCES IN ALL ASPECTS OF ANESTHESIA AND PAIN MANAGEMENT
Journal of Clinical Anesthesiology Research
PROVIDES COMPLETE AND TIMELY COVERAGE OF ADVANCES IN ALL ASPECTS OF ANESTHESIA AND PAIN MANAGEMENT
Journal of Clinical Anesthesiology Research
PROVIDES COMPLETE AND TIMELY COVERAGE OF ADVANCES IN ALL ASPECTS OF ANESTHESIA AND PAIN MANAGEMENT
Journal of Clinical Anesthesiology Research
PROVIDES COMPLETE AND TIMELY COVERAGE OF ADVANCES IN ALL ASPECTS OF ANESTHESIA AND PAIN MANAGEMENT
Sameer Sethi
Additional Professor, Department of Anaesthesia and Intensive Care, Sector 12, Pgimer, Chandigarh
Correspondence to: Sameer Sethi, Additional Professor, Department of Anaesthesia and Intensive Care, Sector 12, Pgimer, Chandigarh.
Received date: July 16, 2021; Accepted date: August 4, 2021; Published date: August 10, 2021
Citation: Sethi S (2021) Endoscopic Dacryocystorhinostomy in an Elderly Patient With Severe Left Ventricular Dysfunction Under Individualized Monitored Anesthesia Care. J Clin Anesthes Res 2(1): pp. 1-3. doi: 10.52916/jcar214009
Copyright: ©2021 Sethi S. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution and reproduction in any medium, provided the original author and source are credited.
Endoscopic dacryocystorhinostomy is generally performed under general anaesthesia. However, elderly patients with multiple comorbidities can impose significant risk during conduction of general anesthesia. We report safe management of an elderly patient with hypothyroidism and severe left ventricular systolic dysfunction having implantable cardioverter defibrillator planned for endoscopic dacryocystorhinostomy using monitored anesthesia care. Emphasis is given to the specific drug choices and technique of oxygen supplementation along with assisted local anesthesia in this scenario.
Endoscopic dacryocystorhinostomy, Monitored anesthesia care, Ring-Adair-Elwyn (RAE) tube
Endoscopic dacryocystorhinostomy (endoDCR) is generally performed under general anaesthesia. However, elderly patients with multiple comorbidities can impose significant risk during conduction of general anesthesia. We report safe management of an elderly patient with hypothyroidism and severe left ventricular systolic dysfunction having Implantable Cardioverter Defibrillator (ICD) planned for endoDCR using Monitored Anesthesia Care (MAC) [individualized drug choices and technique of oxygen supplementation] with assisted local anesthesia.
An eighty two years-male was diagnosed with left nasolacrimal duct obstruction and was scheduled for left endoDCR. He had undergone coronary artery bypass grafting with three grafts for triple vessel disease three years back. ICD with VVI mode was inserted two years back prophylactically in view of low left ventricular ejection fraction (20-25%). Patient was receiving amiodarone 100 mg OD,aspirin 150 mg OD, dabigatran 110 mg OD and metoprolol 50 mg OD orally. He was detected having hypothyroidism since 5 months and was on tablet levothyroxine 125 µg OD.
During preanesthesia checkup, he had no other complaints except for age related deafness. On examination, airway parameters were normal except for presence of long beard. His pulse rate was 60 bpm and blood pressure was 140/76 mm Hg. His routine blood investigations were within normal limits. Chest radiograph showed presence of ICD generator in left pectoral region and lead in right ventricle. Electrocardiogram revealed prolonged PR interval and T wave inversions in lead II, III, V4- V6. Transthoracic 2D echocardiography documented regional wall motion abnormalities (severe hypokinesia to akinesia) in left anterior descending and right coronary arteries’ territories.
Exercise stress test was negative at a predicted Metabolic Equivalent of Tasks (METs) of 5.7 with no episodes of angina, hypotension, syncope, dizziness, arrhythmia, S3 or rales. No significant ST-T changes were noted during exercise or recovery phase. His recent thyroid function test showed elevated TSH but normal T3 and T4. Tablets aspirin and and dabigatran were discontinued for 5 days and 2 days respectively prior to the surgery.
After discussing with the patient and surgical team, endoDCR was planned under monitored anesthesia care (MAC) with assisted local anesthesia [1]. Patient was advised to continue tablets levothyroxine 125 mcg OD, amiodarone 100 mg OD and metoprolol 50 mg OD even on the day of surgery. He was kept nil per oral for 8 hrs for solids, 2 hrs for clear fluids. The ICD mode was changed to OVO mode (i.e. chamber to be shocked and tachycardia detection functions were disabled) in the preoperative area under continuous vital monitoring. Nasal packing was done using Merocel® soaked with 4% lignocaine and adrenaline solution half an hour prior to shifting inside operation theatre.
In the operation theatre, all standard monitoring was established. Zoll pads were applied on the chest in the anteroposterior position and were connected to defibrillator. IV access was secured with 18G venous cannula on left dorsum and dexmedetomidine infusion was started at 0.8 mcg/kg for 10 minutes followed by 0.5 mcg/kg/hr. Intravenous fentanyl 50 mcg was given slowly. Oxygen was supplemented using modification of a Ring-Adair-Elwyn (RAE) tube kept in the left buccal region (This novel approach has been described by Heard et al. [2] for apneic oxygenation) and connected to the oxygen source at 6 L/ min [2]( Figure 1).
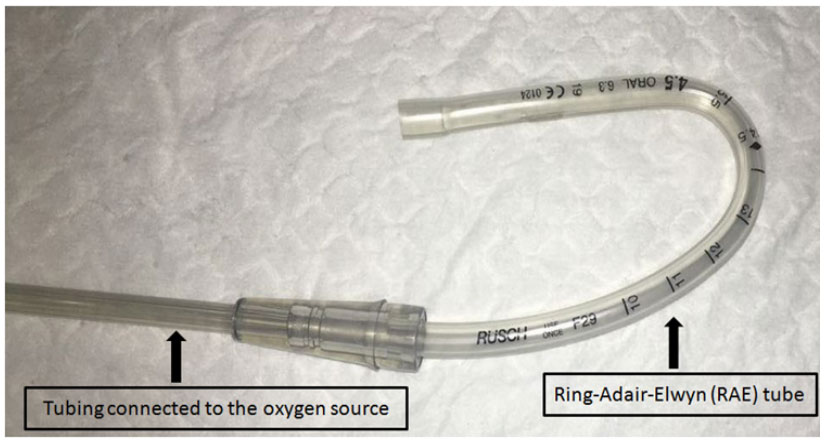 Figure 1: Ring-Adair-Elwyn (RAE) tube for oxygen supply
Figure 1: Ring-Adair-Elwyn (RAE) tube for oxygen supplyPatient was maintaining spontaneous respiration with Modified Ramsay Sedation scale of 2-3. Local anesthetics (2% lignocaine with 1:4,00,000 adrenaline-total volume 3cc) was infiltrated in the lateral wall of the left nostril by the surgeon. Patient had stable vitals throughout the procedure. The total duration of the surgery was 35 min. The ICD was again changed to VVI mode 4 hrs after the surgery. The rest postoperative period was uneventful.
Thorough preoperative evaluation in this case directed to major anesthesia concerns viz, elderly patient with multiple comorbidities (American Society of Anaesthesiologists physical status III), need for individualized sedation regimen so as to maintain hemodynamic parameters along with spontaneous respiration, administration of local anesthetic adjuncts in concentrations suitable for use in ischaemic heart disease patient, requirement of a novel technique for oxygen supplementation during MAC for endoDCR.
Individualised MAC with assisted local anesthesia is acceptable, tolerable and effective technique for endoDCR which enables avoiding the risk associated with general anesthesia especially in elderly patients with multiple comorbidities [1,3,4]. It has shown to have further benefits like less postoperative nauseavomiting, less bleeding and reduced hospital staying cost [3]. General anesthetic agents lead to vasodilation resulting in venous engorgement and surgical bleeding along with hypotension; both of these could have been detrimental in our case.
Intensive monitoring of hemodynamics was initiated in the preoperative period itself as the mode of ICD was changed to OVO mode to avoid effects of electrical interference. Zoll pads were applied in this patient of severe left ventricular systolic dysfunction to avoid delay in delivery of shock whenever needed.
Sedative agents like propofol, midazolam are used during MAC, however, may cause respiratory depression. Dexmedetomidine infusion was the best sedation option in our case as it causes conscious sedation without respiratory depression. We used lower doses of dexmedetomidine to avoid excessive bradycardia and hypotension. Local anesthetic agents were used along with lower concentration of adrenaline to prevent deleterious tachycardia in ischaemic heart disease patient.
Oxygen supplementation is very much important during sedation especially when the airway is not approachable for anaesthetists during the procedure. As the surgery was planned via endonasal approach, facemask or nasal prongs were not feasible options for administration of oxygen in this case. Hence, oxygen was delivered using a tailored technique described by Heard et al for apneic oxygenation in obese patients.2 Machine end of a Ring-Adair-Elwyn (RAE) tube kept in the left buccal region after removing the tube connector and its patient end was connected to oxygen source (6 L/min). This viable alternative was better tolerated by the index patient.
Anesthesiologists must take into account the patient as well as the surgery related factors to provide optimal and safe anesthesia. Monitored anesthesia care is a viable option especially in high-risk patients undergoing endoDCR. Decision regarding choice of drugs e.g., sedatives should be meticulously weighed within the appropriate clinical context. In addition to vigilant monitoring of hemodynamics, this case highlights the selection of individualized method of oxygen supplementation.
Respub Journals an online international open access organization which publishes all kinds of peer reviewed articles in the journals. Respub Journals focus into the fields of Clinical and Medical.

Attribution 4.0 International (CC BY 4.0). With this license readers can share, distribute, download, even commercially, as long as the original source is properly cited.
About ResPub
Responsibilities of Reviewers
Guidelines For Editors
Special Issue
Ethics And Policies
Payment
